
Abstract
Objective
The effectiveness of axillary brachial plexus block (ABPB) performed using peripheral nerve stimulation (PNS) alone was compared with PNS preceded by nerve localization using a pen device, enabling nerve mapping without puncturing the skin.
Methods
Patients undergoing unilateral hand or forearm surgery suitable for ABPB were randomly assigned to receive either PNS alone (pen
Results
Thirty patients were included in each group. The block performance time was longer in the pen + group than the pen
Conclusion
The pen device seems to be a helpful addition to PNS for ABPB, with improved results in terms of block success and patient comfort, but further studies are needed to confirm these findings.
Keywords
Introduction
Brachial plexus block performed via the axillary approach provides analgesia in the forearm and hand. In the axilla, the brachial plexus nerves and axillary artery are found together within a sheath and are close to the skin surface. The anatomical structure of the axilla makes the target nerves more reliably and easily reachable and this method is readily accepted by the patient.1,2
The use of a pen device for nerve localization in axillary brachial plexus block (ABPB) has become accepted in anaesthesia practice, but little has been published concerning its efficacy. This device connects to a peripheral nerve stimulator, enabling nerve mapping without puncturing the skin (Figure 1).
Percutaneous nerve localization pen device.
In this prospective study, ABPB was performed using peripheral nerve stimulation (PNS) alone or preceded by nerve localization with a pen device. The two procedures were compared in terms of the block success rate, block performance time, number of needle insertions and repositionings, complications and patient comfort.
Patients and methods
Patients
Patients undergoing unilateral hand or forearm surgery suitable for ABPB at the Faculty of Medicine, Akdeniz University, Antalya, Turkey, over a period of 8 months between October and May 2011 who were aged between 18 and 65 years and who had an American Society of Anesthesiologists (ASA) status of class I–III were enrolled. Patients who were not suitable for regional anaesthesia were excluded from the study.
The study protocol was approved by the ethics committee of the Faculty of Medicine, Akdeniz University, and written consent was obtained from all study participants.
Patients were premedicated with 1 mg intravenous midazolam. Arterial blood pressure, heart rate, electrocardiogram and peripheral oxygen saturation were monitored throughout the procedure. Patients were randomly divided using a sealed envelope system into two groups to receive PNS via an inserted needle either alone (pen
Procedure in the pen − group
The arm to be operated on was positioned at 90° abduction with the forearm at 90° flexion. The axilla was cleaned with povidone–iodine. Following infiltration of 30 mg lidocaine subcutaneously to provide skin anaesthesia in the area where the block was to be performed, the axillary artery was palpated. A 50 mm Stimuplex® needle connected to a Stimuplex® nerve stimulator (B Braun, Melsungen, Germany) was inserted through the skin and subcutaneous tissue alongside the artery. Electrical stimulation at 2 Hz and 2 mA was applied to the needle. Muscle contractions in the forearm, hand and fingers (stimulated by the musculocutaneous) were observed and the needle repositioned until movements associated with the particular nerve to be blocked were seen. When stimulation of the needle produced the most powerful contractions, the current was reduced to 0.5 mA. If the contractions ceased, the needle was repositioned until muscle contractions occurred at the lower current levels. Confirmation was obtained that the needle was not inside a blood vessel by negative aspiration. Then 70 mg lidocaine was injected via the needle, followed by 150 mg bupivacaine 0.5% in 10 ml normal saline (total volume 40 ml) (single injection technique).
Procedure in the pen + group
The arm to be operated on was positioned and the axilla prepared as for the pen
The pen device was then disconnected from the nerve stimulator and a 50 mm Stimuplex® needle was connected in its place. The needle was inserted through the skin and subcutaneous tissue at the position marked. Electrical stimulation at 2 Hz and 2 mA was applied to the needle. Muscle contractions in the forearm, hand and fingers were observed and the needle repositioned until movements associated with the particular nerve to be blocked were seen. When stimulation of the needle produced the most powerful contractions, the current was reduced to 0.5 mA. If the contractions ceased, the needle was repositioned until muscle contractions occurred at the lower current levels. Confirmation was obtained that the needle was not inside a blood vessel by negative aspiration. Then 70 mg lidocaine was injected via the needle, followed by 150 mg bupivacaine 0.5% in 10 ml normal saline (total volume 40 ml) (single injection technique).
Assessment of procedure
The block performance time, defined as the time between palpation of the axillary artery to the time when the needle was removed, was measured by an assistant using a chronograph. In addition, the total number of times the needle was withdrawn through the skin (needle insertion count) or repositioned without withdrawal (needle passage count), the duration of the operation, and the need for any additional intraoperative sedation or local anaesthesia to the surgical area were recorded by the anaesthetist, who was not blinded to the procesure.
Evaluation of block success
To assess sensory block in the operation area, a pinprick test on all four terminal branch areas was conducted every 5 min following the injection of local anaesthesia. The result was scored on a scale from 0 to 2, where 2 represented total loss of both pain and touch (complete block), 1 represented loss of pain but not touch (partial block), and 0 represented persistence of both pain and touch (no block).
A modified Bromage scale 3 was used to perform motor block assessment every 5 min following the injection of local anaesthesia. The result was scored on a scale from 0 to 3, where 0 represented absence of movement in the upper extremity, 1 represented the presence of movement in the fingers only, 2 represented the presence of flexion in the wrist, and 3 represented the presence of flexion in the elbow.
Evaluation of block success.

Overall block success was defined in terms of the need for additional intravenous sedation or local anaesthesia to the surgical area. No requirement for additional intravenous sedation or local anaesthesia was defined as complete block success and was assigned a score of 0. The need for additional sedation was assigned a score of 1, and the need for additional local anaesthesia and additional sedation was assigned a score of 2; a score of 1 or 2 was defined as assisted block success.
In addition, the need for intraoperative analgesia (50 µg fentanyl intravenously) was scored at 60 and 90 min from the beginning of the block procedure
Evaluation of pain
Pain in the surgical area and pain related to the block procedure were evaluated using a visual analogue scale (VAS) ranging from 1 to 10.
To assess pain in the surgical area, patients were asked to score the pain before commencing the surgical procedure, at 5 min and 10 min following local anaesthesia administration for axillary block, at 10 min intervals for 1 h during surgery, then at 30 min intervals for 150 min, and at the end of the operation.
To assess pain related to the block performance, patients were asked to score the pain felt in the axilla due to needle entry and drug administration.
Patient satisfaction and complications
At the end of the operation, all patients were asked whether or not they would be happy to undergo the same anaesthesia procedure again in the future.
Vascular complications (arterial or venous puncture), neurological complications, complications in the injection area (haematoma or infection), local anaesthetic toxicity/allergic reactions and any other complications were recorded.
Statistical analyses
For our sample size (n = 30 in each group), with a significance level of 0.05 and effect size of 0.55, post hoc analysis showed a power of 0.73. Results were expressed as frequencies, percentages or means ± SD. Pearson’s χ2 or Fisher’s exact test were used to establish relationships between categorical data, the Mann–Whitney U-test or Student’s t-test were used to analyse differences between independent measurements, and the Wilcoxon signed rank test was used in the analysis of differences between measurements recorded at different times. All statistical analyses were performed using SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA). A P-value of <0.05 was considered to be statistically significant.
Results
Characteristics of patients undergoing axillary brachial plexus block performed using peripheral nerve stimulation with (pen + group) or without (pen − group) the use of a pen device for nerve localization.

Data presented as mean ± SD or number of patients.
No statistically significant between-group differences (P ≥ 0.05) using Student’s t-test (age, body mass index), Pearson’s χ2 test (sex) or the Mann–Whitney U-test (duration of operation).
Block performance time and needle insertion and passage counts in patients undergoing axillary brachial plexus block performed using peripheral nerve stimulation with (pen + group) or without (pen − group) the use of a pen device for nerve localization.
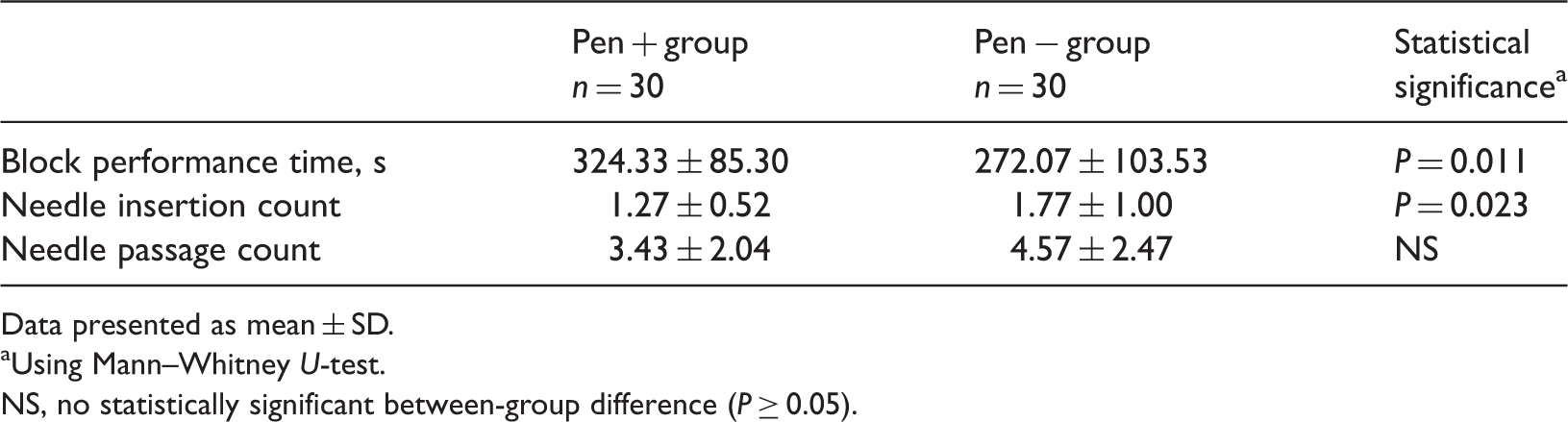
Data presented as mean ± SD.
Using Mann–Whitney U-test.
NS, no statistically significant between-group difference (P ≥ 0.05).
Overall block success score in patients undergoing axillary brachial plexus block performed using peripheral nerve stimulation with (pen + group; n = 30) or without (pen − group; n = 30) the use of a pen device for nerve localization.
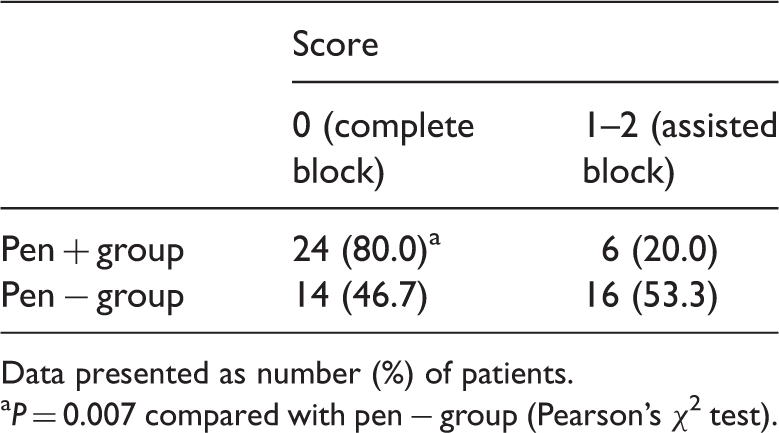
Data presented as number (%) of patients.
P = 0.007 compared with pen − group (Pearson’s χ2 test).
Intraoperative analgesic score at 60 and 90 min in patients undergoing axillary brachial plexus block performed using peripheral nerve stimulation with (pen + group; n = 30) or without (pen − group; n = 30) the use of a pen device for nerve localization.

Data presented as number of patients; no data is given for patients whose duration of operation was <60 or 90 min, respectively.
P = 0.019 compared with pen − group (Pearson’s χ2 test).
Preoperative and 60 min visual analogue scale (VAS) scores for pain in the surgical area in patients undergoing axillary brachial plexus block performed using peripheral nerve stimulation with (pen + group; n = 30) or without (pen − group; n = 30) the use of a pen device for nerve localization.
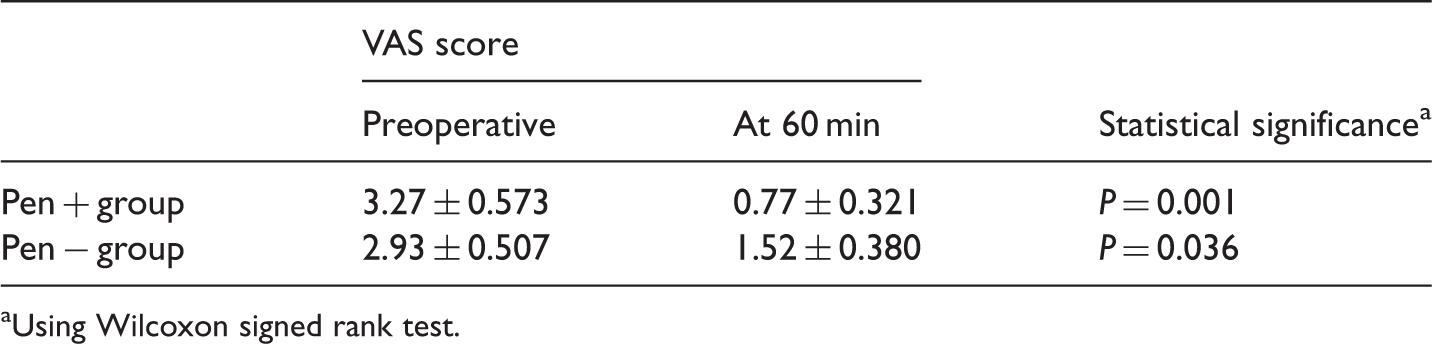
Using Wilcoxon signed rank test.
When compared using the Mann–Whitney U-test, there was no significant difference in the VAS score for pain in the axilla due to needle entry and drug administration between the two groups (P = 0.257, data not shown). In addition, the percentage of patients who would be happy to undergo the same anaesthesia procedure again in the future was not significantly different in the two groups (28/30 in the pen + groups vs 23/30 in the pen − group, Fisher’s exact test, P = 0.145) (data not shown).
Arterial puncture occurred in one patient from each group, and venous puncture occurred in three patients in the pen + group and seven patients in the pen
Discussion
Brachial plexus block is a frequently used method of regional anaesthesia. Blocking the brachial plexus in the axilla was first reported by Halsted in 1884 4 and its clinical use was described by Hirschel 5 in 1911. Its popularity grew following the publication of an article by Burnham 6 in 1959.
Ultrasonography gives the opportunity to observe the contents of the axilla for more accurate positioning of the needle and local anaesthetic distribution, increasing block quality and decreasing the amount of local anaesthetic required.2,7,8 However, ultrasonography is not always available in operating rooms. 9 The use of peripheral nerve stimulation for nerve localization was first reported in the 1950s.10,11 This method is invasive and may require multiple needle passages in order to obtain the desired motor or sensory response to electrical stimulation. In a study by Casati et al. 12 involving 60 patients, ABPB carried out using ultrasonography or PNS for nerve localization was compared in terms of the time to block onset, block success, procedure-related pain and patient satisfaction; both methods had similar success rates, patient satisfaction and complication rates. Koscielniak-Nielsen et al. 13 reported that pain scores at the time of multiple needle passages were lower than those associated with electrical stimulation or anaesthetic injection. On the other hand, Bloc et al. 14 demonstrated that ultrasonography-guided methods were associated with greater patient satisfaction and comfort than PNS.
In the present study, ABPB performed using PNS preceded by nerve localization with a pen device was compared with PNS alone. A number of articles have shown that pain at the time of peripheral nerve block is mostly associated with multiple electrolocalizations or injections.15–17 Sia et al.
18
reported that the cause of major pain at the time of the procedure was the withdrawal and repositioning of the needle, whereas Standl and Burmeister
19
correlated patient dissatisfaction with repeated muscle contractions and needle movements. In a study of peripheral block performed on 3996 patients using PNS, a high success rate of up to 94% was obtained; however, 74% of the patients said that they would prefer a different anaesthetic method next time, mainly due to discomfort during performance of the block.
20
In the present study, the needle insertion count was significantly lower in the pen + group compared with the pen
During nerve localization in PNS, the needle may need to be repositioned many times. Repeated insertion and withdrawal of the stimulation needle and its repositioning in the subcutaneous tissue may alter the pain resistance of the patient and additional analgesia/sedation may be necessary during the procedure. 12 In the present study, there was a significantly smaller needle insertion count and a significantly decreased need for intraoperative analgesia in the pen + group. Further studies are needed to compare the effects of non-invasive methods such as the pen device and ultrasonography with those of PNS on patient satisfaction.
In a review by De Andrés and Sala-Blanch
21
that compared PNS with other methods, it was reported that nerve stimulation was not superior to other nerve localization methods despite its numerous advantages. In a study by Goldberg et al.,
22
the techniques of transarterial fixation, paraesthesia and nerve stimulation were compared and shown to have similar success rates. However, only single doses of anaesthesia were used, whereas multiple injections may have been more suitable.
23
In a study by Baranowski and Pither
24
comparing ABPB using multiple injections guided by nerve stimulation or paraesthesia, no difference in success rates was found between these techniques. However, the number of patients in the PNS group was low and there were variations in the number of nerves detected.
23
In contrast, a study of 100 patients comparing multiple injections guided by nerve stimulation or paraesthesia reported shorter performance times, faster onset times and higher complete block rates, particularly in the radial and musculocutaneous nerves, in the neurostimulation group.
18
In the present study, complete block rates approaching 50% were obtained in the pen
Although there is a theoretical risk of needle trauma to nerves in ABPB, a number of studies have reported either no neurological complications15,25 or low rates of temporary neurological dysfunction.20,26 Therefore, it seems that the use of stimulation needles is not associated with increased nerve damage. In the present study, no nerve damage was observed in either group. A small number of arterial and venous punctures occurred, but the rate of vascular complications was not significantly different in the two groups. However, ultrasonography has been shown to superior to PNS in terms of vascular complications. 27
In contrast to studies that have compared different nerve identification methods, the present study used the same fundamental approach in both groups (PNS) but this was facilitated by use of the pen device in the pen + group. As the pen device is a recent development, very little has yet been published concerning its use. However, there are a number of studies of ABPB conducted using other types of percutaneous electrode guidance (PEG) that resemble the pen device in that they are simple and non-invasive. The use of modified electrocardiography electrodes or isolated needles has been shown to decrease the needle exploration time and needle passage count and to reduce procedure-related pain.28,29 The success rate of block performed following PEG using an insulated needle was reported as >85% by Capdevila et al. 9 This is similar to the block success rate of 80% using the pen device in the present study.
These studies with PEG suggest that supporting techniques such as the pen device used in the present study could improve results in terms of block performance time and patient satisfaction. However, Wegener et al. 30 have suggested that the pen device is not a reliable method compared with high-resolution ultrasonography for nerve localization. Theoretically, the pen device works on the principle that the threshold current needed to stimulate the nerve is dependent on the distance from the electrode to the nerve. 31 However, since electrical resistance in biological tissues demonstrates variability,32,33 this correlation is not always linear. 34 Thus the pen device is unlikely to be able to provide localization information as reliably as a method that generates real-time images such as ultrasonography.
The results of the present study, together with those reported in the literature for other types of PEG, suggest that use of the pen device can increase block success with PNS. However, further clinical studies with a greater number of subjects are needed to confirm these findings.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.