
Abstract
Centipede bites are reported in many parts of tropical and subtropical countries, such as India. Centipede envenomation produces significant local symptoms, with pain being the most prominent symptom. The emergency department (ED) plays a crucial role in managing the victims through appropriate pain management and control of other local and systemic symptoms. Nonopioids and weak opioids, along with local measures, are often employed, but the intense pain is often refractory to these conventional techniques. Regional anesthesia has numerous benefits over these traditional measures, such as avoidance of polypharmacy and its consequent systemic adverse effects, excellent quality of pain control, and decreased need or avoidance of hospital admission. The applications of regional anesthesia have recently increased tremendously in the ED but are unreported for the management related to centipede bites. We report a case of centipede bite in which conventional analgesics did not help, and the pain was successfully managed by low-volume selective sensory peripheral nerve block.
Introduction
Centipede bites (CBs) are reported in many parts of tropical and subtropical countries, such as India.1,2 The venom of centipedes contains a diverse mixture of toxins, including neurotoxins and peptides. 3 The envenomation from CBs is rarely life-threatening but produces significant local symptoms.1,2 Acute moderate-to-severe pain at the bitten site is the most typical symptom after a venomous CB due to the interaction of venom constituents with the pain pathways.1,3-5 Acute local pain may last for 30 min to 72 h after the bite. 1 Acetaminophen, weak opioids such as tramadol, or injectable nonsteroidal anti-inflammatory drugs are mostly employed for pain management but often produce inadequate analgesia.1,4 Ultrasound-guided peripheral nerve blocks (PNBs) are gaining popularity in emergency departments (EDs) for various traumatic and procedural pain management interventions.6,7 Here, we report a patient with a CB who presented to our ED with complaints of severe pain and was successfully treated with an ultrasound-guided selective superficial radial nerve (SRN) block.
Case Report
A 50-y-old woman presented to our ED 45 min following a CB on the base of the left middle finger while working at home. She complained of redness, swelling, and excruciating pain. Her pain score on the Numerical Rating Scale (NRS) was 6/10 at the time of presentation. Her vitals were normal except for tachycardia attributed to pain. On examination, redness was noted over the base of the left middle finger, with swelling extending to the dorsum of the hand. Her complete blood count was normal except for a total leucocyte count of 16,000/mm3. Wound cleaning was done, and tetanus immunization was given. The pain was treated with intravenous acetaminophen (1000 mg) and an injection of diclofenac (75 mg), and she was discharged after observation for 2 h. Six hours after the bite, she returned to the ED with increased pain (NRS score, 10/10) and swelling (Figure 1). The left SRN block was performed in the midforearm under ultrasound guidance with 2 mL of 0.75% ropivacaine (15 mg) using a linear transducer probe (SonoSite EDGE II; SonoSite, Inc, Bothell, WA) by an in-plane technique, which reduced her NRS score to 2/10 within 5 min. The sensory innervation of the SRN, probe position, normal sonoanatomy, and sonoanatomy with hydro-dissection around the SRN are depicted in Figure 2. The effect of the nerve block wore off after 15 h, after which she had an NRS score of 4/10. She was further managed with tablet acetaminophen (650 mg), diclofenac (50 mg), and serratiopeptidase. The patient was monitored for limb swelling in the ED for 6 h after the nerve block and followed up after discharge for any other complications. The local pain subsided in 1 wk, and the swelling subsided within 2 wk without local tissue necrosis. Written informed consent was obtained from the patient for the PNB and to publish clinical images and case details.
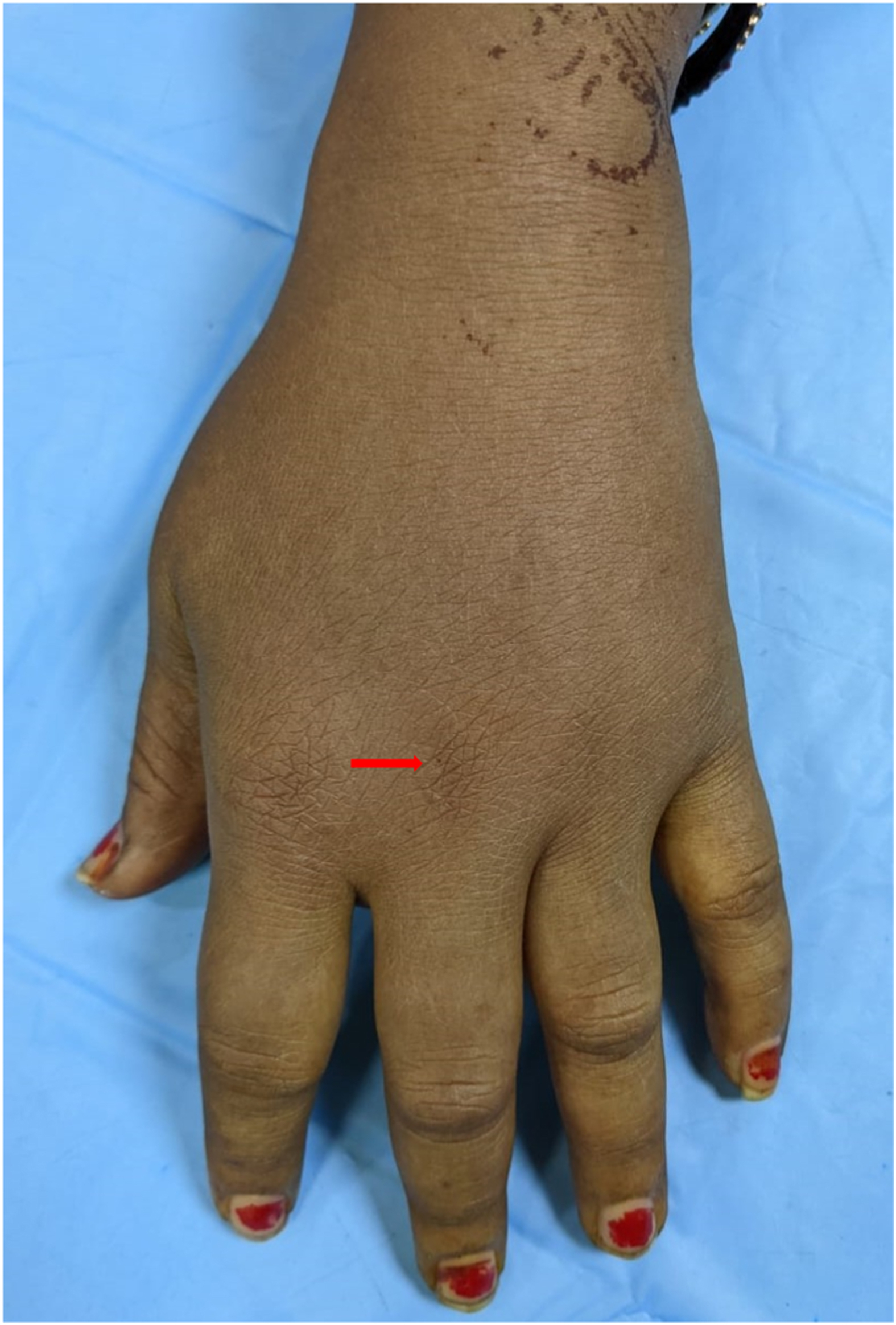
Image showing a centipede bite at the base of the middle finger (arrow) of the left hand with mild swelling of the dorsum of the left hand.
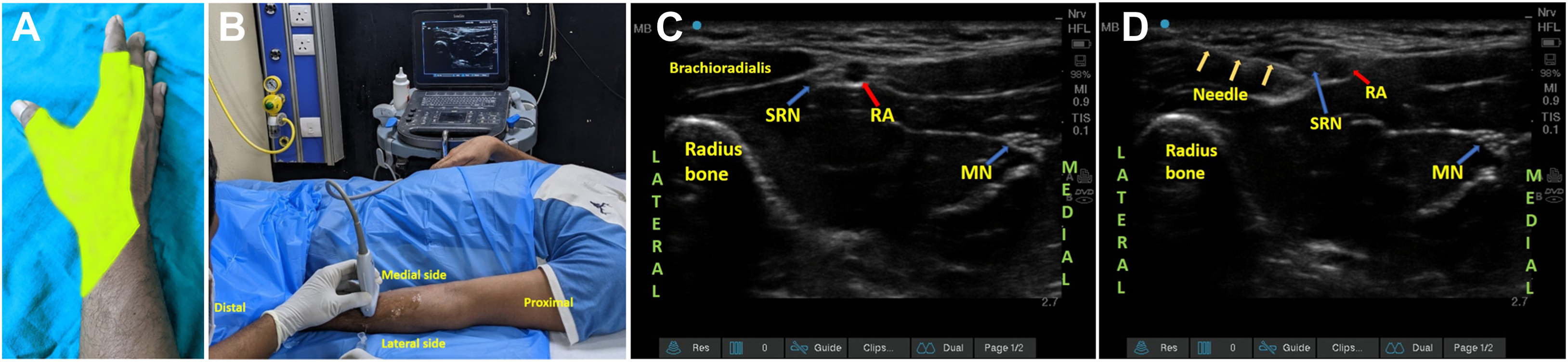
A, Sensory distribution of the SRN in the dorsum of the hand. B, Probe position for SRN block in the midforearm. C, Sonoanatomy of the SRN. D, Sonoanatomy showing needle through the fascial plane (triple arrow) from the lateral side and hydro-dissection and local anesthetic drug deposition around the SRN. MN, median nerve; RA, radial artery; SRN, superficial radial nerve.
Discussion
Centipedes belong to a group of predatory venomous arthropods, with the most significant species being Scolopendra (Figure 3). 1 Most venom constituents are a diverse mixture of proteins, peptides, and enzymatic and nonenzymatic compounds, including metalloproteases, phospholipases, and hydrolases.3,8 Among the various symptoms of envenomation, local pain, swelling, and redness are the most common.1,3 Most patients visit healthcare settings to manage these local symptoms, particularly excruciating pain. 1 -3 The mechanism of venom-induced pain is complex and directly related to the venom constituents and is not vividly reported in the literature.3,8 The pain severity varies according to the quantity and biochemical composition of the injected venom and is species-specific for CBs. 3 Inadequate pain relief leads to patient discomfort and suffering and may predispose patients to long-term sequelae, such as complex regional pain syndrome. 5 Our patient returned from home complaining of rebound pain after intravenous and oral analgesia. Acetaminophen, nonsteroidal anti-inflammatory drugs, or weak opioids such as tramadol are mostly employed for pain management but often produce inadequate analgesia.4,5 Local lignocaine infiltration is a recommended treatment method. Its application is, however, limited by local edema and erythema, which reduce its effectiveness and add to patient discomfort. 1 Most CBs occur in the extremities, such as the foot and hands.1,3 Immersion of bite sites in hot water is another reported method for pain management of CBs as heat denatures the heat-liable venomous proteins.1,3,4 This modality is ineffective in many patients, however; some may develop increasing swelling and erythema, exacerbating the discomfort. 4 Chaou et al 4 compared the analgesic efficacy of ice packs, hot water immersion, and intramuscular ketorolac injection to treat centipede envenomation and concluded that all had a similar effect on pain scores. However, the analgesia efficacy was short-lived, and the author reported that 3 of 60 patients revisited the ED with progression of local symptoms. 4 Thumtecho et al 5 reported complex regional pain syndrome in a patient with a CB who presented to the ED with hyperalgesia and allodynia 2 wk after the CB. Hence, appropriate management of acute local pain is paramount to prevent such delayed complications.

Image of centipede species Scolopendra found in the Asian subcontinent.
Earlier reports documented the safety and efficacy of ultrasound-guided selective PNBs for procedural pain relief and snake bite pain management in the ED.7,9-11 However, its use in the pain management of CBs is not documented to date. The SRN is a branch of the radial nerve along with the posterior interosseous nerve. 11 Ultrasound-guided SRN block is a simple technique of acquiring analgesia on the dorsum of the hand by blocking the nerve in the middle third of the forearm. 11 At this position, the nerve lies lateral to the radial artery in a neurovascular sheath, and the cephalic vein is superficial to the nerve. 11 The nerve is easily identified and reached with a standard 25-mm, 24-gauge hypodermic needle under ultrasound guidance from the lateral side to deposit the drug near the nerve. 11 The selective sensory block avoids the distressing motor blockade associated with regional blocks. Prolonged analgesia for up to 18 h can be achieved with a low dose (1.5–2 mL) of long-acting local anesthetic, such as 0.75% ropivacaine. 10 Ropivacaine is preferable in ED settings because of its better safety profile and reasonably longer duration of analgesic effect. 6 The site of the block is away from the site of the bite, thus adding to the patient’s cooperation.
To conclude, selective SRN block can be a credible choice for pain management following CBs in the hand or fingers. The nerve is easy to identify and block under ultrasound guidance.
Footnotes
Acknowledgments
The authors are pleased to acknowledge Shri Suvendu Mallick, Head of the Odisha snake helpline, for providing us the image of the centipede belonging to the species Scolopendra.
Author Contributions: conceptualization (CRM); methodology (CRM, RVR, AG); data curation (RVR); resourses (SB); software (CRM, AG, SB); investigation (CRM, RVR, AG); formal analysis (CRM); supervision (CRM); project administration (CRM); visualization (RVR, AG); writing of the original draft of the manuscript (CRM, RVR, SB); review and editing of the manuscript (RVR, AG, SB); reading and approval of the content of the final manuscript (CRM, RVR, AG, SB).
Financial/Material Support: None.
Disclosures: None.