
Abstract
Hematotoxic snake bite is a leading cause of mortality in South India. However, it is rare for the emergency physician to encounter a patient with trauma associated with snakebite. Management of such a patient differs substantially from the routine management of either a trauma patient or a snakebite victim. A 59-y-old man was bitten by a snake, after which he lost consciousness, fell, and sustained facial trauma. He was rushed to the emergency department within 30 min and was discovered to have ongoing oromaxillofacial bleeding. His respiratory distress and gasping respirations warranted orotracheal intubation and ventilation. He was treated with anti-snake venom and underwent viscoelastometry-guided transfusion to correct coagulopathy. Hemostasis was achieved after administration of tranexamic acid and bilateral posterior nasal packing. Imaging studies revealed craniomaxillofacial trauma with intracranial hemorrhage. He underwent a delayed mandibular repair. Judicious, guided fluid management, adequate nutrition, and prompt weaning off the ventilator allowed early discharge of the patient from the hospital. The minimal weakness present in his left lower limb at the time of discharge had improved by the time of follow-up. This report shows the utility of early and rapid anti-snake venom in envenomated victims with coagulopathy. The role of cryoprecipitate, tranexamic acid, and viscoelastometric testing needs further exploration in specific hematotoxic snakebites.
Introduction
In recent years, snakebite has been gaining recognition as a “disease.” 1 In developing countries, the management of snakebite victims is governed by cost-effective strategies. Even though snakebite has been comprehensively discussed in the literature, cases with concurrent complications such as trauma are seldom addressed. Such complicated cases occur largely in the rural setting. Consequently, the eventual morbidity and mortality are not reported.2,3 The scarcity of literature on the subject and the lack of availability of evidence-based guidelines result in varying practices in the use of anti-snake venom (ASV) and blood product in treating snakebite.4,5
Through this case report, we intend to review the evidence behind rapid administration of ASV and blood products, the rapid correction of coagulopathy, the role of global coagulation assays, and use of tranexamic acid (TXA) in snakebite victims with concurrent trauma and coagulopathy.
Case report
A 59-y-old man was brought to the emergency department after snakebite. He was bitten on his feet at 0800 while walking through a bushy area (Figure 1A). The culprit snake was never identified. His wife, who was with him at the time, witnessed him lose consciousness within 5 min after the bite and fall into a pit nearly 1.5 m deep.

Clinical images. (A) Bite mark noted over the lateral aspect of the right foot with a subtle ecchymotic patch toward the heel (arrow mark pointing at the puncture wound). (B) At admission he was gasping, with severe oromaxillofacial bleeding and a Glasgow Coma Scale score of 4-E1V2M1. (C) After intubation: bilateral posterior nasal packing done with Foley catheter. Through and through lacerated wound on the lower jaw with ongoing bleed sutured soon after. (D) Two hours later, coagulopathy improved, with no active hemorrhage. (E) After extubation: confused, but obeying commands. No coagulopathy. (F) Conscious and well oriented. Multiple contusions present over the body, now resolving.
At 0830, he was brought to the emergency department gasping, with severe bleeding from the mouth and nose impeding normal respiratory efforts. This warranted drug-assisted orotracheal intubation (Figure 1B). A laceration on the lower jaw, chemosis, and purpuric contusions over his left shoulder were noted.
At 0840, polyvalent ASV was started (10 vials) as per the department hematotoxic envenomation protocol (Figure 2). Breathing and ventilation was optimized, but pulsatile bleeding from the nose continued and could not be controlled with direct pressure or cold compress. The initial blood sample drawn showed features suggestive of consumptive coagulopathy (prothrombin time >180 s [normal 10–14 s]; activated partial thromboplastin time >180 s [normal 25–35 s], serum fibrinogen <10 mg·dL-1 [normal 200–400 mg·dL-1]) with normal liver and renal function. Rotational thromboelastometry (ROTEM) showed no clot formation (Figure 3A).
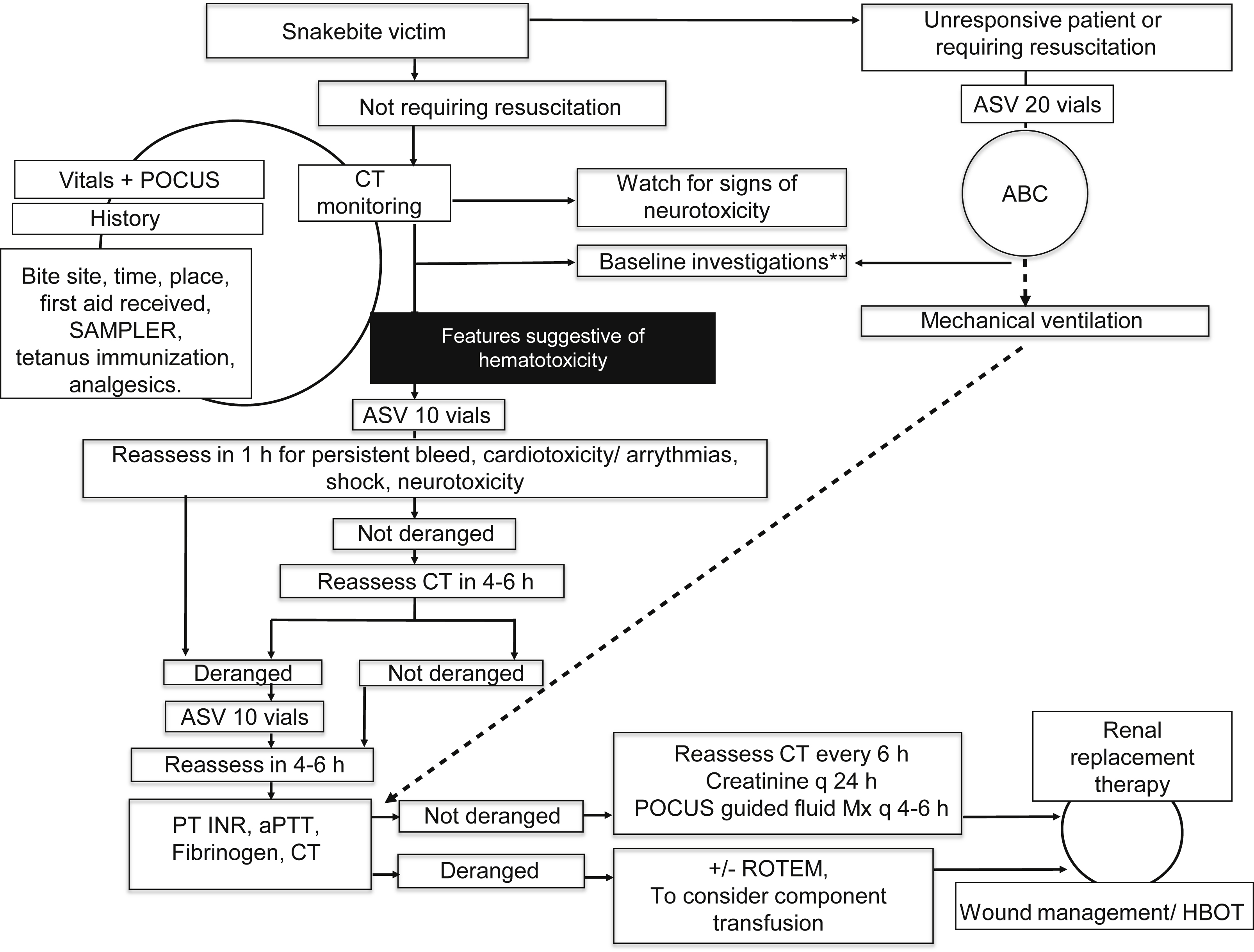
Institute (JMH ED a ) snakebite management protocol. aPTT, activated partial thromboplastin time; ABC, airway, breathing, and circulation; ASV, anti-snake venom; CT, clotting time (modified Lee and White test); CBC, complete blood count; HBOT, hyperbaric oxygen therapy; INR, international normalized ratio; JMH ED, Jubilee Mission Hospital Emergency Department; Mx, management; POCUS, point of care ultrasound; PT, prothrombin time; ROTEM, rotational thromboelastometry; SAMPLER, signs and symptoms, allergies, medications, past medical history, last meal, events leading to the present illness, and risk factors. Baseline investigations include complete blood count, creatinine, PT INR, aPTT. Additional blood tests are sent at admission as per the discretion of the treating clinician on a case by case basis. a JMH ED protocol reproduced with permission.
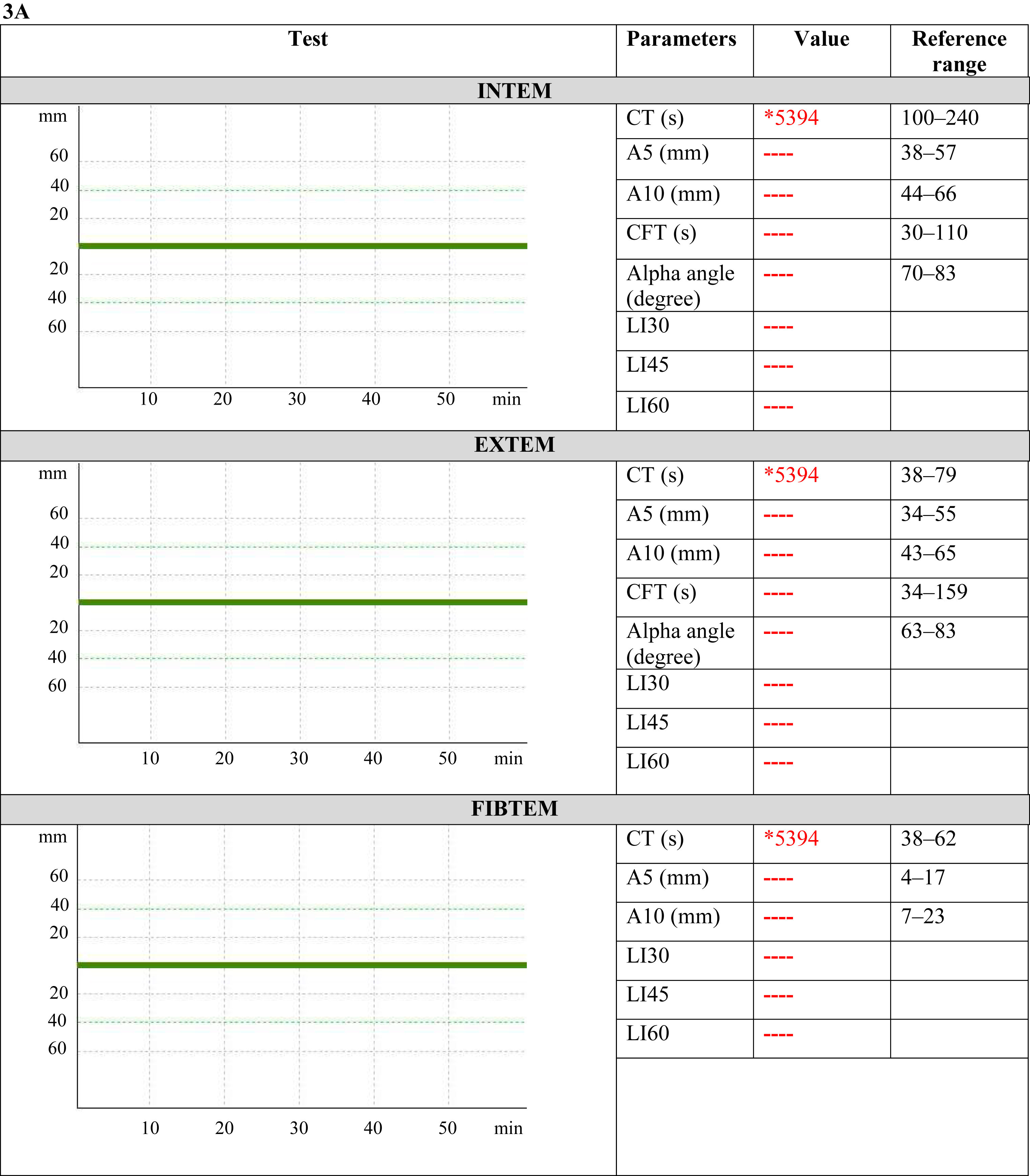
Serial ROTEM. (A) ROTEM at presentation (sample time: 0835) CTEXTEM, CTINTEM and CTFIBTEM showing no clot formation. (B) ROTEM after 20 vials of ASV, 10 units cryoprecipitate, and 1 unit of packed red blood cell transfusion (sample time: 0920) showed clot formation, with CTEXTEM and CTFIBTEM slightly prolonged with a lysis index at 60 min, 95%. (C) ROTEM after blood transfusion and tranexamic acid injection (sample time:1035) showed normal clot formation, with no lysis of clot. Three ROTEM tests were performed: extrinsically activated assay with tissue factor (EXTEM), intrinsically activated test using kaolin (INTEM), and extrinsically activated test with tissue factor and the platelet inhibitor cytochalasin D (FIBTEM). For the ROTEM assays, the following variables were measured: clotting time (CT [s]), time taken from the start of the test to the time for clot until 2 mm amplitude is reached; alpha angle (alpha) is the angle between the central line and a tangent to the curve through 2 mm amplitude point, measured in degrees; clot formation time (CFT [s]), time taken for clot of 20 mm amplitude after CT; A5, A10 (clot amplitude at respective min after the end of CT); and maximum clot firmness (MCF [mm], the maximum amplitude reached during the test). Finally, the lysis index at 60 min (LI60 [%], clot firmness 60 min after CT as percentage of MCF). CTEXTEM, CTINTEM, and CTFIBTEM denote clotting time on EXTEM, INTEM, and FIBTEM, respectively.
At 0855, with the first dose of ASV complete, a persistent tendency to bleed was noted; hence, the second dose of ASV (10 vials) was started in congruence with the protocol and was administered over the next 15 min.
On reassessment at 0915, the patient had ongoing maxillofacial bleed. Point of care ultrasound showed a hyperdynamic heart with an exaggerated phasic variation of inferior vena cava with respiration, warranting fluid replacement. One unit of O-negative packed red blood cells was commenced, along with 3 units of fresh frozen plasma (FFP) to partially compensate for the volume loss, correct coagulopathy, and improve tissue oxygenation. Crystalloid or colloid transfusions were strictly restricted. He was also given 1 g of TXA and 10 units of cryoprecipitate.
On repeat ROTEM, clot formation was seen but with a slightly prolonged CTEXTEM and CTFIBTEM (Figure 3B).
The laceration on the lower jaw was sutured. A Foley catheter was inserted through each nostril and bulb inflated with air to achieve hemorrhage control (Figure 1C).
By 0930, the decision was made to stop further transfusion because clinically the bleed had decreased, and ROTEM findings were reassuring (Figure 3B).
Computed tomography imaging of the head revealed a thin intraventricular hemorrhage, right subcondylar mandibular fracture with temporomandibular dislocation, and left maxillary sinus fractures in the anterior and posterior walls with pneumo-orbit on the same side (Figure 4). Computed tomography imaging of the chest showed consolidated right lower lung zones with thin pleural effusion. Following this, the patient was transferred to the medical intensive care unit (Figure 1D) where a repeat ROTEM demonstrated a stable clot formation (Figure 3C).
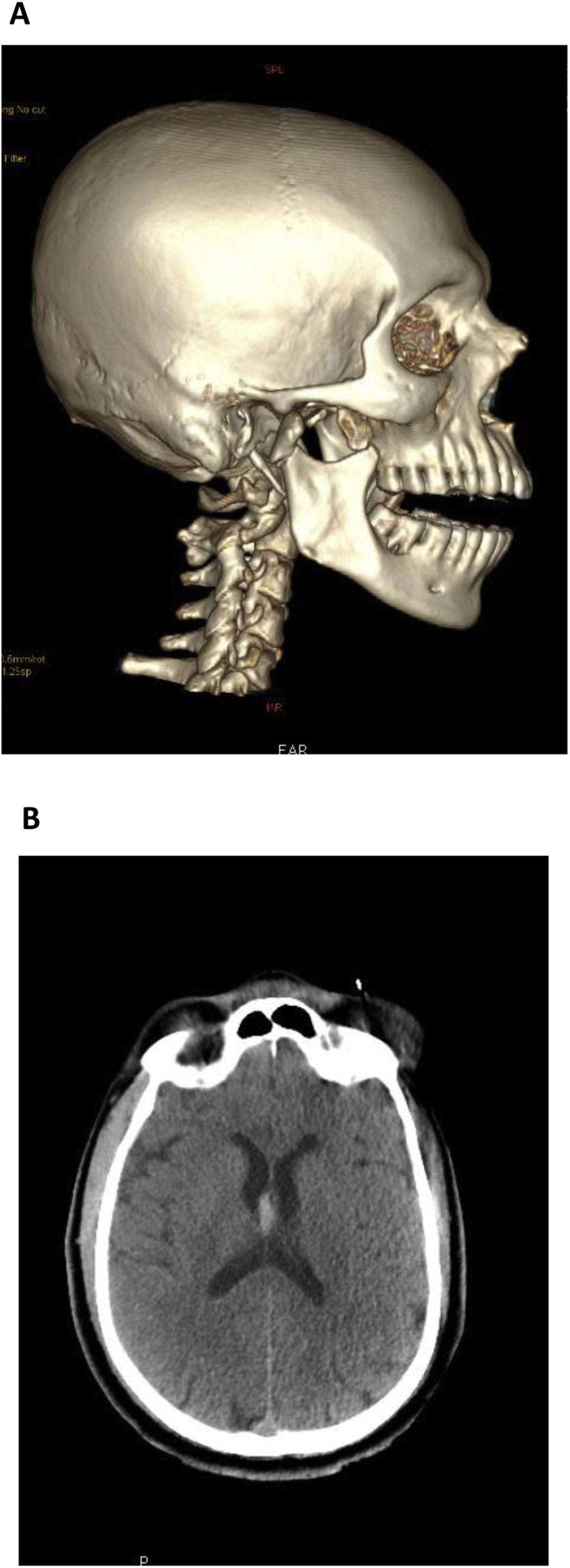
(A) Right subcondylar mandibular fracture with temporomandibular joint dislocation. (B) Axial CT images showing intraventricular hemorrhage.
All intravenous fluid was administered, while monitoring his inferior vena cava distensibility (target: 50–80%) and hourly urine output. Coagulopathy improved (Tables 1 and 2), and the posterior nasal pack was removed after 12 h. His sensorium improved progressively over the next 24 h after cessation of sedatives. He was extubated 36 h after admission (Figure 1E). The dislocated mandibular fracture was fixed 7 d later, and intracranial hemorrhage was managed conservatively (Figure 1F). He had residual weakness of his left lower limb, which gradually improved over the course of 1 mo with physical rehabilitation therapy. Modified Rankin score at discharge was 2, which improved to 0 by the end of 1 mo (Figure 5).
Blood investigations (Day 1)
APTT, activated partial thromboplastin time; ctrl, control; INR, international normalized ratio; LDH, lactate dehydrogenase; PT, prothrombin time.
Reference values are affected by many variables, including the patient population and the laboratory methods used. The ranges used at Jubilee Mission Medical College & Research Institute are for adults who do not have medical conditions that could affect the results. They may therefore not be appropriate for all patients.
Investigation not done or result unavailable.
Blood investigations (Days 2–13)
APTT, activated partial thromboplastin time; ctrl, control; INR, international normalized ratio; PT, prothrombin time.
Reference values are affected by many variables, including the patient population and the laboratory methods used. The ranges used at Jubilee Mission Medical College & Research Institute are for adults who do not have medical conditions that could affect the results. They may therefore not be appropriate for all patients.
Investigation not done or result unavailable.
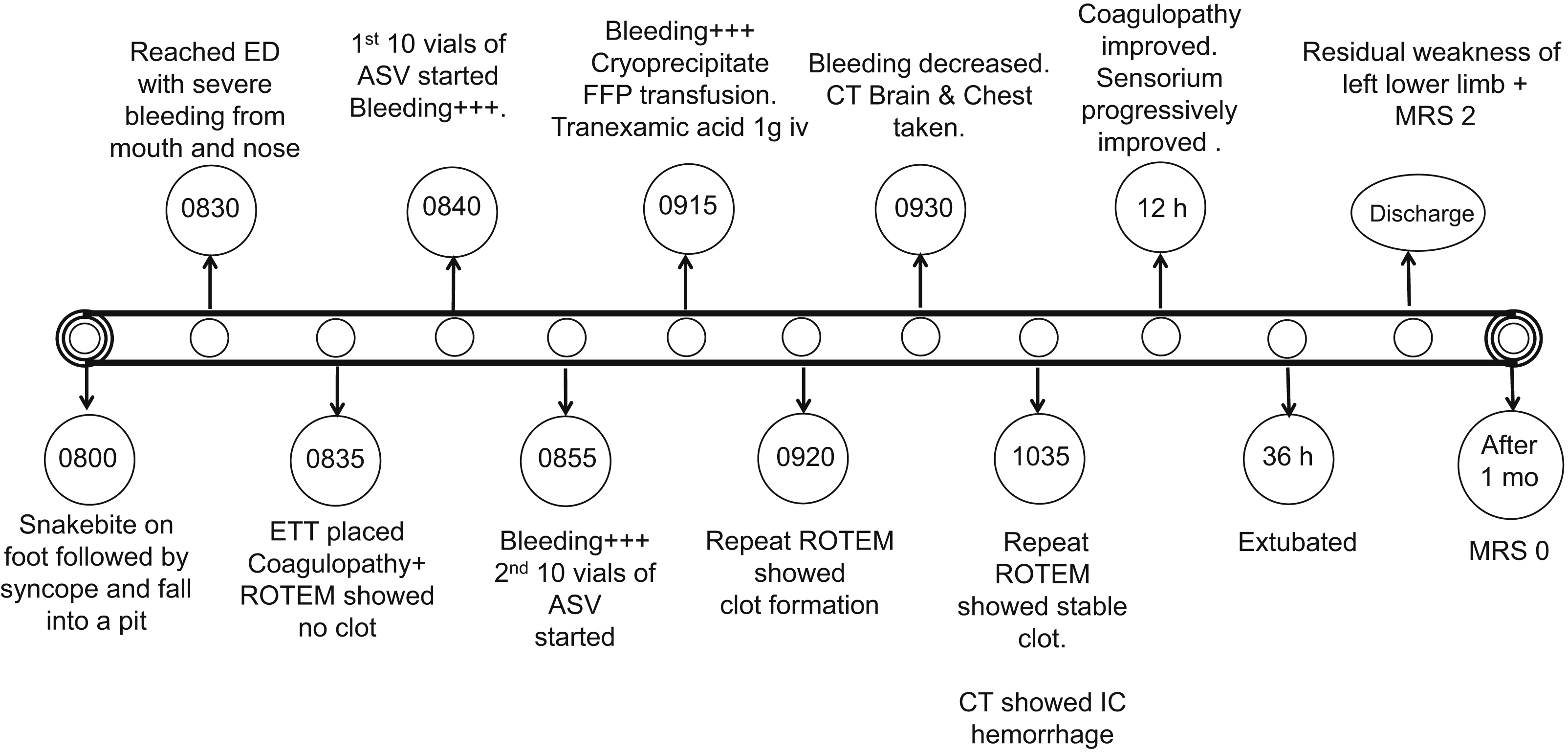
Timeline of events. CT, computed tomography; ED, emergency department; ETT, endotracheal tube; FFP, fresh frozen plasma; IC, intracranial; MRS, modified rankin score; ROTEM, rotational thromboelastometry.
Discussion
Every year, out of the estimated 138,000 deaths that occur globally due to snake envenomation, 50,000 (36%) deaths occur in India.2,3,6,7 Snakebite maims less and kills more in India when compared to other regions in the world. 6 The most common reason for mortality due to snakebite in South India is coagulopathy, which is also the leading cause of morbid renal failure in the victims. 7 -9 The ASV available in India is polyvalent, capable of neutralizing the venom of Russell’s viper (Daboia russelii), binocellate cobra (Naja naja), common krait (Bungarus caeruleus), and saw-scaled viper (Echis carinatus). 6 In Central Kerala, South India, Russell’s viper bites are the most common cause of hematotoxic envenomation, followed by the hump-nosed pit viper (Hypnale hypnale).9,10 Hump-nosed pit viper envenomation in the region has no specific ASV and is notorious for causing prolonged coagulopathy and renal failure. 8 -11
Successful management of snakebite victims with coagulopathy lies in achieving hemostasis and effective nephroprotection. 12 Venom-induced consumptive coagulopathy (VICC) and early trauma-induced coagulopathy (ETIC) are a spectrum of disorders that span hypo- and hypercoagulable states, ultimately causing depletion of the coagulation cascade and resulting in clinical bleed.13,14 VICC is often described as differing from disseminated intravascular coagulation (DIC), especially in its rapidity of setting and resolution. 15 In a patient with trauma after snakebite, the target should be to minimize the clinical bleed in the individual. We suggest the following strategies employed in the case management of a hematotoxic snake envenomation with concurrent trauma.
Early, Rapid ASV
Rapid administration of ASV is controversial, especially because of the antigenic potential of the equine-derived polyvalent ASV in the region. 16 Rapid infusion of ASV (in 20 min) has been shown not to affect the incidence or severity of early ASV reactions compared to slow infusions (over 120 min). 17
The practicing clinician should keep 2 points in mind in this context to guide judgment:
We administered the standard dose of ASV (10 vials) over a period of 15 min and a second dose in another 10 to 15 min, keeping in mind to watch for early anaphylaxis and delayed serum sickness.
Role of Early Transfusion
The firmness or strength of the clot formed aids in stopping the bleed. The stable fibrin mesh formation at the end of the cascade with platelets determines the clot strength. 23
In snakebite victims, the cascade is triggered at multiple levels, leading to consumption of coagulation factors. The fibrinolytic enzymes in the venom concurrently result in dissolution of a formed clot.14,15 Supplementing the coagulation factors in the form of plasma is often theorized to worsen VICC if the venom is not already neutralized by ASV. 24 On the other hand, although ASV is widely recommended for VICC, researchers claim there is limited evidence to support its effectiveness. 25 Plasma transfusion may improve the laboratory parameters in snakebite victims, although its benefits in reducing mortality and morbidity are still under scrutiny.5,14,26,27
In our patient, the ASV was infused in less than 30 min, and we tested the patient’s blood again for any signs of improvement in coagulopathy. With no signs of stable clot formation in the patient and in view of his ongoing maxillofacial bleed, we proceeded with early transfusion.
Role of Cryoprecipitate Transfusion
The ROTEM-guided algorithm supported administration of fibrinogen concentrate or cryoprecipitate over plasma in trauma to improve clot firmness; in the event of massive hemorrhage, clot firmness is affected before thrombin generation. 28
In our case, because blood loss was mostly due to coagulopathy, we decided to replace fibrinogen as we would in trauma, but with restricted fluids to minimize overload and strain of the kidneys.
The venom of both Daboia russelii and Hypnale hypnale is notorious for causing depletion of fibrinogen.14,21 Hypnale envenomation also causes factor VIII deficiency.21,29 ETIC also causes fibrinogen depletion. 30 Cryoprecipitate contains less volume than plasma and is a more concentrated source of fibrinogen and factor VIII. 31 Hence, we preferred it over FFP as our first blood component in a setting of coagulopathy in a snakebite victim with head trauma.
Role of Packed Red Blood Cells in Coagulopathy
The role of red blood cells (RBCs) in achieving hemostasis and their prothrombotic properties are often given less importance by the clinician in comparison to other blood products, such as FFP. 32 The rheological effects of RBCs include their being concentrated in the center of blood vessels, with consequent platelet-rich plasma margination to the vessel wall. 33 RBCs interact with endothelial cells, platelets, and fibrinogen and affect the structure and mechanical properties of clots, aiding in clot stabilization. 34 RBC volume correction should occur concurrently in the management of bleeding patient to improve hemostasis. 35
Role of Rotem-Guided Transfusion in Hematotoxic Envenomation
The traditional coagulation tests (prothrombin time, activated partial thromboplastin time) have been standardized for monitoring therapy in vitro. They inform on the initiation of clotting but may not reflect the hemostatic capacity of the individual in vivo. Global coagulation assays such as viscoelastometric tests (eg, ROTEM, thromboelastogram) or clot waveform analysis look beyond the initiation of coagulation and provide global information on the dynamics of clot development, stabilization, and dissolution that closely reflects hemostasis in vivo.28,36
In our patient, the ROTEM at admission showed no clot formation, whereas the one soon after transfusion showed stable clot formation, which was mirrored by clinical resolution of bleed in the victim (Figure 3). Viscoelastometric tests aid in tailoring transfusion according to patient status in ETIC. 37 Its role in snakebite management is limited to case series and case reports. 38 -43 Fibrinogen depletion that occurs in ETIC is associated with a prolonged CTEXTEM assay. 30
One key aspect of interest in interpreting the results of ROTEM in trauma victims is that they should be in a reasonable sequence (A5FIBTEM prior to CTEXTEM), not according to availability (CTEXTEM prior to A5FIBTEM).28,37 There is also a need to study the results of ROTEM in a snakebite victim to identify its usefulness (in guiding therapy) while avoiding the potential for misinterpretation of the results.
Role of Tranexamic Acid in Snakebite
Fibrinolytic enzymes in snake bite cause dissolution of the formed clot, as evidenced by clot lysis in vitro. 44 Hence, antifibrinolytic drugs have been used in the management of snakebite victims by some.45,46
Microthrombi formed in DIC are shown to lead to end organ damage, as evidenced most commonly by acute tubular necrosis and renal failure. 47 The possibility of thrombotic microangiopathy in bite victims and impaired clearing of microthrombi in renal vasculature leading to renal failure is an argument against the use of antifibrinolytics such as TXA.48,49 In the early phase, DIC is prothrombotic; it then progresses to a hyperfibrinolytic phase and later enters an antifibrinolytic state.50,51 The coagulopathic changes in a snakebite victim happen in a matter of minutes to hours. 36 TXA might have a role in the hyperfibrinolytic phase. Once renal failure sets in, administering TXA could be more harmful because it is dependent on the renal excretion pathway. 52
In our patient with evident ongoing hemorrhage, we administered TXA as a stat dose earlier on. No rise in serum creatinine or decrease in urine output was noted throughout the patient’s hospital stay in our institute. Stringent fluid management and nutritional support were emphasized throughout the management of the victim.
In snakebite, the role of TXA and the timeframe in which it needs to be administered can be challenging because the venom profile and its effect on the coagulation pathway vary among the various snakes seen in this region. 53 Researchers should prospectively take the lead to identify TXA’s potential use in snakebite victim management.
Conclusions
Concurrent administration of ASV and blood products, rapid correction of coagulopathy, and the roles of TXA and viscoelastometric testing are all areas of controversy in the management of snake envenomation and trauma victims. Early and rapid ASV administration is to be considered in envenomated victims with coagulopathy. The role of cryoprecipitate and TXA in specific hematotoxic snakebites needs to be further explored. Even if viscoelastometric tests may not be cost-efficient screening tests, they might have a role in guiding transfusion requirements in patients with coagulopathy after envenomation.
Footnotes
Acknowledgements
Acknowledgments: The authors acknowledge the contribution of Dr Paul Mathai, from the Department of Oromaxillofacial Surgery, for his help in patient care.
Author Contributions: SVA, DM, JT, and KCK were involved in the patient care. SVA reviewed the literature and wrote the first draft. BH and DM were responsible for the infographics and compilation of the figures and legends. AP, SVA, DM, AMR, JT, BH, and KCK reviewed the manuscript and approved it.
Financial/Material Support: None.
Disclosures: None.