
Abstract
Snakebite envenoming is a neglected tropical disease disproportionately affecting the rural and marginalized population in low-middle-income countries. The saw-scaled viper (Echis carinatus) is a clinically important snake that causes serious morbidity and mortality in the Indian subcontinent. Even though it is within the so-called big-four snakes against which polyvalent antivenom is available throughout India, reports of antivenom ineffectiveness are emerging in saw-scaled viper envenoming, especially around Jodhpur, Rajasthan, India. This case report highlights a patient with saw-scaled viper envenoming with an ineffective antivenom response complicated by acute kidney injury as well as local and systemic bleeding complications, which subsequently resulted in a pelvic hematoma that compressed the lumbosacral nerves, causing lower-limb weakness and sensory deficits. He was successfully managed with hematoma aspiration and supportive care. This case brings into focus the challenges of managing saw-scaled viper envenoming in this region with antivenom ineffectiveness, resulting in delayed and significant coagulopathy and its complications leading to prolonged hospital stay and morbidity. Our report spotlights less emphasized aspects of long-term morbidity in snakebite survivors, such as loss of working days and productivity. We also highlight the need for an organized system of long-term follow-up of snakebite survivors to screen for possible complications and manage them early.
Introduction
Snakebite envenoming is a neglected tropical disease estimated to cause 0.8 deaths (0.5–1.0) per 100,000 people globally, and India had the greatest absolute number of snakebite envenoming deaths of >50,000 annually; in addition, snake bite envenoming resulted in long-lasting disabilities and sequelae in at least another 400,000 people. 1 -3 As the World Health Organization mandate to reduce snakebite mortality by half by 2030 is drawing near, there is a serious need to focus on survivors and mitigating their disabilities.4,5 In this report, we highlight a case of saw-scaled viper (Echis carinatus sochureki) envenoming in Rajasthan, which is a high-burden state in India for both snakebite envenoming and deaths, with a disabling complication of painful limb paralysis following a pelvic hematoma compressing the lumbar plexus 30 days after the snakebite.3,6
The Indian polyvalent antivenom contains immunoglobulins purified from the plasma of horses hyperimmunized with venom from Naja naja, Bungarus caeruleus, Daboia russelii, and Echis carinatus. Most of the venom collected for antivenom production in India comes from a small geographic area through the Irula Cooperative Society, Tamil Nadu, India. 7 This report also highlights region-specific issues related to snakebites, such as the ineffectiveness of the available Indian polyvalent antivenom in Rajasthan due to the presence of medically important regional subspecies (Echis carinatus sochureki) whose venom is not used in the manufacturing of polyvalent antivenom, leading to various complications in survivors.
Case Report
A 50-y-old male farmer with no prior comorbidities presented to our hospital with right foot swelling 2 h following a saw-scaled viper bite while working at his farm; the snake was killed, and a photograph was taken by the patient’s family (Figure 1A). Local examination showed fang marks and swelling (Figure 1B). He had local oozing of blood and gingival bleeding. A 20-min whole-blood clotting test, a bedside test to determine the need for antivenom, was performed, which found positive incoagulable blood at 20 min, suggesting venom-induced consumption coagulopathy (VICC). Laboratory investigations showed normal hemoglobin level and total leucocyte count, with thrombocytopenia (platelet count, 47×109⋅dL−1), low plasma fibrinogen level (0.6 g⋅L−1), prothrombin time of 18.3 s (control value, 12.1 s), and activated partial thromboplastin time of 32.1 s (control value, 21.7 s) (testing performed using Sysmex CA1500 Hemostasis System and Thromorel S kit reagent and control plasma; Siemens Healthcare Diagnostics, Marburg, Germany). He was administered 10 vials of polyvalent antivenom (BNo. A05321080; Bharat Serums and Vaccines Limited, Mumbai, India) at presentation and 10 vials subsequently at 6 and 12 h after the first dose for persistent complete VICC with local and gingival bleeding. Despite antivenom, swelling progressed up to the right knee over the next 3 h and further to the thigh and inguinal region over the next 6 h, with right inguinal lymphadenopathy. The patient developed oliguria, with a serum urea concentration of 126 mg⋅dL−1 and creatinine level of 4.92 mg⋅dL−1 on day 2 of envenoming. He was initiated on hemodialysis for management of acute kidney injury (AKI). By week 3, his hemoglobin level remained at 6.5 to 7.1 g⋅dL−1, while the platelet count improved (nadir platelet count, 27×109⋅dL−1 on day 4), and coagulopathy was improving, as noted by an international normalized ratio of <1.5 (Table 1). 8 Blood transfusion support with cryoprecipitate, fresh frozen plasma, and packed red blood cells was administered, along with 3 sessions of plasma exchange for possible thrombotic microangiopathy. The patient developed pneumonia on day 20 in hospital, which was managed with antibiotics (piperacillin-tazobactam and azithromycin, later changed to meropenem) and supportive care. His plasma fibrinogen level was persistently low, with raised concentrations of D-dimer (>20 mg⋅L−1; normal value, <0.5 mg⋅L−1) and serum lactate dehydrogenase (1148 U⋅L−1; reference range, <270 U⋅L−1). The patient required intensive care support for 30 d and 8 sessions of hemodialysis, with slow improvement in urine output.
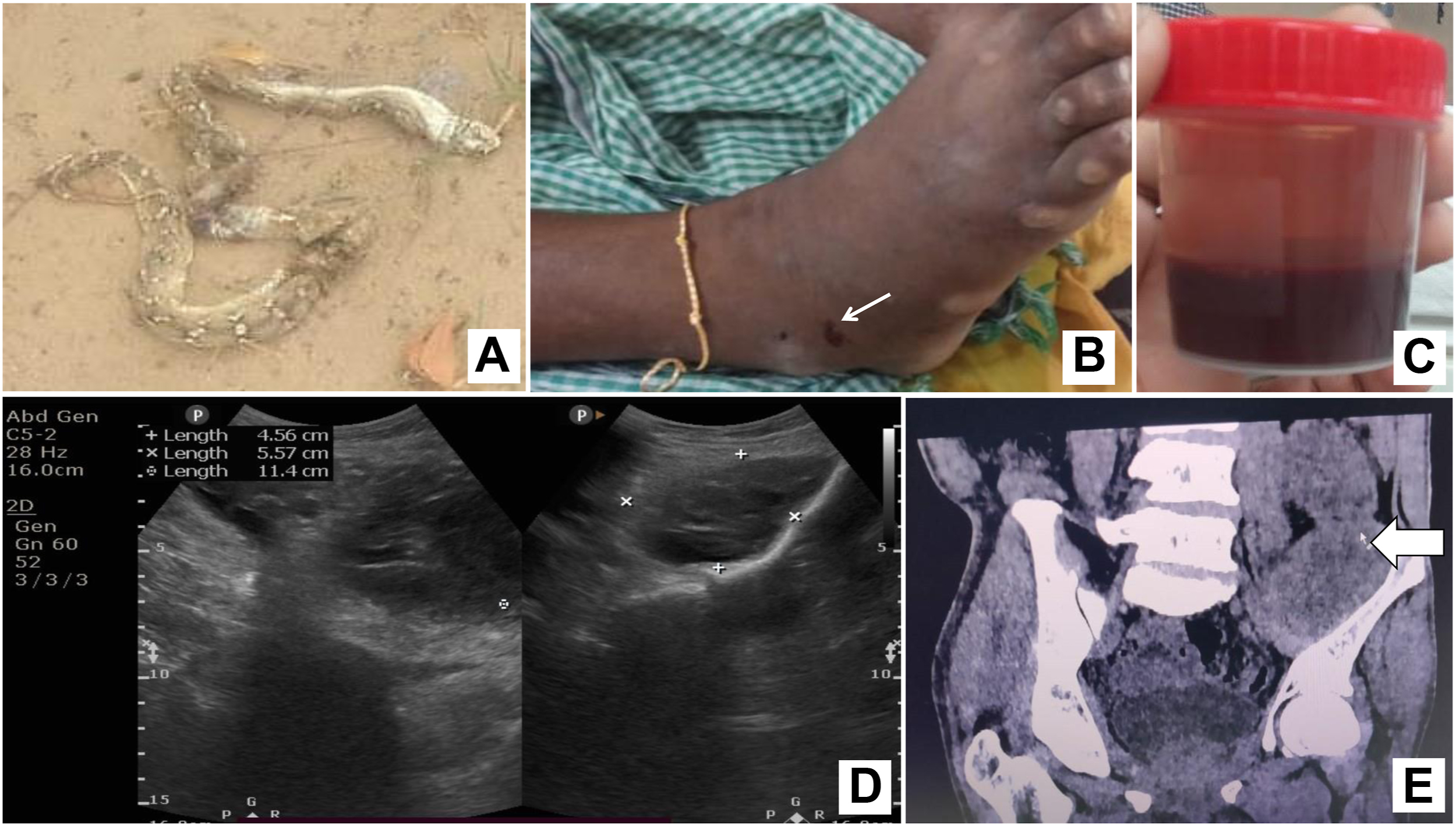
A, Photograph of the snake identified as Echis carinatus sochureki (Courtesy: patient’s family). B, Right foot swelling with fang marks (white arrow) with blood oozing. C, Blood aspirated from pelvic hematoma under ultrasound guidance on day 42. D, Ultrasonography of the pelvis after aspiration of the pelvic hematoma on day 42. E, Computerized tomography of the pelvis (coronal section) on day 48 showing residual collection after aspiration of the hematoma (white arrow).
Serial coagulation parameters, procedures, and blood product transfusions in the patient with Echis carinatus sochureki envenoming
aPTT, activated partial thromboplastin time; Cryos, cryoprecipitate; CT, computerized tomography; FFP, fresh frozen plasma; HD, hemodialysis; INR, international normalized ratio (<1.5=resolved coagulopathy); PLEX, plasma exchange; PRBC, packed red blood cell; PT, prothrombin time; RDP, random donor platelet; VICC, venom-induced consumption coagulopathy.
On day 30, after the envenoming, the patient was transferred to the medical ward and complained of paresthesia and tingling of both lower limbs, which had progressed over the previous 5 d, causing difficulty standing up from a sitting position. He was able to walk with support. On evaluation, the patient was found to have a proximal muscle power medical research council grade of 4/5 in both lower limbs, with wasting of left quadriceps and absent left knee jerk. Bilateral ankle jerks were normal, and he reported decreased perception of touch, temperature, and pain sensations (50% compared with these sensations over his arms). He was evaluated further for this gradually progressive asymmetric proximal muscle paralysis and sensory loss. A nerve conduction study revealed left femoral, peroneal, and saphenous axonal nerve conduction defects, suggestive of lumbosacral plexopathy. Ultrasound of the pelvis showed an 8.5×6.1×12.5-cm3 ill-defined hypoechoic collection with thick internal septation in the left iliac region abutting the iliopsoas muscle posteriorly. Further, noncontrast CT of the pelvis confirmed an intramuscular hematoma, 200-mL size in the left iliopsoas muscle. There was no history of trauma. Hence, the patient was diagnosed with delayed limb paralysis following iliopsoas hematoma. As coagulopathy had resolved by day 33 (Table 1), ultrasound-guided aspiration of the hematoma was performed, which, however, revealed frank blood (Figure 1B–D). A follow-up noncontrast CT of the pelvis showed a significant reduction in the collection volume (Figure 1E). The patient improved symptomatically following the aspiration procedure and was discharged on day 51. Muscle power and sensation improved gradually over the next 3 mo. The clinical course is summarized in Figure 2. At 3 mo, repeat ultrasound showed complete resolution of the hematoma. The patient was pain free and able to walk without support following 3 full months of physical rehabilitation and as-needed pain medications, including tramadol and, later, nonsteroidal anti-inflammatory drugs.
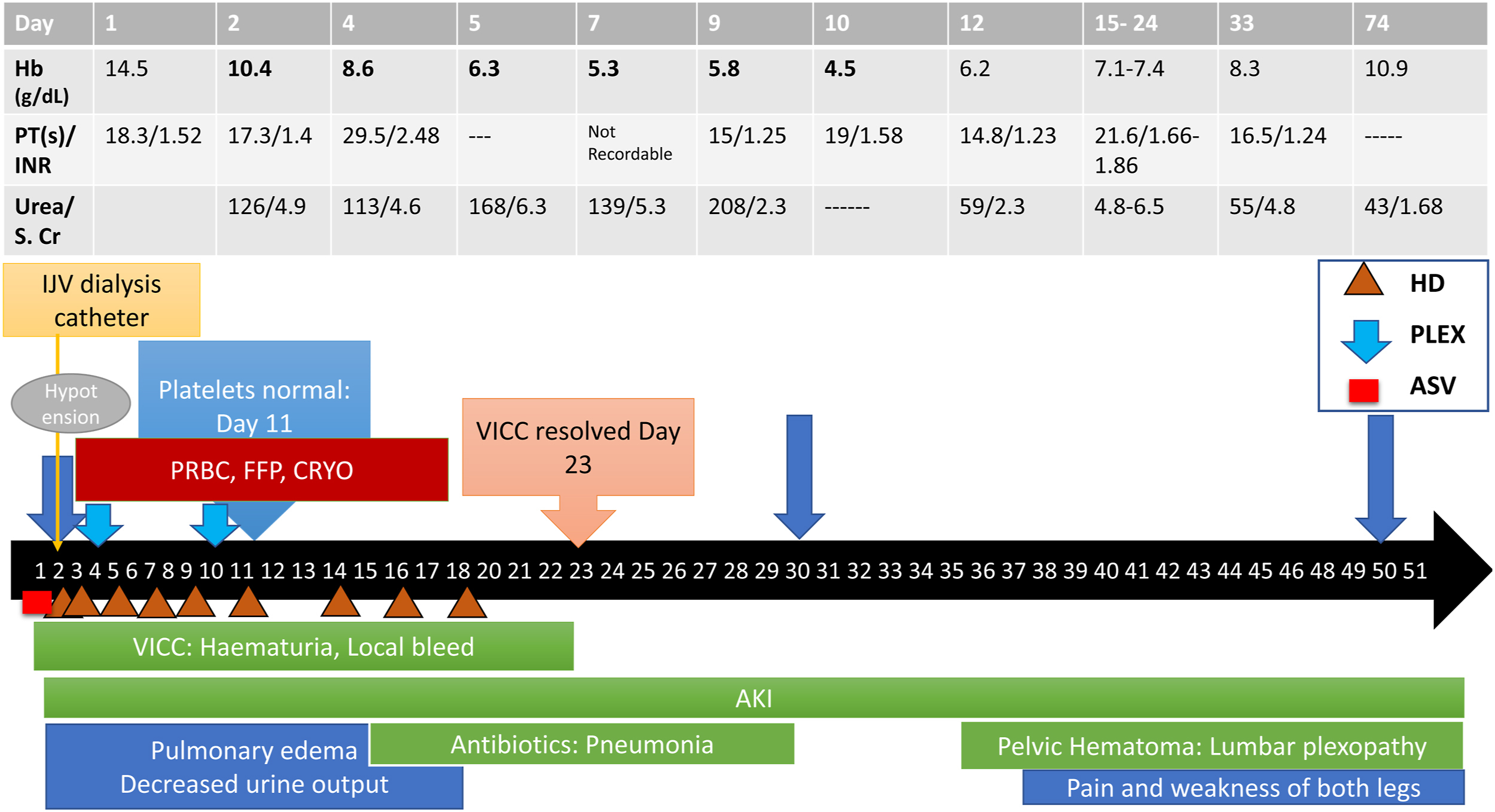
Timeline depicting the clinical course of events and management of the patient. AKI, acute kidney injury; ASV, antivenom; CRYO, cryoprecipitate; FFP, fresh frozen plasma; Hb, hemoglobin; HD, hemodialysis; IJV, internal jugular vein; INR, international normalized ratio; PLEX, plasma exchange; PRBC, packed red blood cell; PT, prothrombin time; S. Cr, serum creatinine; VICC, venom-induced consumption coagulopathy.
Discussion
Most snakebite envenomings in India are attributed to the “big-four” snakes—Indian cobra, krait, Russell’s viper, and saw-scaled viper. However, other regional species or subspecies, such as E c sochureki in the Thar desert areas of Rajasthan, India, are emerging as medically significant.9,10 Viper venom is hemovasculotoxic, causing endothelial dysfunction and bleeding due to coagulopathy and thrombocytopenia. 11
Our patient had coagulopathy requiring extensive transfusion support, AKI requiring renal replacement therapy, and, later, lower-limb weakness, with inability to mobilize, resulting in 50 d of hospital stay, all following a single devastating snakebite event. His weakness occurred because of compression of the lumbosacral plexus and related nerves by a hematoma formed owing to persistent and delayed coagulopathy as a result of antivenom ineffectiveness. He needed multiple invasive procedural interventions for management. While acute hemorrhagic complications of viper envenoming are well known, delayed hemorrhagic complications resulting in long-term disability are not well documented.
Delayed bleeding complications, including broad ligament hematoma, intrabdominal collection, splenic rupture, and delayed pelvic hematoma, have been reported following 2 to 6 d of snakebite. 12 -15 Possible reasons for delayed complications are persistent venom hemorrhagins and hemolysins with VICC and defibrination syndrome possibly due to ineffective antivenom response. 2 Though the initial focus in our patient was on other life-threatening complications (bleeding, AKI, and pneumonia), nerve compression symptoms lasting beyond 1 mo of the bite resulting in a serious disability is an important sequela that deserves to be highlighted. Femoral neuropathy following iliopsoas hematoma is a rare complication that has been reported postoperatively and in patients with bleeding diathesis (hemophilia) or anticoagulant use.16,17 Additionally, the prolonged coagulation defects in the form of delayed hypofibrinogenemia, which lasted >26 d (the plasma fibrinogen level on day 26 of the bite was 1.09 g⋅L−1), is another serious issue that requires further exploration.
Antivenom ineffectiveness is an important factor evident in our patient with prolonged coagulopathy, leading to spontaneous pelvic bleeding along with AKI requiring renal replacement therapy, as he developed these complications despite more-than-adequate doses of antivenom administered early (within 3 h) in the course of envenoming. E c sochureki, a subspecies of E carinatus, common in Rajasthan, is increasingly being implicated in prolonged coagulopathy resulting from an inadequate antivenom response.2,9,10 The ineffectiveness of antivenom is a serious problem in this part of the country, where transfusion support and supportive care are the only management a healthcare provider can offer in the event of a viper bite. Most of the complications, hospital stay, and morbidity could have been prevented and addressed by a more effective antivenom in this patient.
The reason for the antivenom ineffectiveness in this report is thought to be potentially due to intraspecific variation in venom composition across different diverse geographic regions. Venom collected for the production of polyvalent antivenom in India is from a confined geographic region, Tamil Nadu, located on the southeastern coast of India. This suggests that antivenom prepared from the venom of snakes that are geographically remote to Rajasthan may not be as effective as antivenom prepared from snakes within the local geographic region.10,18,19
Though the focus is usually on mortality and acute complications, long-term health effects due to snakebites are not uncommon. Snakebite survivors are affected by economic burden, livelihood and livestock loss, marked disabilities, and psychological burden. 20 Disabilities due to snakebite range from swelling of the involved limb, muscle wasting, reduced muscle power, fixed deformities, chronic nonhealing ulcers, visual loss, chronic kidney disease, myocardial ischemia, stroke, depression, and endocrine dysfunction of long-standing limb or digit amputations. 21 -23All these are closely related to the geographical, socioeconomic, and public health status of the region.24,25
Our patient, an agricultural laborer, faced not only physical morbidities but also financial stresses that undermined his fitness to work, resulting in a huge loss of productivity following the single snakebite event. Fortunately, the insult was reversible because of available support at our tertiary care center; however, the nature of complications and the time-to-recovery time sorely highlight a need for a better management system in these patients.
Currently, no organized health systems exist in low-middle-income countries for addressing the long-term effects of snakebite or their sequelae. Though there is some support for snakebite deaths, such as direct cash transfer to families of victims, survivors are often neglected. 5 Our patient experienced at least 3 mo of distress even with reversible complications. A better model of healthcare delivery, reorienting the system beginning primary care onward from only mitigating acute crises to comprehensive long-term snakebite care, is urgently required. Policymakers must consider disability benefits as with occupational diseases for snakebite victims. 26
Conclusion
Our report serves to highlight the lesser-known long-term complication of nerve root compression resulting from uncorrected coagulopathy and pelvic hematoma and the consequent disability faced by a snakebite survivor who suffered envenoming from E c sochureki. Better antivenoms and healthcare delivery systems to address long-term complications arising after snakebite envenoming are urgently needed in this region.
Footnotes
Acknowledgments
We gratefully acknowledge the patient’s family for sharing the image of the snake. We wish to express our thanks to Mr Vishal Santra, Member - International Union for Conservation of Nature (IUCN) Viper Specialist Group Secretary, Society for Nature Conservation, Research and Community Engagement, for inputs on identifying the snake.
Author Contributions: study concept and design (MKG, MG); data acquisition (AK, AK, PG, AS, MKG, MG); data analysis (AK, PG, AS, MKG, MG); drafting and critical revision of the manuscript (AK, AK, MKG, AS, MG); all authors read and approved the final manuscript.
Financial/Material Support: None.
Disclosures: None.