
Abstract
The spotted deer Axis axis is a Cervidae mammal that lives in most parts of Southeast Asia. Spotted deer attacks on humans are scarcely reported in the literature and are a rare phenomenon. A 31-y-old man was attacked by an unprovoked male spotted deer while supervising maintenance inside a deer enclosure. The victim received deep lacerations in the lower limbs and puncture wounds in the chest and abdomen. The victim made a full recovery after prompt management at a tertiary care hospital. The potential factors leading to this uncommon attack are discussed.
Introduction
The spotted deer Axis axis is a cervid mammal found in Sri Lanka, India, Nepal, Bangladesh, and Bhutan. 1 The subspecies Axis axis ceylonensis (Figure 1) mainly inhabits the lowland forests of the dry zone in Sri Lanka. 2 Spotted deer are herbivores that spend much time in open glades and grassy areas in the forest and are most active in early mornings and afternoons. 2 Despite being a shy animal, it has a marked behavior change during the rutting season and often becomes more territorial, aggressive, and likely to attack other animal species or even humans. 2

Spotted deer Axis axis ceylonensis captured in Wilpatthu national park.
Injuries related to mammals of family Cervidae have been reported in literature. 3 -7 However, the mechanism of injuries, sequela, and management of Axis axis ceylonensis attacks and related injuries in humans have never been described. We describe a case of a man who was attacked by a spotted deer and recovered without significant complications.
Case presentation
A 31-y-old man sustained an unprovoked attack by a male spotted deer. The man was supervising a crew repairing a water line inside the deer enclosure located at an army camp. At that time, a deer herd was grazing at a distance of 30 to 40 m. The deer first struck the patient in the right lower leg, knocking him to the ground. While he was on the ground, the same deer attacked again, causing injuries to the right side of the chest, abdomen, and medial aspect of the right thigh. The deer attacked again when the man stood up. The man tried to restrain the deer by holding onto its antlers, thus sustaining injuries to his right arm. The work crew intervened to rescue him from the attack. First aid was administered before he was transferred to teaching hospital Anuradhapura in stable condition.
The physical examination at the hospital revealed puncture wounds in his chest (Figure 2A) (1 cm by 2 cm) and abdomen (Figure 2B) (1 cm by 2 cm), a deep laceration (Figure 2D) (5 cm by 7 cm) in the right calf and a laceration (1 cm by 2 cm) in the right thigh (Figure 2C), a laceration (1 cm by 2 cm) in the posterior aspect of the right elbow, and abrasion in the anterior aspect of the right arm (9 cm by 1 cm). He had decreased air entry to the right lung base and mild tenderness in the upper abdomen. A tube thoracostomy was performed. Focused abdominal sonography for trauma was negative. The contrast-enhanced computed tomography revealed hemopneumoperitoneum and liver contusion but no evidence of bowel perforation. The x-rays of the hand revealed no evidence of fractures. Prophylactic intravenous cefuroxime and metronidazole were administered. Oral diclofenac sodium was provided for analgesia. Injection of tetanus toxoid was given as a prophylactic measure. The patient’s vital signs were monitored throughout the night.
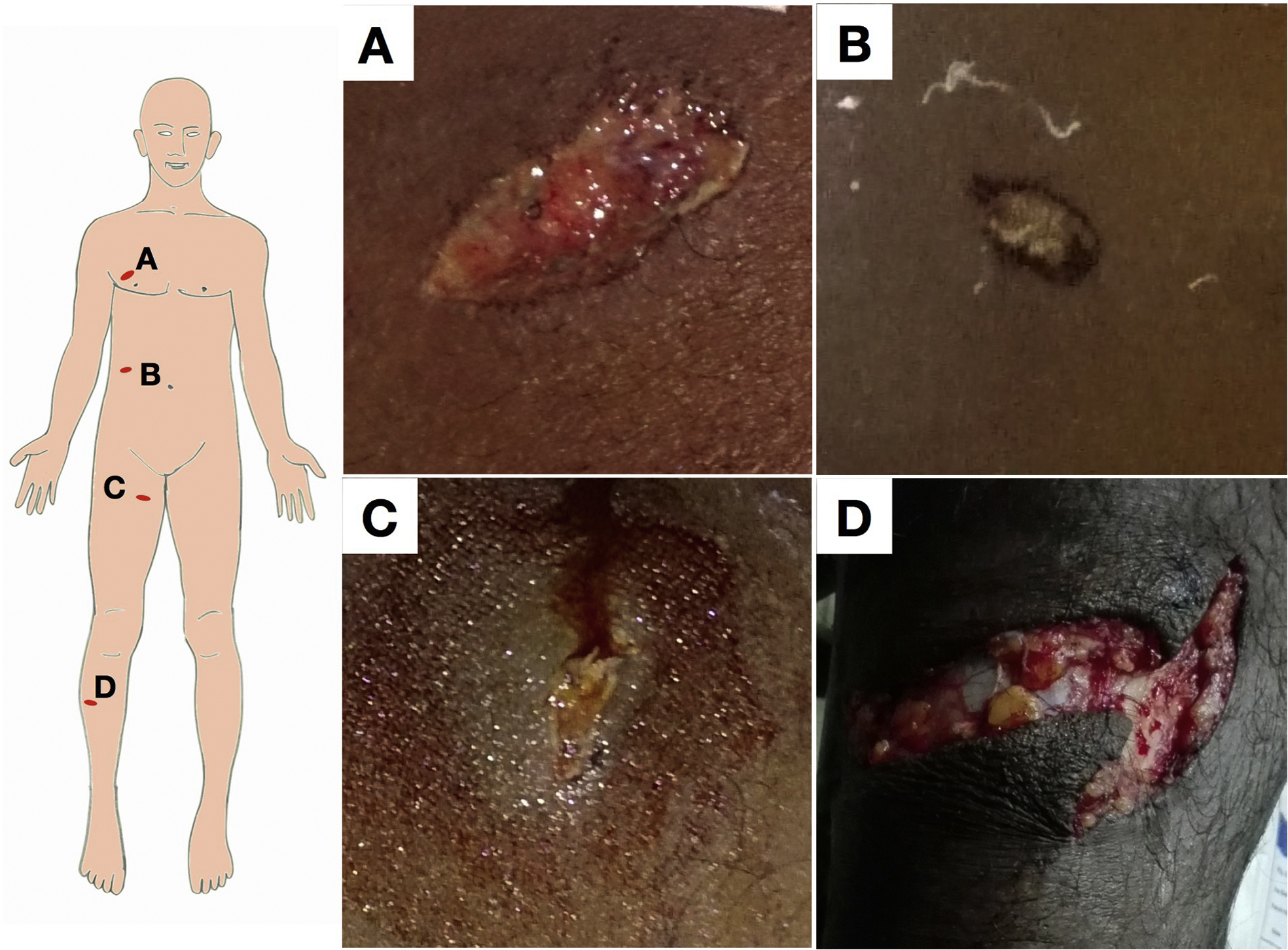
Injuries sustained by the patient. (A, B, and C) Penetrating injuries. (D) Laceration.
On hospital day 2, wounds were explored under general anesthesia. The upper and lower limb and chest wounds were cleaned and sutured. Initial contrast-enhanced computed tomography revealed no evidence of bowel perforation or active bleeding; subsequently, the patient was managed conservatively, and oral intake was resumed on the same day.
On hospital day 3, intravenous antibiotics were changed to oral cloxacillin and metronidazole. Chest physiotherapy and nebulization with a bronchodilator were initiated. The patient developed a fever in the evening, and auscultation revealed lung crackles. Repeat computed tomography showed a mild interval increase in hemoperitoneum. Intravenous clarithromycin was added to the antibiotic regimen for broader coverage.
He was mobilized over the following days. On hospital day 9, the thoracotomy tube was removed. He was discharged on hospital day 10 with oral antibiotics and analgesics for a week. He was subsequently seen for follow-up in the surgical clinic 2 wk after discharge and was recovering well with no permanent disabilities.
Discussion
There are 4 species of cervids found in Sri Lanka: the sambar Cervus unicolor, barking deer Muntiacus muntjak, hog deer Axis porcinus, and spotted deer Axis axis ceylonensis. 8 The Axis axis ceylonens is a slender, graceful deer typically found in herds of hinds, fawns, and a few stags. 2
The adult male deer exceeds the female in both size and weight.2,9 The male deer has a usually bright, glossy rufous color, spotted all over the upper parts with small, pure white spots. Its fur is soft, short, and close over the whole body and a little longer on the tail. The males have antlers, in contrast to the females, which they use to fight with other males during the mating season. Sometimes they kick their victims.
The mating season of Sri Lankan subspecies seems to be irregular and intermittent throughout the whole year, 2 in contrast to many other species of cervids with clear rutting seasons. 3 As a result of deforestation, this once abundant species is increasingly confined to national parks and reserves. Spotted deer do well in captivity and are often kept in parks and large gardens in Sri Lanka. 2
We performed an extensive literature search on spotted deer attacks using online medical literature databases (PubMed, Scopus) and found no published literature on a human attack by spotted deer. Published Cervidae attacks have led to injuries ranging from soft tissue injuries, scalp lacerations, and concussions to broken or dislocated bones and death. 3 -7
Male Cervidae attacks are thought to be primarily related to the rut, whereas female Cervidae attacks have occurred when animals are cornered or protecting offspring.8,10 During the rutting season, male deer become highly territorial and perceive other males as a potential threat. The rutting season is highly irregular in Sri Lanka, and the spotted deer involved in this case likely was in a rut and attacked to defend its perceived territory. 8
Conclusions
We have outlined the management in a case of a spotted deer attack. The patient should be thoroughly assessed according to advanced trauma life support protocol. 11 Depending on the extent and severity of injuries, relevant imaging and other investigations should be performed. Pain should be assessed objectively using a pain score, and a suitable analgesic should be administered based on the World Health Organization analgesic ladder. 12
The tetanus immunization status of the patient should be assessed and appropriate immunization provided. We recommend empiric broad-spectrum antibiotics for antler wounds. Wounds must be copiously irrigated and, depending on the degree of contamination, either primarily or secondarily sutured. Unexpected encounters are rare because spotted deer have an acute sense of hearing and usually avoid interactions with humans. Nevertheless, male deer can become aggressive during the rutting season, and female deer can become aggressive when defending offspring. Those at risk include hunters, loggers, farmers, hikers, zookeepers, and people who keep them as pets. If a deer becomes aggressive, we recommend staying away or being cautious about a possible attack from Cervidae species whenever possible, despite the common belief that these deer are shy. Zookeepers and other animal handlers should avoid turning their back to deer and should ideally be accompanied by colleagues in the animal enclosure.
Footnotes
Acknowledgements
Acknowledgments: The authors thank Mr. Sidantha Wijerathne for the image of a spotted deer in Wilpaththu national park in Sri Lanka.
Author Contributions: Study concept, management of patient (SPBT); literature review and drafting and editing of the manuscript (SPBT, BTBW); data collection (HSW); approval of final manuscript (SPBT, BTBW, HSW).
Financial/Material Support: None.
Disclosures: None.