
Abstract
The sloth bear (Melursus ursinus) is an omnivore that has been reported around most parts of South Asia. Although rare, sloth bear attacks can inflict potentially life-threatening injuries. This cross-sectional study analyzed 10 patients who had been mauled by sloth bears and who presented to rural hospitals in the Anuradhapura district of Sri Lanka between 2015 and 2019. All of the patients were male farmers. The human–bear encounters occurred in the jungle during the daytime. Ten victims sustained multiple soft tissue and bone injuries, mainly to the face and arms. The injuries ranged from minor abrasions to extensive deep lacerations and bone fractures. All of the patients were managed in the tertiary care hospital by multidisciplinary surgical teams. Sloth bear-inflicted wounds must be treated as major trauma. There is a need to formulate guidelines and train medical officers in managing animal-inflicted injuries in Sri Lanka.
Introduction
The sloth bear (Melursus ursinus) is an omnivore that has been reported in Sri Lanka, India, Bangladesh, and Nepal. 1 The Sri Lankan subspecies (Melursus ursinus inornatus) (Figure 1A and B) is found primarily at low elevations (≤300 m) in open forests with lower human population densities.2,3

A and B, Sri Lankan sloth bear (Melursus ursinus inornatus) front & side view. C and D, sharp claws. (Figure 1A, C & D taken by author BTBW and Figure 1B taken by Dr. PADM Senarachchi, in Wilpaththu National Park in Sri Lanka).
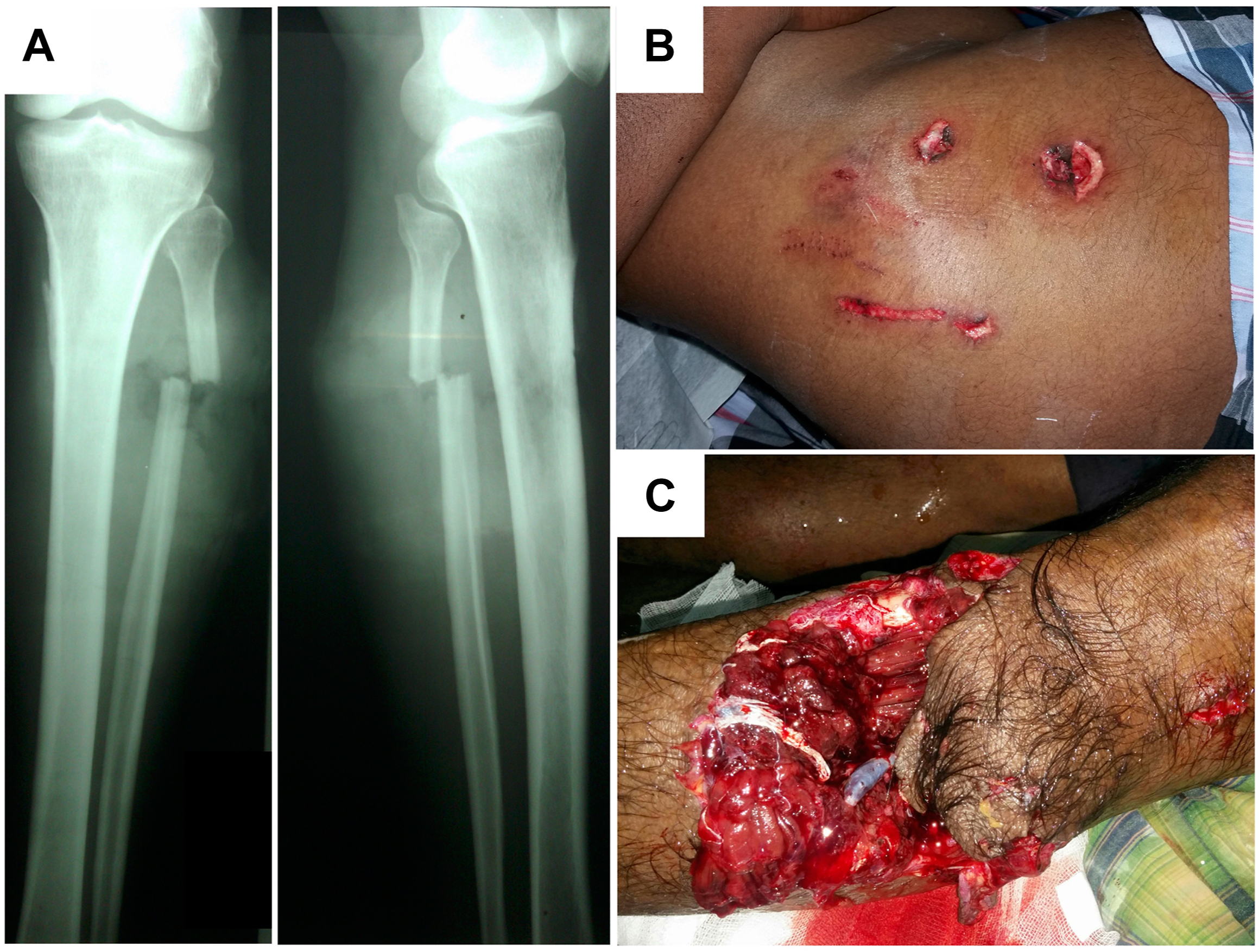
A, Case 1–Fibular fracture; B, Case 3–Abdominal laceration and, C, Case 4–Laceration near right knee.
The Sri Lankan sloth bear has a large head and powerful forefeet but weaker hindquarters. The average height of adult male is about 90 cm at the shoulder and female is about 60 cm. 4 They weigh between 75 to 100 kg. 4 The fur of the body is rather long, shaggy, and sparse. 2 The claws are well developed (Figure 1C and D), enabling the bears to climb trees and dig for termites. 2 They have powerful jaws and strong teeth with prominent canines. The claws and teeth can inflict terrible injuries. They have a fearsome reputation among farmers as an animal that attacks without provocation.5,6 The Sri Lankan sloth bear does not have a distinct breeding season. 2 They have unique adaptations for feeding on termites and are fond of honey and fruit.2,5
Attacks on humans have been reported in Sri Lanka since the 19th century, 7 but details of injuries and medical management have rarely been documented. Almost all bear attacks occur in dry zones, and a significant number are in the Anuradhapura district. 5 Bear attacks can cause physical disability, which profoundly affects the earning capacity of victims, and concomitant physical disfigurements affect their psychosocial wellbeing.
The objectives of this study were to describe the demographics, clinical manifestations of injuries, and management outcomes of bear attack cases admitted to the Teaching Hospital Anuradhapura (THA) over 5 y.
Methods
A cross-sectional retrospective analysis of medical records of bear attack victims presented to the university surgical unit and clinic at THA from January 2015 through December 2019 was carried out. The clinical data of patients were extracted from the medical records by a medical officer within few days or weeks after leaving the hospital. Later, after informed consent, the patients were contacted over the phone and interviewed. The patient demographics, circumstances of the incident, the number of bears involved in the attack, injury profile, defensive strategy, first aid used, management, and complications were recorded. Descriptive statistics were calculated using an online calculator (QuickCalcsl; GraphPad Software). Ethical clearance was obtained from the ethics review committee of the faculty of medicine and allied sciences, Rajarata University of Sri Lanka. Data are presented as mean±SD with range.
Results
All 10 patients were male, 40±11 (20–53) y of age. There were 2 attacks in the northeast-monsoon season (Dec–Feb), 1 attack in the first inter-monsoon season (Mar–Apr), 5 attacks in the southwest-monsoon season (May–Sep), and 2 attacks in the second inter-monsoon season (Oct–Nov). Human and bear encounters occurred between 0730 and 1800. Six attacks occurred between 1200 and 1500. Nine attacks occurred in the jungle (unprotected areas), and 1 in a chena (swidden farming practiced in Asian countries). Six occasions involved a solitary bear. In 3 of these encounters, the victims were mauled while searching for fruits of the ironwood tree (Manilkara hexandra), the dragon’s eye tree (Dimocarpus longan), or for bee honey. These are all common sources of food for bears and humans.
Two attacks involved 2 bears. Two bears jumped on the victim from a close distance in the first attack, whereas 2 bears emerged from behind an anthill and attacked in the other instance. Two other incidents involved female bears accompanied by cubs.
In 8 incidents, bears made a frontal attack; the victims sustained soft tissue injuries to the scalp, face, nose, ears, muscles, and buttocks and fractures to the upper and lower limbs and the mastoid and zygomatic bones. When they fell, the bear bit various parts of the body, causing multiple injuries. On 2 occasions, the victims were initially bitten on the leg. In the first instance, the bear charged for about 15 to 20 min, bellowing. The victim hit it with a wooden pole, and the bear fell and bit the patient’s left calf, which resulted in left common peroneal nerve injury followed by nerve palsy. On the other occasion, the victim nearly stepped on a bear lying on the ground and was bitten on the leg.
One patient developed cerebrospinal fluid rhinorrhea and pneumocephalus and was given empirical antibiotics to prevent meningitis. He did not developed meningitis during his hospital stay of 17 d. Nine patients were initially admitted to peripheral hospitals, and 1 to the THA. Upon admission to the peripheral hospital, the hemodynamic statuses of 6 patients were not recorded; 3 patients’ hemodynamic statuses were recorded. Two patients (Table 1, patients 05 and 10) were hemodynamically stable. One patient (Table 1, patient 01) had a blood pressure (BP) of 90/60 mm Hg and a pulse rate of 88 beats·min-1. Because both blood and blood products were not available in the peripheral hospitals, IV fluid resuscitation with crystalloid was started for this patient, whereas for the other 3 patients, IV access was established. Empirical IV antibiotics were administered to 5 patients, and another received oral antibiotics. Four out of 9 patients were given tetanus toxoid injections. Subsequently, all 9 patients were transferred to the THA within 40 to 100 min. At the time of admission to the THA, 9 out of 10 patients were hemodynamically stable. One patient (Table 1, patient 01) transferred from a peripheral hospital had a BP of 100/60 mm Hg and a pulse rate of 98 beats·min-1.
Summary of bear attack cases
M, man; PR, pulse rate; BP, blood pressure; IV, intravenous; IM, intramuscular; PO, per oral; PPI, proton pump inhibitor; ARV, anti-rabies vaccine; RIG, rabies immunoglobulin; THA, Teaching Hospital Anuradhapura; CSF, cerebrospinal fluid POP, plaster of Paris; ORIF, open reduction and internal fixation.
All had x-rays of their limbs and chest, but 2 patients who had sustained extensive facial and scalp injuries had CT scans of the skull, brain, and face.
Intravenous fluids were continued for 4 patients and started for others to maintain IV access. The IV antibiotics were administered empirically to cover gram-positive, negative, and anaerobes. All were given nonsteroidal anti-inflammatory drugs and proton pump inhibitors in combination with paracetamol. An opioid was added for 6 patients. Tetanus toxoid was administered to the 5 patients who did not receive it at the peripheral hospital. Due to the risk of contracting rabies, all patients were immunized against rabies (immunoglobulin followed by a course of rabies vaccine).
After initial management, the wounds were explored; the devitalized tissues were excised, and the wounds were thoroughly irrigated with normal saline under general anesthesia and aseptic conditions in the operating theater. In 6 cases, primary suturing was done. In the remaining 4, wounds were dressed in 10% povidone-iodine-soaked gauze. Delayed primary suturing was performed for 3 patients (Table 1, patients 05, 06, and 07) within 24 to 48 h, but in 1 patient, the timing of suturing was not recorded. Two patients (Table 1, patients 07 and 08) with extensive soft tissue injuries and fractures were managed by teams of plastic, oromaxillofacial, orthopedic, and otolaryngology surgeons. One of them was managed in the intensive care unit for 1 d, in anticipation of breathing problems due to significant facial edema.
Patient 1 had tachycardia and a BP of 100/60 mm Hg on admission to the THA. Two others (Table 1, patients 07 and 08 ) lost blood in the perioperative period. These 3 patients had blood transfusions (1 unit of red cell concentrate each) to compensate for blood loss. The hospital stay was 7±5 (2–17) d. Two patients (Table 1, patients 07 and 08 ) who sustained multiple severe injuries were kept in the hospital for 11 and 17 d, respectively.
While in the hospital, 1 patient developed flap necrosis of the scalp and another developed common peroneal nerve palsy. None of the patients died from their injuries.
Discussion
Dwindling forest cover, increased population density, and encroachment on traditional bear habitats has led to a rise in human–bear encounters, causing increased mortality and morbidity of both humans and bears. A study carried out in the dry zone of Sri Lanka showed that the number of bear attacks on humans doubled every 5 y for the past 20 y. 5 All of our patients were men, similar to other studies done in the region.5,8–10 In South Asian countries, men are the primary income earners. They visit forests to gather livestock, hunt, and collect nontimber forest products. They tend to travel alone and walk deeper into the forest than women, thus increasing the probability of encountering bears. 9 There is a positive relationship between outdoor activities and bear attacks.11,12 Mauling by bears can lead to significant disabilities, affecting the victim’s ability to engage in previous occupations.
Our victims encountered bears during the daytime hours. The same time range was observed in 2 studies carried out in Sri Lanka and India.5,9 All of the encounters took place in unprotected areas (not in national parks or wildlife sanctuaries), indicating that bears venture from the protected areas to forage for food. Most human activities leading to conflict with bears happen during the daytime in the jungle. A single bear attacked in the majority of our cases, and similar patterns were observed in other studies.5,9,13–16 A single person and a solitary bear traveling in the jungle would not make much noise; therefore, the likelihood of encountering each other is high. In the encounters where cubs accompanied a female bear, she would have attacked without provocation to protect her offspring. The occasions on which two bears were involved were close encounters; therefore, the bears would have been startled, leading to an unprovoked attack.
In most of the incidents, the bear made a frontal attack; it was upright and made sweeping motions with its paws leading to facial and scalp injuries. This is typical of sloth bear attacks.8,9,16 Bears are intelligent; they attack the face to weaken the victim, who then cannot retaliate. 17 Most of our patients sustained injuries to multiple sites, although in other studies this ranged from 25 to 52%.9,14
Nine encounters were sudden, where the bear and the victim surprised each other; hence, these attacks could have been defensive. Sloth bears share the same habitats used by other large carnivores 18 and have adopted highly aggressive behaviors, such as standing on their hind legs, bellowing loudly, and rushing to deter the potential predator.5,9
In 4 of our patients, IV access was established at primary care hospitals. All of these patients sustained extensive injuries. Their condition may have deteriorated while being transferred since it took considerable time to transfer patients to the tertiary care hospital. Therefore, it was vital to establish IV access/IV fluid resuscitation at first contact to prevent or mitigate hypovolemia. Ideally the first patient should have had blood transfusion in the primary care hospital, but these hospitals do not have facilities to store blood and blood products.
Bears carry multiple microbes in their mouths. 19 Bear bites are usually deep and highly susceptible to developing anaerobic infections, including tetanus. 5 Wounds would have been contaminated with soil and other elements because of the ferocity of the altercations. Indications for antibiotic therapy are contamination, infected bites, fresh, large penetrating wounds, or full-thickness skin punctures. 20 Bear bites fulfill these criteria. Anticipating infections by aerobes and anaerobes, the patients received empiric broad-spectrum antibiotics. A tetanus toxoid was given, either at the peripheral hospital or the THA. Bears can potentially transmit rabies.21,22 Consequently, vaccines and immunoglobulin to protect against rabies were administered.
Irrigation of wounds with antibiotics solutions or saline, and wound debridement are key to successful wound management.20,22 Some injuries required special investigations and multidisciplinary team involvement. Therefore, bear attack victims should ideally be managed in a tertiary care hospital.
None of our patients died from their injuries. In comparison, in an Indian study, the mortality rate was 2 to 11%. 13 This difference could be because of several reasons. In Sri Lanka, some victims might have died or gone missing in the jungle, or there may have been under-reporting because victims who engage in illegal activities (eg, poaching or growing cannabis) would not come to the hospital for treatment.
The patient with pneumocephalus and cerebrospinal fluid rhinorrhoea was given empheric antibiotics and did not developed meningitis. This is in contrast to a Nepali study, in which a patient with pneumocephalus came to the hospital 24 h after the incident and subsequently developed meningitis. 23 Medical officers should be trained to identify the patients who are more prone to developing meningitis after bear attacks and administer antibiotics without undue delay.
This study raises a few important points in managing patients sustaining bear attacks in Sri Lanka. There is a lack of uniformity in the management. The most probable reasons are the nonavailability of necessary equipment and medications, lack of knowledge, and the absence of clear protocols and guidelines at the peripheral hospitals. A practical problem is the unavailability of data due to deficiencies in record keeping; as data are essential in making guidelines, improvements in record keeping must be addressed. Guidelines for the management of animal bites, especially with regards to IV access, administration of tetanus toxoid, antibiotics, analgesics, control of hemorrhage, and expedited transfer to a tertiary care hospital should be developed and implemented. Furthermore, ensuring the continuous availability of essential medications, dressings, and other equipment is a necessity. Medical officers and the supporting staff working in peripheral hospitals should be trained in the initial management of acute trauma patients. At the tertiary care centers, protocols should be made on subsequent management regarding investigations, timely referrals, multidisciplinary team approaches, timing, and the extent of wound management.
Conserving the Sri Lankan bear while reducing the mortality and morbidity to the humans is a daunting task. Minimizing human–bear encounters is the key strategy. Even though there is no consensus on the best protective action against sloth bear attacks, several measures could be adopted to mitigate human–bear conflicts. People can make noises while traveling in areas where encounters with bears are more likely, or when searching for common food sources, such as bee honey and fruits. In fact, the Veddas (indigenous people living in Sri Lanka) either shout or chant in loud voice when they travel in bear-infested terrain, giving bears ample warning to move away. 24 Bears are reluctant to attack humans who travel in groups.5,25 When venturing into a forest, travel as a group and when moving apart, keep in touch with each other by verbal communication or visual sighting. If a bear is seen at a distance, avoid it by quietly moving out of the way.5,25
Finally, communities should be educated regarding the unique status and value of the Sri Lankan sloth bear and the vital role it plays in maintaining ecological balance.
Limitations
The limitations in our study were that, compared with other studies, our numbers were small, making the comparisons and conclusions challenging. Another limitation of this study was the retrospective nature of some of the events, which were subjected to recall bias. There were also a few inadequacies in the data because of gaps in record maintenance. A few patients did not come for follow up or respond despite repeated attempts to contact them.
Conclusion
In our study, the attacks occurred during daytime, across all seasons, in the forest or its vicinity. Most of these encounters were unexpected. The majority of the attacks were frontal, leading to extensive soft tissue injuries in the upper torso.
Footnotes
Acknowledgments
The authors especially thank the editorial team and the anonymous reviewers of Wilderness & Environmental Medicine journal for their valuable comments and suggestions to improve this manuscript.
Authors Contributions: Study concept (SPBT); management of patients (SPBT, AS, VC); literature review and drafting and editing of the manuscript (SPBT, BTBW); all authors approved the final manuscript.
Financial/Material Support: None.
Disclosures: None.