
Abstract
There is little information in the literature on the safety of reascent to high altitude shortly after resolution of severe acute altitude illness, including high altitude pulmonary or cerebral edema. We present a case of a 52-y-old male climber who was diagnosed with high altitude pulmonary edema during the 2018 Everest spring climbing season, descended to low altitude for 9 d, received treatment, and returned to continue climbing with a very rapid ascent rate. Despite a very recent history of high altitude pulmonary edema and not using pharmacologic prophylaxis over a very rapid reascent profile, the climber successfully summited Mt. Everest (8848 m) and Lhotse (8516 m) without any problems.
Introduction
High altitude pulmonary edema (HAPE) is a life-threatening form of high altitude illness. It usually occurs at altitudes above 2500 m, but cases have been reported as low as 1400 m in patients with congenital unilateral absence of a pulmonary artery. 1 The incidence of HAPE has been estimated at 0.01 to 15% across studies, with the variability in reported rates a function of the altitude at which HAPE was assessed and the rate of ascent. Among trekkers and mountaineers in the Himalayas and Alps with a rate of ascent of >600 m·d-1, the incidence is around 4%. 2 If left untreated, this noncardiogenic form of pulmonary edema carries a fatality rate of around 50%. 3
HAPE is defined by at least 2 symptoms (dyspnea at rest, cough, weakness or decreased exertional performance, chest tightness or congestion) and at least 2 signs (crackles or wheezing, central cyanosis, tachypnea, or tachycardia). 4 Although there has been considerable progress in knowledge about the risk factors, pathophysiology, diagnosis, and treatment of HAPE, there are no published guidelines on the safety of return to high altitude immediately after illness. The Wilderness Medical Society guidelines for prevention and treatment of acute altitude illness mention that return to high altitude may be considered when symptoms of HAPE have resolved, there is no requirement for supplemental oxygen at rest or with mild exercise, and all vasodilator therapies have been stopped. 5 Because there is little information in this area, physicians lack guidance on how to counsel people who want to reascend shortly after severe high altitude illnesses, including HAPE.
We present a case of a climber who was diagnosed with HAPE during the 2018 Everest spring climbing season, descended to low altitude, received treatment, and returned to continue climbing. Despite having recently experienced HAPE, the climber successfully summited Mt. Everest (8848 m) and Lhotse (8516 m) without further problems.
Case report
This is a case of a previously healthy 52-y-old male who lives at an altitude of about 800 m. He had previous mountaineering experience climbing several 6000 to 7000 m peaks in the Karakoram and Tian Shan ranges. The highest altitude he had previously attained was 7546 m on Muztagh Ata. He had no history of altitude illness in his past climbing experiences. He had trekked to the Everest Base Camp (EBC) early in the season following a standard itinerary. He had taken 9 d to arrive to EBC (5360 m) from the trailhead at Lukla (2800 m) without any health issues and, in particular, no signs of any upper respiratory tract infections.
After a week at the EBC, he flew to the United Kingdom to participate in the London Marathon, completed it, and remained in London for a week. After this he flew to Tibet, stayed there for 3 d, visited the northern base camp of Mt. Everest (5150 m) by road, and then flew to Kathmandu (1400 m).
Soon after his arrival in Kathmandu (1400 m), he flew on a helicopter to Lukla and then from Lukla to EBC (5360 m) the same day. The total gain of elevation was 3960 m in a day. He had not taken any medication because he believed he was already acclimatized.
The next morning an emergency call was made by his guide to the volunteer doctors at the Himalayan Rescue Association EBC Clinic because the climber had developed severe headache, bad cough, and shortness of breath on minimal exertion, all of which had started and progressed overnight. He had a pulse rate of 100 beats·min-1, temperature 37.3°C, respiratory rate 20 breaths·min-1, and oxygen saturation 63% breathing ambient air. He was not cyanotic but was dyspneic with minimal activity, such as walking to the toilet tent. On examination, diffuse crackles were heard in both lungs. Cardiac examination was normal except for tachycardia. With a clinical diagnosis of HAPE, he was started on oxygen at 2 L·min-1, advised to rest completely, and given nifedipine 20 mg immediate release, acetazolamide 250 mg, and paracetamol (acetaminophen in the United States and Canada) 1 g orally.
After 2 hours, the climber was evacuated by helicopter to Kathmandu and was seen at a hospital there. At the hospital in Kathmandu, his oxygen saturation was 90% breathing ambient air. The headache had decreased, but crackles were still present on auscultation of the chest. Radiograph of the chest showed evidence of bilateral opacities, more on the right side, normal heart size, and fluid in the right minor fissure (Figure 1). All other investigations were normal. He was discharged without any medication and with advice to follow up in 2 wk. After 9 d, symptom free, his radiograph was repeated, and it was normal (Figure 2). He was not using supplemental oxygen and was not on vasodilators. The next day, he made another helicopter flight from Kathmandu to the base camp with a stopover of a few minutes at Lukla, a gain of 4000 m in an hour. He was not on any drugs for prophylaxis. He did not go for the customary acclimatization climbs as other climbers do but attempted a summit push. His climbing route took him to Camp II (6400 m) on the first day. After spending the night at Camp II, he climbed to Camp III (7100 m) and spent 2 nights there After 2 nights at Camp III, he climbed to Camp IV (8000 m) and spent another night and an entire day there before the push for the summit of Mt. Everest. He was on supplemental oxygen beyond Camp III. He successfully summited Mt. Everest (8848 m) 5 d after leaving the EBC with an average gain of 690 m per day. He followed that by summiting Lhotse (8516 m) in the next 48 h. After descending to the base camp, he ran the Everest Marathon (42 km) from EBC to Namche Bazaar (3400 m).
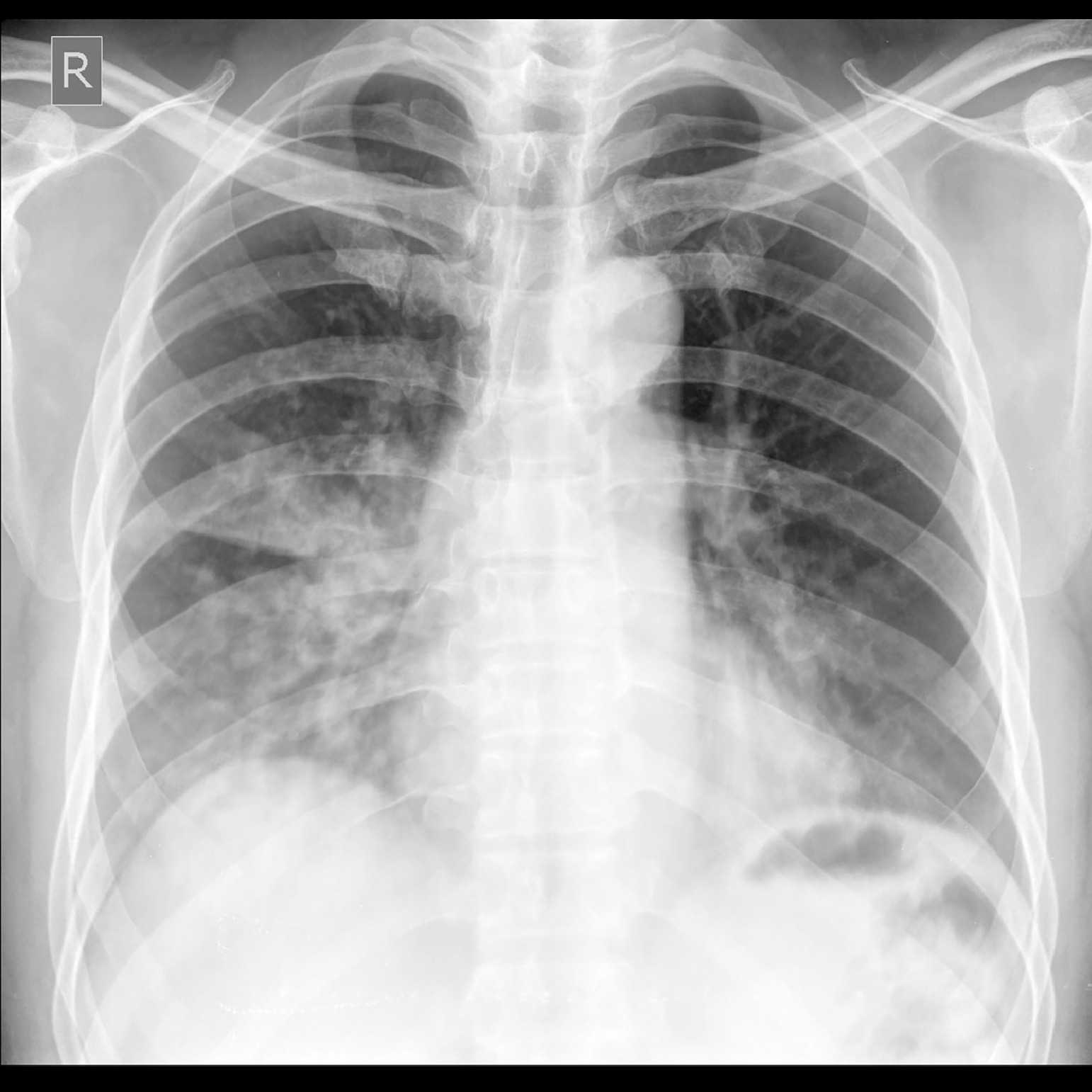
Chest radiograph showing bilateral opacities, more prominent on the right side; normal heart size; and fluid in the right minor fissure on first arrival to the hospital. Features are suggestive of high altitude pulmonary edema.
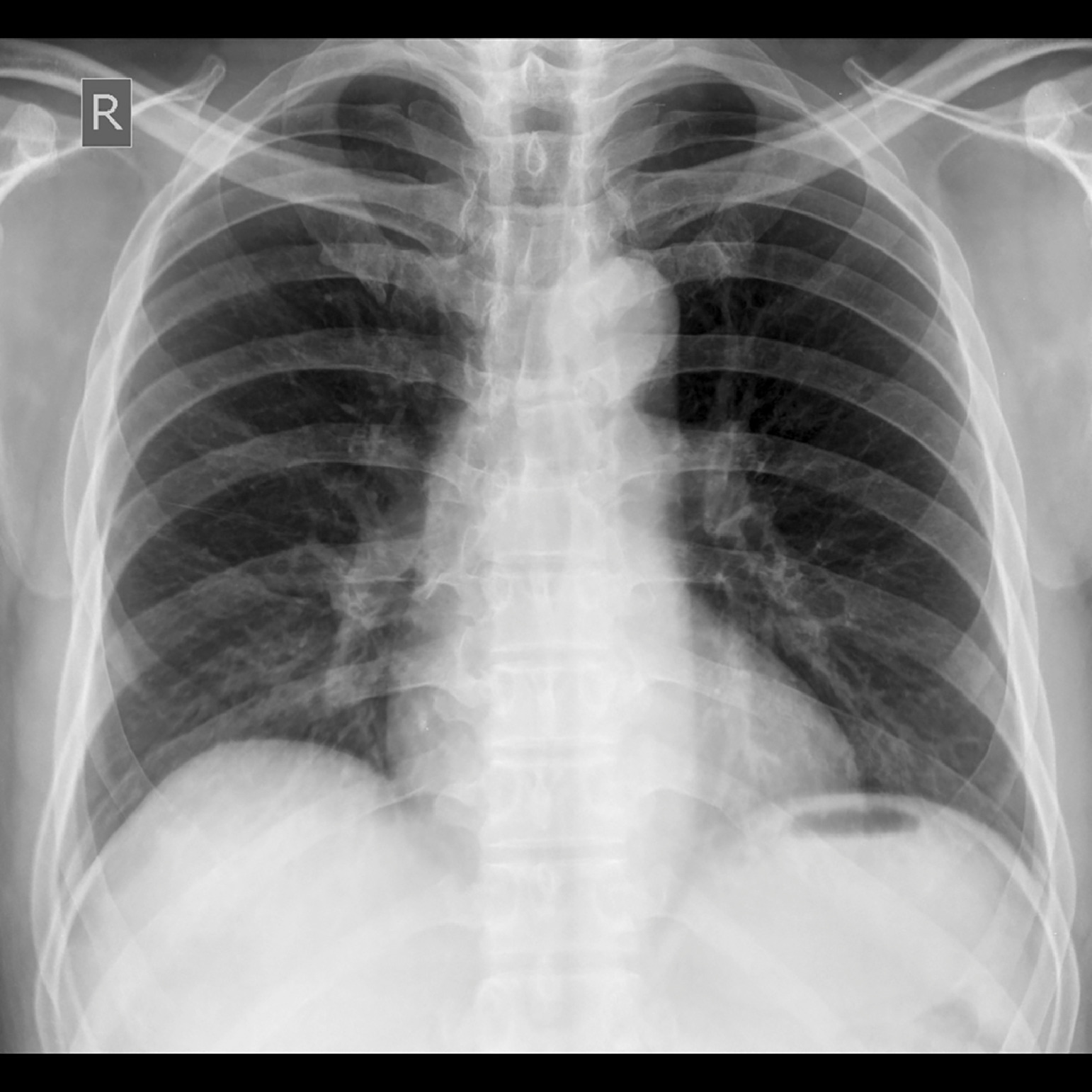
Complete resolution of radiographic changes seen in Figure 1 after 9 d at lower altitude.
Discussion
This case describes a previously unreported situation in which a climber with very recent HAPE successfully summited two 8000 m peaks despite a very fast ascent profile without pharmacologic prophylaxis. A search of the existing literature revealed a single case report and a case series of 3 climbers who made successful reascents after recent HAPE, with only 2 who reached altitudes above 8000 m.6,7 The case report describes a successful ascent of Mt. Everest after HAPE at Camp II (6600 m) on one of the acclimatization climbs. The climber descended to EBC, received treatment, trekked further to Namche (3400 m), and on his reascent 10 d later was taking prophylaxis with sildenafil, acetazolamide, and salmeterol/fluticasone. He summited 21 d after his initial illness without a recurrence of HAPE. 7 Of the 3 cases in the case series, only 1 case is of a successful summit of Everest; the other 2 involve a case from Denali (6200 m) and a case from Kalapathhar (5550 m). 6 In all of these cases, after the initial episode of HAPE and treatment, the reascent followed a conservative ascent profile. The case from Kalapathhar, the climber only ascended an average of 350 m·d-1.6,7 In all of the successful reascents noted, the individuals reached an altitude higher than that at which they initially developed HAPE.6,7 The case we describe is different in that the reascent to EBC followed a very rapid ascent profile. In the 2 cases of successful ascents of Everest, each climber had made acclimatization climbs as high as 6600 m before becoming ill with HAPE.6,7 That was not the case in this report; the climber became ill before starting any acclimatization rotation. The case described in this report is different in that the climber had a very rapid reascent profile, did not take any medication for prophylaxis against HAPE, and reached the summits of two 8000 m peaks after reascent. The reascent and eventual summits were successful despite the climber having at least 3 risk factors for acquiring HAPE: rapid ascent profile, history of HAPE, and very strenuous physical activity at high altitude. 8
A detailed description of the pathophysiology of HAPE is beyond the scope of this report. Briefly, HAPE is thought to result from exaggerated hypoxic pulmonary vasoconstriction, elevated pulmonary hydrostatic capillary pressure, stress failure of the pulmonary capillaries, and decreased alveolar fluid clearance with rapidly reversible damage to pulmonary capillaries.2,9–12 Looking at the literature, there is information on the risk of recurrence of HAPE with reascent in the future, with studies reporting recurrence rates of 13 to 60%.13,14 In all these reports, however, the reascent took place months to years after the initial episode of HAPE. 13 –15 There is no information in the literature on the risk with immediate reascent after HAPE. Although our report and the others in the literature suggest immediate reascent may be possible without recurrence, the true risk of recurrence remains unknown.
The current case report and the other 4 cases show that is possible to reascend safely soon after recovering from HAPE, at least under some circumstances. However, climbers should not adopt this as standard practice. In 4 of the 5 instances of successful reascent, the individual followed a conservative ascent profile. One climber also used prophylactic medications.6,7 Although some individuals have excessive pulmonary vascular responses to exercise or hypoxia and have a predilection for developing HAPE upon reascent, some individuals develop HAPE only once in the setting of other predisposing factors, such as a viral illness, and do not develop HAPE again when they reascend.
In the absence of systematic studies, a cautious approach is warranted. Climbers should be symptom-free off medications and supplemental oxygen, should make efforts to use a slow ascent rate, and should strongly consider use of pharmacologic prophylaxis with reascent. Climbers should also take into consideration the risks on the safety and well-being of the entire expedition with rapid reascents.
Footnotes
Acknowledgments
We express our gratitude to Dr. Buddha Basnyat for his assistance in manuscript write-up and invaluable comments in helping finish the article.
Author Contributions: Study concept and design (SD); drafting of the manuscript (SD); critical revision of the manuscript (SA); approval of final manuscript (SD, SA).
Financial/Material Support: None.
Disclosures: None.