
Abstract
Extremities are the area of the body most commonly affected by frostbite, which can also affect the face, ears, perineum, or genitals. Optimum management has moved away from early amputation and debridement toward maximizing tissue preservation and delaying surgical intervention. Increasing length of digit amputation increases morbidity, in terms of loss of hand function, experienced by patients. Reconstruction of affected digits is limited by bone necrosis, which often leads to shortened residual stumps and limited functional outcomes. This case describes the management of a severe frostbite injury affecting both hands and feet in a 39-y-old man, sustained during descent of Mount Everest. The use of a pedicled abdominal flap to provide soft-tissue cover permitted optimized digit length and function and sensate digits. The case highlights the benefits of early multidisciplinary team involvement in the management of severe frostbite to optimize functional outcome.
Introduction
Frostbite is defined as a cold thermal injury occurring in tissues exposed to temperatures below their freezing point, typically –0.5°C. Frostbite can also occur during sustained nonfreezing cooling at temperatures of up to +2°C. 1 Historically prevalent in military populations, it has become increasingly common in civilian populations exposed to extreme cold through occupation (handling of liquid CO2 or NO2), recreation (winter sports and mountaineering), homelessness (inadequate clothing and shelter for environmental conditions), and substance abuse (impaired decision making and lack of capacity to seek shelter).2,3 The extent of injury depends on numerous factors, including outright temperature, wind chill, length of exposure, wet/dry exposure, adequacy of clothing, nutritional status, individual susceptibility, and comorbidity, notably peripheral vascular disease and neuropathies.4,5
The management of frostbite can be divided into prehospital and hospital phases. The focus of prehospital care is moving the patient out of the exposed environment, local rewarming, and prevention of refreezing injury.6,7 Aspirin and ibuprofen have been shown to be of benefit because of their respective rheologic and prostaglandin effects, which inhibit platelet aggregation. 8 Once in the hospital, management should focus on correcting systemic hypothermia, after which a detailed assessment of the affected area should be performed. Imaging options provide information on tissue perfusion and bone viability. 9 If the injury is less than 24 h old, thrombolysis with tissue plasminogen activator should be considered. 9 Iloprost infusion is associated with vasodilatation and platelet inhibition and has been found to reduce the need for amputation.10,11 Hyperbaric oxygen therapy has also been found to decrease ischemia-reperfusion injury and accelerate demarcation between viable and nonviable tissue. 12
Classification systems in use include those by Cauchy et al, who classified injury severity by clinical and radiological findings on day 2 postinjury (Table 1). The need for urgent amputation is rare and its use is contraindicated before detailed imaging, to permit complete demarcation of viable tissue. 13
Classification of frostbite*
Adapted from Cauchy et al. 24
Case Report
A right-hand–dominant, 39-y-old man experienced prolonged exposure during descent from a successful attempt to summit Mount Everest (8848 m), sustaining severe frostbite injuries to both hands and feet. Rewarming was initiated on the South Col (7950 m). After delayed evacuation, he was managed with further rewarming and iloprost infusion on days 4 to 9 postinjury, followed by hyperbaric oxygen therapy. After demarcation of the injury and visible ongoing necrosis, advice was sought via the British Mountaineering Council Frostbite e-referral system (

Initial assessment in the UK. On the left hand, dry, clean necrosis of the distal thumb; the first digit extending to the proximal interphalangeal joint; and the second, third, and fourth digits to the metacarpophalangeal joints. On the right hand, the thumb was unaffected; however, all the other digits exhibited dry and clean necrosis extending to the metacarpophalangeal joints. These areas of necrosis were well demarcated by this time.
Technetium-99 scanning revealed nonviable bone in the proximal phalanges of the fingers and toes, except for the thumbs (grade 4 frostbite injury; Table 1). Damage to the toes prevented their use as donor sites. Multidisciplinary discussion took place with the patient, including a vascular surgeon, plastic surgeon, and hand physiotherapist, giving priority to the patient's dominant right hand. The tissues were allowed to demarcate fully over several weeks.
It was evident that complete debridement would leave bone exposed without adequate soft-tissue coverage (Figure 2). To maximize remaining digit length, use of a pedicled abdominal flap was chosen (Figures 3 and 4). An interval of 4 wk allowed sufficient neovascularization of the flap before division and skin grafting of raw areas (Figure 5). Importantly, a second technetium-99 scan identified viability of the previously ischemic bone. Salvage of the ischemic bone and soft-tissue grafting permitted an additional 1 cm of digital length for each finger treated. Sensitivity to pressure, pain, and temperature was preserved and has permitted subsequent mountaineering expeditions, including an ascent of the Matterhorn (4478 m) 13 mo after the injuries discussed here.
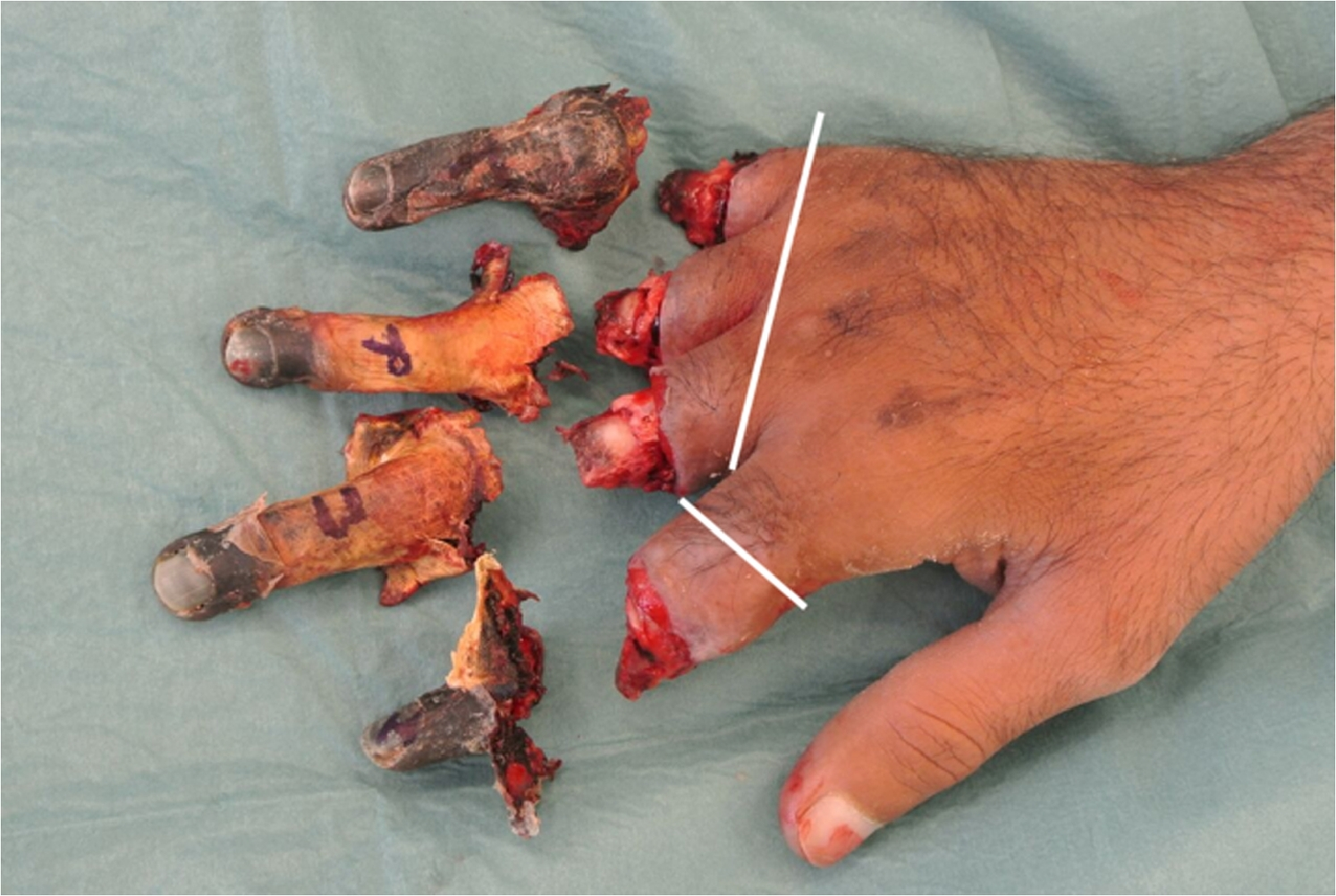
Amputation levels of fingers on right hand. White lines indicate where the treating team considers level of amputation would have been had the described technique not been employed.
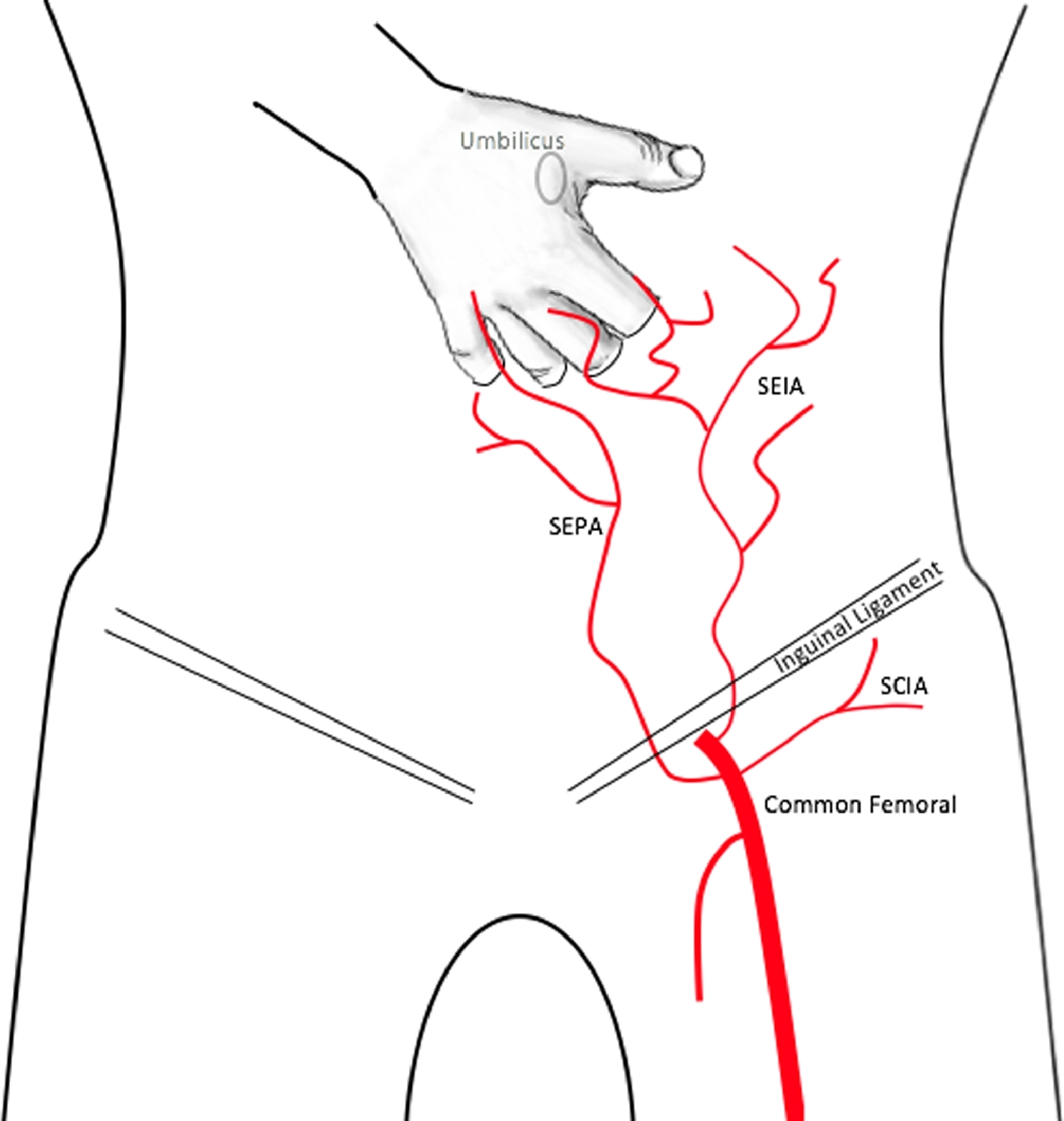
Diagrammatic representation of vascular supply to a pedicled flap. Adapted from Sabapathy and Bajantri 2014. 25 SEPA, superficial external pudendal artery; SIEA, superficial inferior epigastric artery; SCIA, superficial circumflex iliac artery.

Hand immediately after finger implantation.

Right hand after explantation and skin closure, demonstrating preserved stump length.
Discussion
Approximately 45,000 finger amputations are performed each year in the United States. 14 Studies of patient-reported outcomes show less than half of patients who have undergone a partial hand amputation are able to return to work and that they report significant psychosocial morbidity.14,15 Prosthetic replacement is possible, but functional options are limited. Therefore, preservation of finger stump length is key to maintaining hand function and limiting the functional and psychological impact of digit loss.
The use of a pedicled flap was first described in 1932. 16 In the context of complex and/or multiple hand or forearm injuries, such as partial traumatic amputation, crush injuries, degloving, or burns, 17 a pedicled groin flap has traditionally been the procedure of choice to restore skin coverage. The advent of microsurgical free-tissue transfer has reduced the need for this technique. Because of necrosis of the patient's toes, toe-to-hand transfer was not an option. In addition, a forearm flap was inadequate to provide complete tissue coverage.
The vascular supply to the anterior abdominal wall comprises the cutaneous branches of the superficial inferior epigastric artery, the superficial external pudendal artery, and the superficial circumflex iliac artery.18,19 In this case, the flap procedure was 2-staged. Stage 1 required raising of the flap around a vascular pedicle, after which the recipient site was implanted to allow new vascular ingrowth (approximately 3 wk, although shorter division times have been reported). 20 Once the new blood supply was dominant, the native vascular pedicle could be safely divided without rendering the flap ischemic. This freed the recipient site from the donor site, and the flap could then be closed over the site of the original injury (stage 2) (Figures 4 and 5). One advantage of implanting the digits separately rather than raising a single flap is the avoidance of the need for temporary syndactilization, thus decreasing the operating time and surgical morbidity of a further procedure to separate the digits. Reports of discomfort and shoulder stiffness during arm immobilization are common.21,22 Total immobility of the limb is paramount to allow neovascularization to occur. This can be achieved with the help of bandaging or, if needed, external fixation. 17 Postoperative physiotherapy and occupational therapy are vital to aid successful functional outcomes for patients in adapting to new finger length and functionality. 23
Conclusions
This case demonstrates the use of a pedicled abdominal flap after severe frostbite injury. The benefits of this technique include maximization of residual digit length and functionality as well as complete soft-tissue coverage. The importance of preserving as much viable, sensate digit length for future dexterity, hand function, and quality of life in patients requiring multiple, bilateral digital amputations cannot be underestimated. A fit, motivated patient and early involvement of a specialist multidisciplinary team were key to a successful outcome in this case.
Footnotes
Acknowledgments
The authors would like to thank the teams at Everest ER and the CIWEC clinic, Kathmandu, for their initial medical intervention and assistance in this case.
Author Contributions: Concept and design (CHEI); acquisition of data (MRV, CHEI); drafting of the manuscript (OLF); critical revision of the manuscript (RAB, MRV, CHEI); final approval of the manuscript (OLF, RAB, MRV, CHEI).
Financial/Material Support: None.
Disclosures: None.