
Abstract
Introduction
To explore baseline knowledge about avalanche guidelines and the Avalanche Victim Resuscitation Checklist (AVReCh) in Italy and the knowledge acquisition from a standardized lecture.
Methods
Standardized lecture material discussing AVReCh was presented during 8 mountain medicine courses from November 2014 to April 2016 in different regions of Italy. To determine the knowledge acquisition from the lecture, a pre- and postlecture survey was utilized.
Results
A total of 193 surveys were analyzed. More than 50% of the participants had never participated in lectures/courses on avalanche guidelines, and less than 50% of the participants knew about the AVReCh before the lecture. The correct temporal sequence of reportable information in the basic life support section of the AVReCh was selected by 40% of the participants before the lecture and by 75% after the lecture (P<0.001). Within subgroups analysis, most groups saw significant improvement in performance (P<0.05). The selection of the correct burial time increased from 36 to 84% (P<0.05).
Conclusions
Health care providers and mountain rescue personnel are not widely aware of avalanche guidelines. The standardized lecture significantly improved knowledge of the principles of avalanche management related to core AVReCh elements. However, the effect that this knowledge acquisition has on avalanche victim survival or adherence to the AVReCh in the field is yet to be determined.
Introduction
With increases in winter sport participation, there has been increased exposure to avalanche danger. In an avalanche, demands for field rescue commonly overwhelm resources, leading to increased morbidity and mortality. The International Commission for Mountain Emergency Medicine (ICAR MEDCOM) has published official consensus guidelines for the onsite treatment of avalanche victims, 1 and the International Liaison Committee on Cardiopulmonary Resuscitation has included specific recommendations in cardiopulmonary resuscitation guidelines 2 to provide guidance to health care providers and mountain rescue personnel. The Wilderness Medical Society has also recently published practice guidelines for prevention and management of avalanche snow burial accidents. 3
A recent study performed in the European Alps found poor compliance with the ICAR MEDCOM guidelines from 1996–2009, with insufficient transfer of information from the accident site to the hospital. 4 The 2 principal concepts in avalanche survival are burial time and airway patency with presence of an air pocket.2,5 From early data on avalanche survival, it is evident that most victims die from asphyxiation within 35 min of burial. 6 Recently, core temperature (≤30°C) and serum potassium (≤8 mmol·L−1) have been included in the guidelines as prognostic factors for survival. 2 ,3,7 Based on the guidelines, the ICAR MEDCOM created an Avalanche Victim Resuscitation Checklist (AVReCh) in 2014 in an attempt to improve the quality of prehospital patient care (Figure 1).8,9 The checklist concept has been promoted by the World Health Organization since 2008 due to its potential to improve quality of patient care, being a robust and widely applicable tool. 10 AVReCh details a low probability of survival in avalanche burial victims with completely obstructed airways, a burial time of >60 minutes, and/or serum potassium >8 mmol·L−1. 2 ,3,9 Strict adherence to the AVReCh (basic life support [BLS] and advanced life support [ALS] sections) can streamline avalanche victim management.
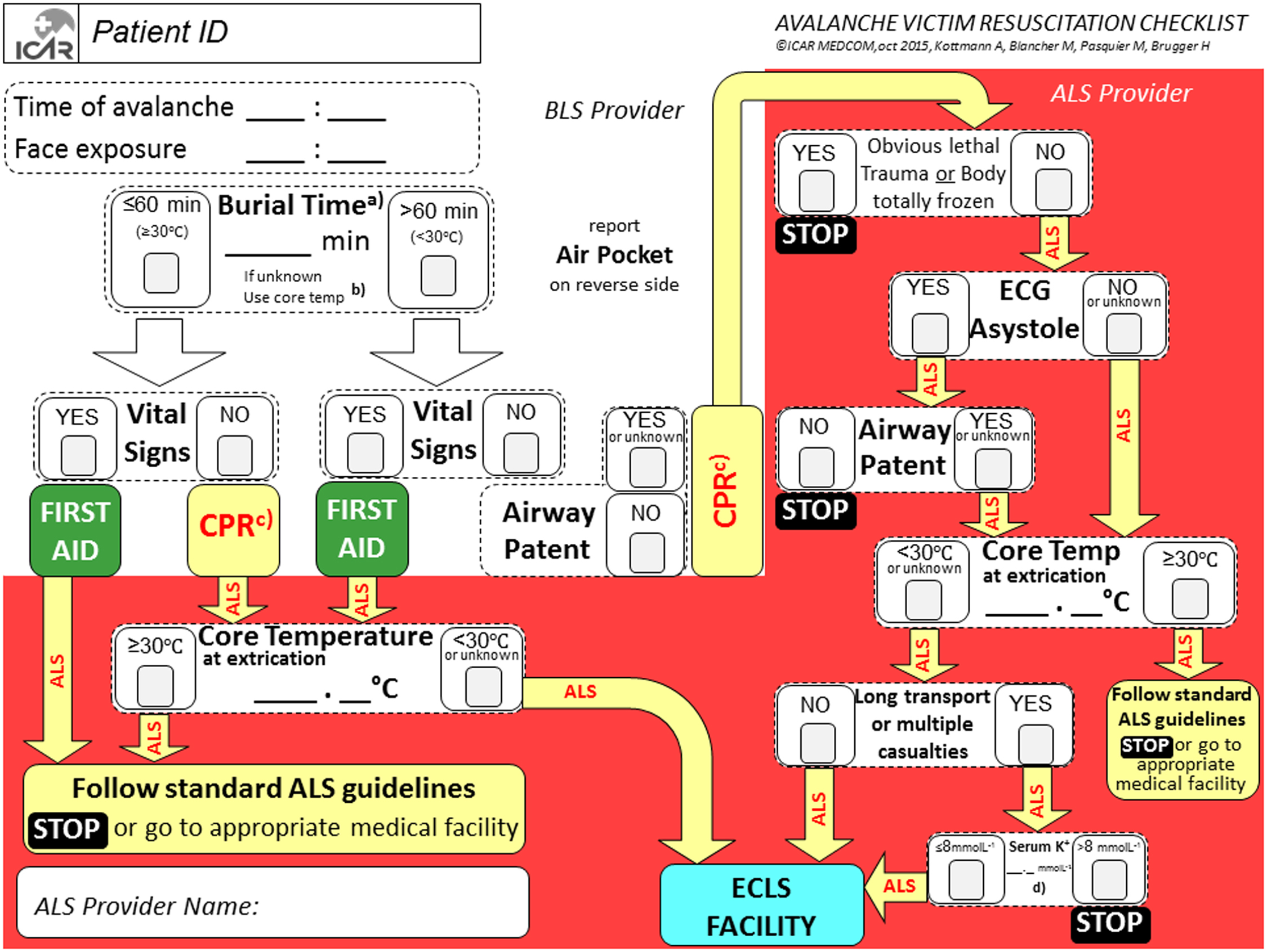
Avalanche Victim Resuscitation Checklist. The white section is addressed to a basic life support–trained first responder, the red section to an advanced life support–trained health care provider. Patient ID, patient identity; CPR, cardiopulmonary resuscitation; BLS, basic life support; ALS, advanced life support; ECLS, extracorporeal life support (cardiopulmonary bypass/extracorporeal membrane oxygenation). A, Time between burial and uncovering the face. B, If duration of burial is unknown, core temperature using an esophageal probe may be substituted in patients in cardiac arrest. C, Cardiopulmonary resuscitation can be withheld if there is an unacceptable level of risk for the rescuer, total body freezing, or obvious lethal trauma (decapitation, truncal transection). D, If potassium at hospital admission exceeds 8 mmol·L−1, consider terminating resuscitation (after excluding crush injuries and consideration of the use of depolarizing paralytics). Modified from Kottmann et al.8,9 with permission from Elsevier.
The aim of the current study was to explore baseline knowledge about avalanche guidelines and the Avalanche Victim Resuscitation Checklist in Italy and knowledge acquisition from a standardized lecture about the AVReCh.
Methods
After the ICAR MEDCOM released standardized lecture material discussing the AVReCh, a 1-hour lecture (based on ICAR MEDCOM material) was presented during 8 mountain medicine courses organized by either the CNSAS-Italian Mountain Rescue or SIMeM-Italian Society of Mountain Medicine. The lecture included information about the BLS and ALS management of avalanche victims and practical training (ie, inserting essential information from standardized examples in a training AVReCh). Specifically, 1 pilot lecture was held at the end of 2014 in Trentino Alto-Adige, Italy, and the other 7 lectures were consecutively held in the winter season of 2015–2016 in different regions of Northern and Central Italy (Abruzzo [1], Emilia Romagna [2], Piemonte [1], Trentino Alto-Adige [2], and Veneto [1]). The lecture was presented by the same member of the ICAR MEDCOM (G.S.).
To determine the knowledge acquisition resulting from this lecture on avalanche resuscitation guidelines, all participants received a pre- and postlecture survey that was developed by the authors. The evaluation time was 15 minutes each. The survey was anonymous, and participants were given an identifying number to facilitate pre- and postanalysis. Based on the study methods presented, the study was exempted from needing the approval of the local ethics board approval (0078304-BZ).
Participants included both novice and expert medical professionals, such as physicians/nurses and mountain rescue personnel, as well as laypersons (nonmedical/nonrescue persons). A total of 6 questions were included in the prelecture survey and 3 in the postlecture survey (see online Supplemental Material). Based on the survey, participants were classified as laypersons, mountain rescue technicians, BLS providers, and/or ALS providers, depending on the highest certification status.
The first 3 questions aimed to collect information regarding previous exposure to a lecture on avalanche guidelines, previous knowledge of the AVReCh, or participation in avalanche rescue. The subsequent 2 questions evaluated the knowledge acquisition from the lecture under investigation: i) the correct temporal sequence of reportable information in the BLS section of the AVReCh. The correct sequence was avalanche time, time of exposure of the victim’s face, airway patency/presence of an air pocket or vital signs, and then first aid/cardiopulmonary resuscitation; ii) the most critical time of avalanche-burial cutoff values. The correct answers were both 35 and 60 min (as guidelines were subsequently changed during the study period, with 35 min still representing the inflection point on the survival curve). 5 ,6,11 The last question aimed to determine the subjective relevance of the lecture for participants. On a 5-point scale (1–5) a score of 4 and 5 were considered relevant.
Data were recorded in an Excel spreadsheet (Microsoft, Redmond, WA) and were analyzed by a statistician (AES) blinded to the study. Data were analyzed using SPSS version 23.0 statistical software (IBM Corp, Armonk, NY). Absolute and relative frequencies were calculated to explore distributions of categorical variables. Subsequently, various 2-way tables were created, and appropriate tests of association were conducted. The values of the answers on the question about the most critical time of avalanche-burial cutoff values were collected as a scale variable. Subsequently, for the aim of the analysis, this variable was transformed in a nominal variable with 2 modalities (right, wrong). Differences between pre- and postlecture results were compared using Wilcoxon signed-rank test. For all tests, the significance level was set at 0.05.
Results
A total of 193 surveys (of the 201 obtained from lecture participants) were analyzed (96%). Eight surveys could not be analyzed because they lacked an identifying number. Participants of the course were ALS providers (47%), laypersons (25%), BLS providers (19%), and mountain rescue technicians (9%). Sixty-five percent of participants had never participated in lessons/courses on avalanche guidelines, and 76% had never participated in avalanche rescue. Only 34% of the participants knew about the AVReCh before the lecture. The correct temporal sequence of reportable information in the BLS section of the AVReCh was selected before the lecture by 40% of the participants—specifically, by 47% of the mountain rescue technicians and 43% of the BLS providers, followed by laypersons (40%) and ALS providers (39%). After the lecture, 75% of the participants gave the correct temporal sequence of reportable information in the BLS section of the AVReCh (P<0.001 comparing pre- and postlecture answers). Within subgroups analysis, most groups demonstrated significant improvement in performance (P<0.05) (Figure 2). The selection of the most critical time of avalanche-burial cutoff values increased from 36 to 84% (P<0.05). Ninety-four percent of participants believed the lecture was useful.
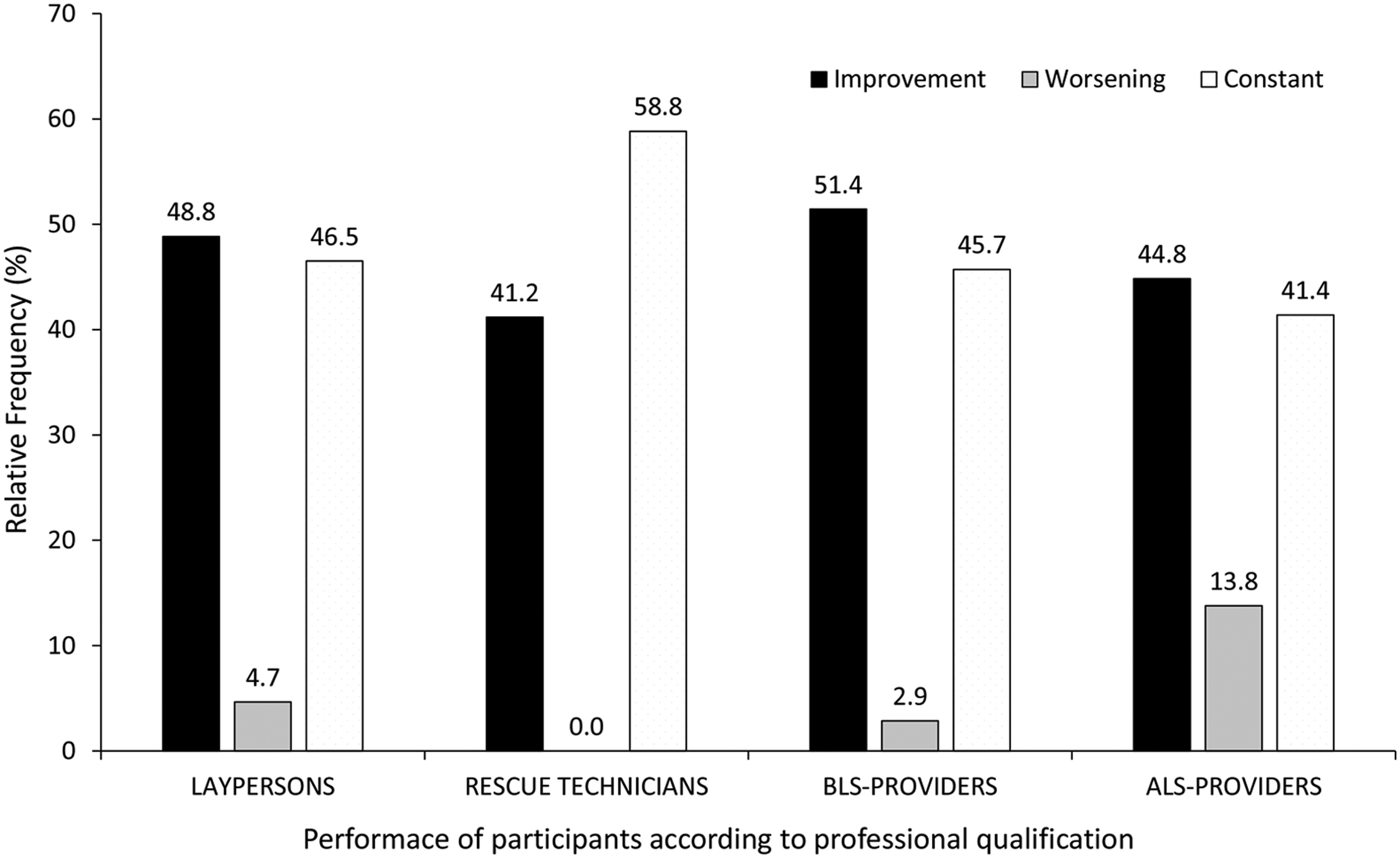
Subgroup analysis of performance changes (as a percentage) in the correct temporal sequence of reportable information in the BLS section of the AVReCh from pre- to postlecture survey. The correct sequence is avalanche time, time of exposure of the victims’ face, airway patency/presence of an air pocket or vital signs, and then first aid/cardiopulmonary resuscitation.
Discussion
The current study seeks to quantify for the first time baseline knowledge about avalanche guidelines and the effect on knowledge acquisition of AVReCh from a standardized lecture via a pre- and postlecture survey. Although existing avalanche management guidelines are simple, the results show that there is an apparent scarcity in avalanche training, even among health care providers interested in mountain medicine or operating in mountain areas and among mountain rescue personnel. However, the results revealed that knowledge of the principles of avalanche management can be improved with a standardized lecture proposed by the ICAR MEDCOM.
Half of the participants in the survey were ALS or BLS providers working in areas with a risk of being involved in a mountain rescue operation (for health care providers operating in helicopter emergency medical services) or were responsible for the downstream care of a patient evacuated from mountain areas. Most helicopter emergency medical services bases operating in the Italian Alps and Apennines are, in fact, specialized in search-and-rescue (SAR) missions, and a mountain rescue technician is part of the team. 12
The survey, together with previous studies, 4 is a testament to the lack of knowledge that prehospital personnel have in avalanche rescue and justifies the need for specific training with standardized lectures to facilitate appropriate prehospital management of specifically mountain-related injuries. In turn, personnel can identify hypothermic victims eligible for prolonged resuscitation (extracorporeal rewarming or possibility for good outcome) vs asphyxia-induced out-of-hospital cardiac arrest (low chance of survival). 2 ,3,8,9 In a previous study, burial duration was documented in 91% of completely buried avalanche victims, and airway status was unknown in 24% of long burial cases. 4
Although ALS providers onsite were more likely to follow the consensus guidelines in prehospital management, the rate of incorrect triage decisions onsite was still high. 4 In fact, onsite decision making by the prehospital ALS providers often occurs with incomplete information, either secondary to delay in arrival or because of the reliance on information gathered by laypersons (eg, winter recreationists) or BLS providers. 13 Despite the national and international promotion over the past two decades, the scarcity of appropriate information acquisition underscores the need to improve education in avalanche rescue during mountain rescue or wilderness certification or first aid courses for winter recreationists. In fact, less than 50% of participants selected the proper sequence in the evaluation of an avalanche victim before the lecture.
International evidence-based guidelines, in combination with the AVReCh and a standardized lecture, seem to have the capability to improve knowledge of the principles of avalanche management. ICAR MEDCOM is disseminating the AVReCh in different local languages, evaluating its use within ICAR SAR organizations, and promoting surveillance of outcome measures at pilot sites. Moreover, dedicated training in avalanche rescue should not only be addressed to health care providers, but also to mountain rescue technicians (of all levels) and winter recreationists. Survival, in fact, depends largely on the immediate extrication of completely buried avalanche victims by bystanders before helicopter crew arrival (survival rate 74 vs 19%, respectively) 13 and on the appropriate transfer of information for onsite decision making. Moreover, it appears that participants believe the subject matter to be relevant, based on survey responses. The effect, however, that this knowledge acquisition has on avalanche victim survival is yet to be determined. The use of the theoretical knowledge can be very challenging in stressful prehospital scenarios like an avalanche. AVReCh (and a standardized lecture material)8,9 has been created to improve quality of patient care and retain essential decision making information in a special prehospital emergency scenario like an avalanche accident.
A significant limitation of this study is that it was performed in 1 country, and the results may not be generalizable to other countries. The study also only demonstrated that knowledge is improved immediately after the lecture, but whether this knowledge was retained for a longer duration of time is unknown.
As participation in winter sports grows, there is an increased possibility of avalanche accidents. First responders must obtain crucial information to facilitate the correct management of the victim/patient by prehospital emergency services. The guidelines for initial information gathering put forth by ICAR MEDCOM and the International Liaison Committee on Cardiopulmonary Resuscitation, however, are infrequently used in avalanche accidents. 4 Our study indicates a lack of knowledge of avalanche guidelines even in different regions with regular avalanche accidents and that a standardized lecture about the AVReCh can facilitate dissemination of these guidelines. Future areas of study will need to determine if participants will be able to use and correctly adhere to the checklist as first responders to an avalanche accident and determine if adherence to the AVReCh improves avalanche victim mortality.
Acknowledgments: The authors acknowledge Elsevier for the permission to reprint a modified version of the Avalanche Victim Resuscitation Checklist from Kottmann et al 9 .
Author Contributions: Study concept and design (GS, MM, HB); Acquisition of the data (GS, MM); Analysis of the data (GS, DF, AES); Drafting of the manuscript (GS, DM, DF); Critical revision of the manuscript (AES, MM, HB); Approval of final manuscript (GS, DM, DF, AES, MM, HB).
Financial/Material Support: None.
Disclosures: None.
Footnotes
Supplemental material
Supplemental material associated with this article can be found in the online version at
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.