
Abstract
To provide guidance to clinicians and avalanche professionals about best practices, the Wilderness Medical Society convened an expert panel to develop evidence-based guidelines for the prevention, rescue, and medical management of avalanche and nonavalanche snow burial victims. Recommendations are graded on the basis of quality of supporting evidence according to the classification scheme of the American College of Chest Physicians.
Introduction
Snow and ice avalanches are widespread in mountainous regions of the world. Worldwide avalanche-related morbidity and mortality are difficult to estimate due to the lack of reporting systems in many countries. Europe and North America have relatively accurate systems for capturing data on avalanche fatalities. Approximately 150 fatalities occur annually in Europe and North America. 1 –4 During the 31 winter seasons between 1983 and 2015, Europe and North America recorded 5123 avalanche fatalities, 5 about 165 deaths per year; most are from Europe, about 130 per year. In the same period an average of 24 people died in avalanches each winter in the United States and 12 in Canada. 5 Avalanche fatalities in mountain regions of other locales—for example, the Andes and the Himalaya—are not systematically recorded. However, the number of fatalities per year may be many times higher than fatalities officially recorded in Europe and North America. Catastrophic avalanches that killed over 10 persons, for example, include the serac fall in Nepal in 2014 and the earthquake in Nepal in 2015. Nonfatal avalanche events are extremely difficult to quantify because many accidents are not reported and organized search and rescue teams are not activated.
Most documented North American and European avalanche fatalities occur in recreational user groups such as snowmobilers, skiers, snowboarders, mountaineers, and snowshoers. Occupational-related avalanche fatalities among ski patrollers, mountain rescuers, mountain guides, and transportation workers occur less frequently, although job requirements may place these personnel at higher and more prolonged risk. 1
Avalanche avoidance should be the main method to mitigate risk of injury and death. If an avalanche incident occurs, rescue by one’s companions—including appropriate resuscitation and advanced life support measures—are critically important to reduce avalanche morbidity and mortality.
Methods
The Wilderness Medical Society convened an expert panel to develop evidence-based recommendations for 3 primary aspects of avalanche accidents: prevention, rescue, and resuscitation. Nonavalanche deep snow and tree-well burial were included as related conditions with pathophysiology and recommendations similar to avalanche burial.
The PubMed database was searched using keywords including avalanche, snow burial, snow asphyxiation, and nonavalanche-related snow immersion death. Secondary references were also included. The panel mainly considered peer-reviewed randomized controlled trials, observational studies, case series, and case reports for inclusion. Only a limited number of studies of avalanche accidents have been published in the peer-reviewed academic literature, so conference proceedings, avalanche center data, letters to the editor, review articles, and books were included for background information. When no studies existed to provide evidence, the recommendations of the panel were based on review articles, textbooks, patient-care experience, and firsthand knowledge of equipment and techniques.
The panel developed recommendations by consensus. The panel graded recommendations based on the strength of the recommendation and the quality of evidence using the classification scheme of the American College of Chest Physicians (see online supplementary Table 1). 6 When no evidence existed, the panel made recommendations based on expert consensus.
Pathophysiology
Avalanche morbidity and mortality largely depend on duration of burial, patency of the airway, air-pocket volume, depth of burial, and traumatic injuries. The term
Asphyxia
Asphyxiation during avalanche burial occurs by 3 primary mechanisms: physical blockage of the upper airway caused by inhaled snow, ice mask formation, and oxygen deprivation due to rebreathing expired air. In addition, the weight and compaction of snow may limit chest expansion and impair ventilation, especially with heavy, dense snow, which is more common in a maritime snow climate and during spring conditions. 14
Complete obstruction of the upper airway by snow or debris results in hypoxia in <10 minutes and acute asphyxiation during the first 30 to 60 minutes of avalanche burial. If the airway is patent, ice mask formation occurs when water vapor in exhaled air condenses and freezes on the snow in front of the face, forming an impermeable barrier that prevents airflow. Because asphyxia is the major cause of death during avalanche burial, time to extrication is a foremost determinant of survival. According to Swiss data, completely buried avalanche victims had >90% chance of survival if they were extricated within about 15 minutes, but only a 30% chance of survival if they were extricated after approximately 30 minutes (Figure 1). 3 ,7,12
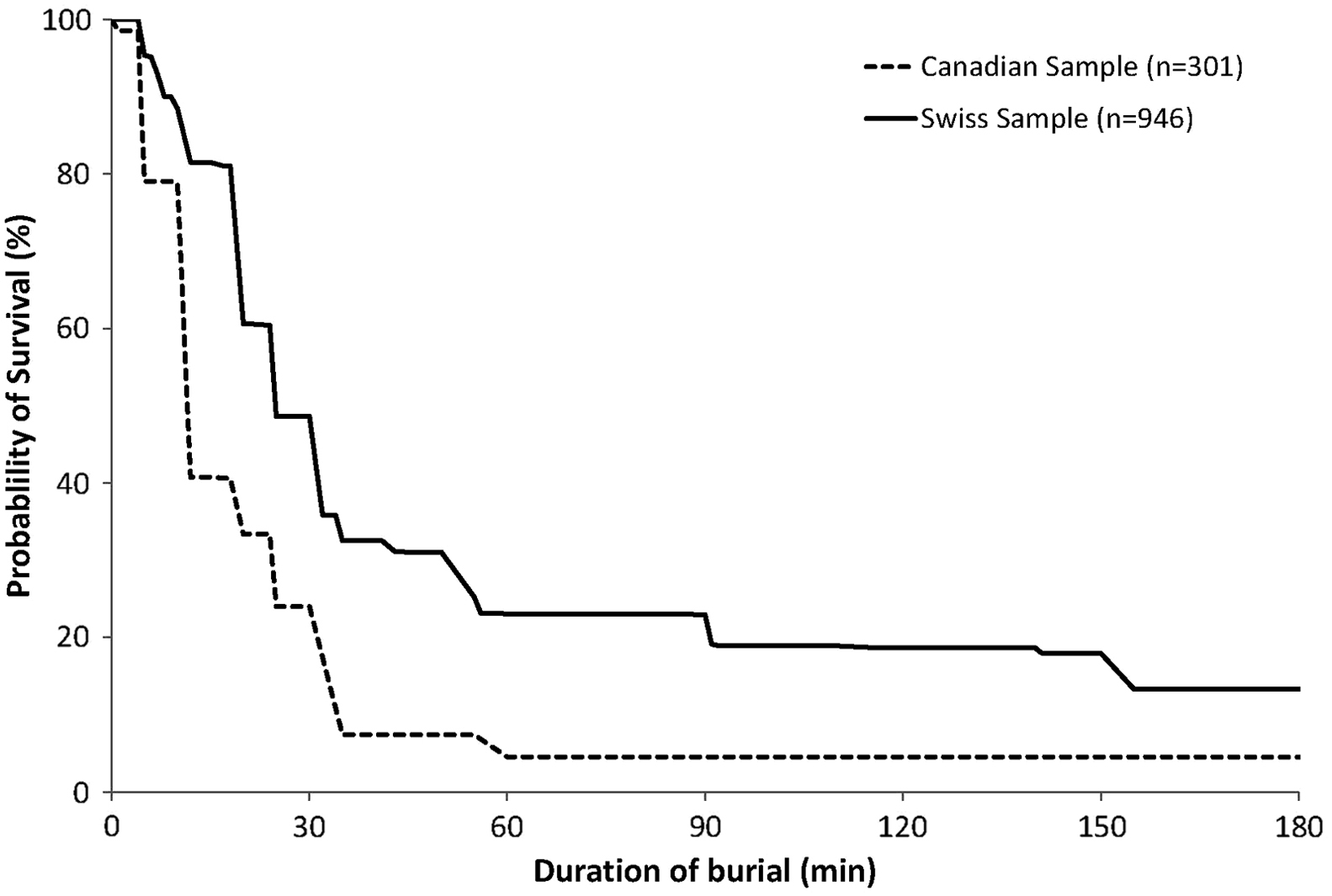
A comparison of the Swiss avalanche survival curve (bolded line) and the Canadian survival curve (dashed line) over the same 25-year period, from 1980 to 2015. Note the rapid drop after 10 minutes in the Canadian curve, although the curve maintains the same morphologic survival phases as the Swiss curve. 3
Survival of a buried victim after more than 30 minutes requires a patent airway and the presence of an air pocket. The larger the volume of the air pocket, the longer the duration of possible survival after burial. Inspired air contains 21% oxygen (O2) and less than 0.03% carbon dioxide (CO2). Expired air contains about 16% O2 and 5% CO2. Rebreathing expired air during avalanche burial results in a progressive decrease in the fraction of inspired oxygen (FIO2) and a progressive increase in the fraction of inspired carbon dioxide (FICO2). 8 ,19,20 Hypoxia and hypercapnia eventually cause death by asphyxiation unless an adequate air pocket exists or the victim is extricated before asphyxia can occur. A larger air pocket volume provides greater surface area for air flow, allowing expired CO2 to diffuse from the air pocket into the snowpack and O2 to diffuse from the snowpack into the air pocket. Snow density and porosity surrounding the air pocket also is a factor in the diffusion of gases, but their impact on survival is still not fully understood. 19 If the air pocket is large enough, asphyxiation is delayed and an avalanche victim may survive for many hours.8,20
Trauma
Trauma accounts for less than 25% of avalanche deaths in North America and Europe in avalanches that are triggered by recreational skiers, snowboarders, and snowmobilers. In catastrophic avalanches, such as those that occurred as a result of the earthquake in Nepal in April 2015 and in the Khumbu Icefall on Mount Everest in 2014, trauma often accounts for a higher percentage of fatalities. Traumatic deaths are associated with a wide range of injuries that depend on geographic differences in terrain features and snowpack. The proportion of avalanche deaths related to trauma in Canada has been reported to be higher than that in Europe and the United States. 9
Avalanche victims can sustain virtually any type of injury during the often-turbulent descent in an avalanche.13,15 Severe injuries are frequently caused by collisions with trees or rocks. Minor injuries likely remain unreported. The most common serious injuries are to the head, cervical spine, chest, and extremities.9,13 In an analysis that examined closed head injuries in avalanche victims, evidence of traumatic brain injury was found in the majority of those studied. An altered level of consciousness could further decrease survival by accelerating asphyxiation. 21
Hypothermia
In victims of avalanche burial who are extricated alive, hypothermia can complicate other conditions such as asphyxia and trauma. Hypothermia causes few fatalities in avalanche victims because death from asphyxia usually occurs before death from hypothermia.2,22 The severity of hypothermia is best determined by core temperature measurement in the field. 23 If core temperature cannot be measured in the field, the severity of hypothermia can be estimated in the field as mild, moderate, or severe using Wilderness Medical Society (WMS) Practice Guidelines for the Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia. 23 The Swiss classification system—grades I to IV—can also be used.23,24 The Swiss system associates level of consciousness, presence or absence of shivering, and presence or absence of additional vital signs with ranges of core temperature, yielding a rough clinical estimate of the grade of hypothermia. 25 Both systems may be inaccurate when hypothermia is associated with trauma because trauma can cause an altered level of consciousness and can inhibit or abolish shivering.
Core temperature cooling rate increases during and after extrication from snow burial due to afterdrop, which is accelerated by increased activity of the avalanche victim, exposure to the air, and removal from the insulation of snow.26,27
Prevention
Prevention of avalanche morbidity and mortality includes 4 components: avoiding being caught in an avalanche, avoiding burial if caught, minimizing trauma if caught, and avoiding asphyxia if buried. The primary target for education is to avoid avalanche accidents. Methods of public safety prevention and mitigation, such as the use of explosives and the employment of barriers such as snow fences, deflectors, and snow sheds across roads, are beyond the scope of this article.
Avalanche Avoidance
Although many avalanches are not reported, elevated avalanche hazard and heightened avalanche activity can be forecasted to some extent. In the majority of avalanche accidents, the victim or someone in the victim’s party triggered the avalanche. 28 Personal avalanche risk can be lowered by avoiding dangerous terrain, snow, and weather conditions. Avoiding avalanche-prone slopes is a complex skill. A detailed discussion of decision-making and safe route selection in avalanche terrain is beyond the scope of these guidelines. Education and experience should be the cornerstone of risk mitigation. Some examples of techniques used to avoid avalanches include avoiding slopes >30 degrees, traveling on ridges, traveling in thick forested terrain, and avoiding travel in avalanche terrain during high-risk conditions when avalanches are likely, such as during and immediately after heavy snowfall and significant wind and during rapidly warming temperatures.29,30
Avalanche education, including avalanche advisories published by local avalanche safety agencies, has been a focus of avalanche accident prevention efforts. Avalanche safety courses, textbooks, and videos provide detailed training for mandatory avalanche safety skills. 29 –31 Decision aids 32 –35 have been developed to facilitate objective and consistent assessment and reduce the influence of misleading human factors. Although the impact of these decision aids are difficult to interpret, especially in the recreational context, analyses generally support their effectiveness.36,37
In addition to education, familiarity and regular practice with safety equipment and exercise of good judgment are vital to avalanche avoidance.
Recommendation
Travelers in avalanche terrain should obtain avalanche education by attending training courses, using educational books and videos, and regularly practicing safe travel and rescue skills. Backcountry users should use avalanche advisories and a decision aid to help with trip planning and route finding in avalanche terrain. Grade: 1C.
Recommendation
Backcountry travelers should exercise conservative judgment and risk-mitigation strategies to avoid triggering and being caught in an avalanche. Ungraded: Expert consensus.
Avoiding Being Caught and Buried
Physical maneuvers
Once an avalanche occurs, a person has limited ability to affect its outcome due to the speed and violence of sliding snow or ice. The person should attempt preventive measures first to avoid being caught once the snow starts sliding.
When entering a potentially high-risk avalanche path for purposes such as mountain rescue or avalanche control work, use of a belay rope that is securely anchored outside the path can prevent an individual from being swept downslope by an accidentally or intentionally triggered avalanche.30,38 Travelers should cross dangerous slopes one at a time, while being watched by a partner, and should move between islands of safety—rock outcroppings, tree clusters, or safer adjacent slopes. Planning an escape route before entering an avalanche-prone area can increase the likelihood of a successful outcome if an avalanche occurs. Avalanche professionals commonly use slope-cutting techniques, in which the backcountry user rapidly traverses a potentially unstable slope from one safe zone to another with the intent of testing stability. This technique may trigger an avalanche in a controlled fashion, possibly eliminating some or all of the avalanche hazard on a slope and providing information about the stability of the slope.30,38 Slope cutting requires extensive experience and is not recommended for recreational backcountry users.
If one is unable to avoid getting caught in an avalanche, the immediate response should be to escape to adjacent terrain that is not involved in the avalanche. When descending suspect slopes, travelers should maintain a speed at which their momentum has a chance to carry them off the moving snow to a preplanned zone of safety. This defensive technique may reduce the odds of being caught and buried but requires expert skill.
The next step, if one is unable to escape the sliding snow, is to avoid burial. A victim, once caught, should attempt to remain on the surface of the sliding snow and fight to move toward the starting zone of the avalanche where the flow is less turbulent. One may be able to arrest a slide by anchoring into the bed surface with a ski pole or ice ax. 39 Grabbing a tree may halt downward movement, but this technique is only practical if performed quickly before the avalanche picks up speed. Some experts recommend swimming motions to stay on the surface of avalanches. Although this practice has been challenged, 39 case studies and theoretical considerations regarding the flow characteristics of avalanches support the importance of victims fighting to stay toward the top of the debris flow. 40
A victim with attached skis, snowboard, or snowshoes will likely be buried deeper than a victim without attached impediments, and extrication will likely be more difficult. Removing equipment, if possible, may improve survival chances. A backpack should be kept on to provide possible protection against trauma. The equipment in the backpack will be useful if the victim is not buried. However, no data support these 2 recommendations.
Recommendation
To avoid being caught in an avalanche, experienced backcountry users can use slope cutting and a belay. Ungraded: Expert consensus.
Recommendation
If caught in an avalanche, one should immediately attempt to escape the moving snow or, if engulfed, fight in any way possible to avoid complete burial. Grade: 1C.
Recommendation
If caught in an avalanche and unable to escape the moving snow, a victim should jettison skis and snowboards. Using a backpack may help mitigate trauma. Ungraded: Expert consensus.
Avalanche airbags
Avalanche airbags are the only avalanche safety devices aimed primarily at preventing burial. 4 Avalanche airbags are backpacks or vests that contain 1 or 2 inflatable balloons. When caught in an avalanche, a user manually deploys the device by pulling an activation handle. This action inflates the stowed balloon(s) to a total volume of about 150 L (Figure 2). To inflate the balloons, avalanche airbags use 1 or 2 cylinders of compressed gas or a battery-powered fan. A deployed airbag increases the effective volume of an avalanche victim, taking advantage of a physical process known as granular convection, which has also been called “inverse segregation.” In a flow of various-sized particles, larger particles are sorted toward the surface. 41 –43 Thus, the increased effective volume reduces the chance of deep or complete burials.
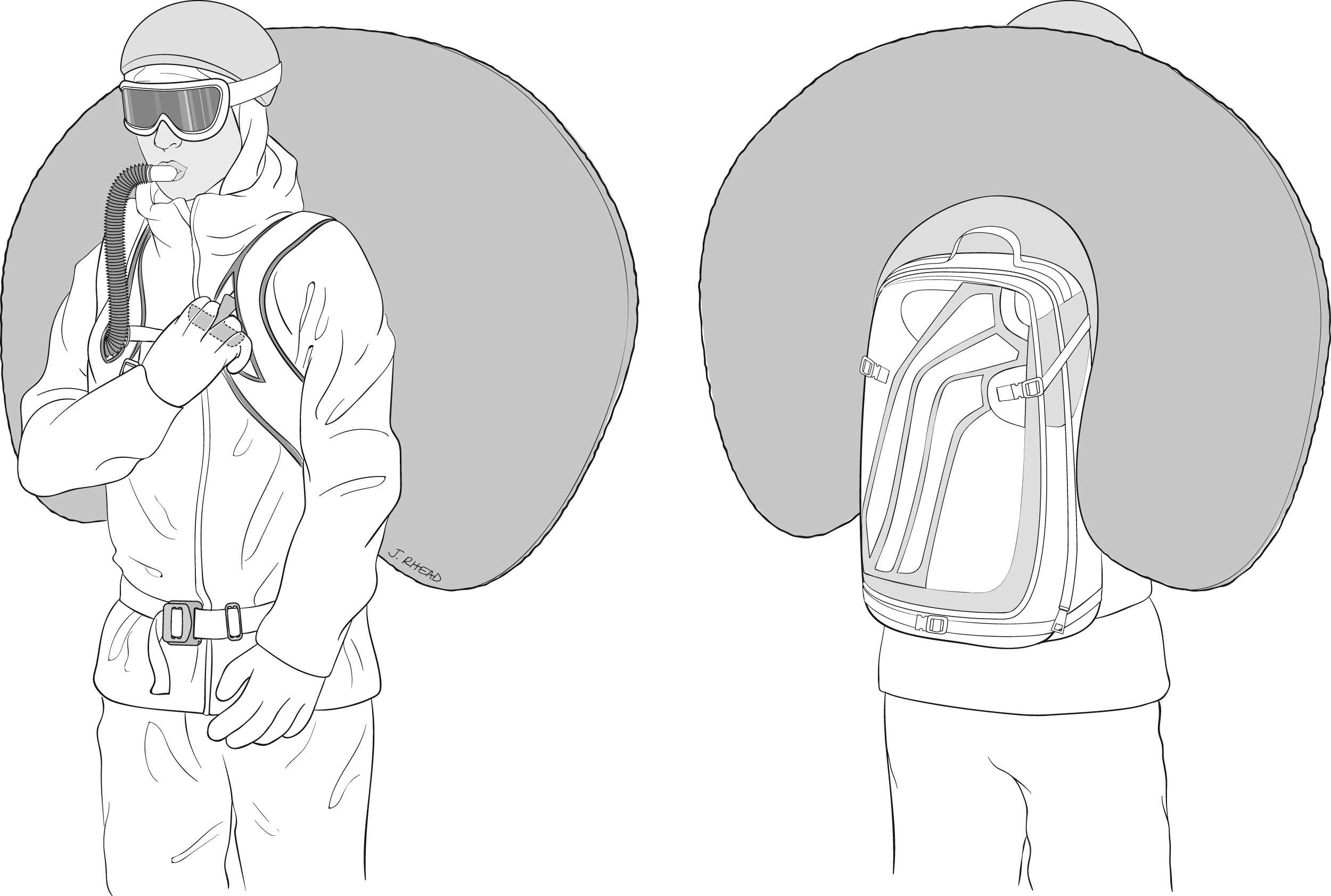
Backpack shown with an airbag deployed and inflated, combined with an artificial air pocket device.
The effectiveness of avalanche airbags is supported in simulations and by epidemiologic studies. Trials using intentionally triggered avalanches and crash test dummies show that dummies with an inflated airbag had a lower probability of being buried. 44 –46 Retrospective statistical evaluations of accident records have compared the mortality rates of avalanche victims with and without airbags. 4 ,47,48 Haegeli et al examined the effectiveness of airbags using avalanche accident records from Europe and North America. 49 In this retrospective analysis, inflated airbags reduced mortality from 22 to 11%, an absolute reduction of 11 percentage points (95% confidence interval: 4–18 percentage points). This study also found that noninflation was a problem with the use of airbags. The observed noninflation rate from all causes across the entire dataset was 20%, reducing overall mortality reduction for airbag users from 11 to 9 percentage points.
With 60% of noninflations attributable to the user failing to trigger the airbag, operator error is the most important limitation of the use of airbags. Other obstacles to use of airbags include cost, weight, and difficulty with regulations limiting most, but not all, compressed gas canisters on commercial airlines. Airbags also lack efficacy if a victim is swept off a cliff or into thick trees, where trauma is a higher risk than asphyxia. Death from asphyxia can also occur with a deployed airbag if the user is buried deeply in a terrain trap or if a second avalanche completely buries the balloon.
Electronic interference between avalanche transceivers and cell phones, medical devices, and radios has also been documented.50,51 No published studies have examined if the electronics of a battery-powered, fan-actuated airbag interfere with the use of transceivers, but it is unlikely because fan airbags do not transmit a signal.
No safety or survival data exist that compare airbags inflated by the 2 different actuation systems. Airbags with fans are advantageous because the user can practice with the device multiple times at little cost, and they are allowed on commercial airplanes. Canister-actuated airbags require additional canisters for practice or for multiple deployments in the field, and most canisters are not allowed on commercial airplanes.
One fan airbag system, after deployed, deflates automatically after 3 minutes. This potentially can create an air pocket. No data confirm creation of an air pocket or potential benefit of an air pocket created by this system.
At least one manufacturer builds a backpack with both an airbag and an artificial air pocket device (AAPD). This type of product is discussed in more detail later.
Recommendation
Travelers entering avalanche terrain should consider using an avalanche airbag. Familiarity and regular practice with airbags is essential. Grade: 1B.
Trauma Prevention
Helmets
Helmets are widely used in ski and snowboard mountaineering and other backcountry pursuits. According to a retrospective review of autopsies of avalanche victims in Utah, traumatic brain injury may contribute to death from asphyxia. 52 Helmets have been shown to prevent minor and major trauma among resort skiers and snowboarders. 53 Some experts have speculated that helmets are less effective at preventing morbidity and mortality in avalanches, while other experts note few downsides exist for using helmets. 54 No studies exist regarding the effectiveness of helmets in reducing death due to head trauma from avalanche accidents. The velocities created by medium and large avalanches may exceed the protective capabilities of helmets designed for recreational skiing and climbing. 54 However, most recreational victims are killed in small- to medium-sized avalanches of lesser velocities, in which helmets could prevent mild to moderate traumatic brain injuries. 28 Helmets can also help prevent lacerations, minor head injuries, and hypothermia.
Recommendation
Helmets should be considered when travelling in avalanche terrain. Grade: 1C.
Avalanche airbags
Some models of avalanche airbags are shaped to surround the head and neck once deployed. Generally, these models are designed as backpacks with single airbags in a “U” shape (Figure 2). This design may help prevent or mitigate injuries sustained from the violence of the avalanche involvement or during collisions with objects in an avalanche. No data are available regarding the use of these devices to reduce the risk of head and neck trauma, but theoretical benefit exists.
Recommendation
Airbag backpacks may or may not provide head and neck protection from trauma. Ungraded: No recommendation.
Asphyxia Avoidance if Buried
Physical maneuvers
An unobstructed airway with an air pocket is critical for surviving avalanche burial, but the violence of an avalanche typically forces snow into the mouth and nose of a victim. One possible technique for protecting the airway during an avalanche is to reach across the face with an arm, then put the crook of the elbow over the mouth. 38 This method not only helps to lessen the amount of inhaled snow from moving debris but could also protect against facial trauma and create a small air pocket after the debris comes to a stop. Because avalanche debris often solidifies before the avalanche comes to a stop, it is important to use this technique prior to the avalanche coming to rest as movement slows.
Recommendation
If caught in an avalanche, a victim should protect the airway and create an air pocket by reaching across the face with an arm, placing the crook of the elbow over the mouth. Grade: 1C.
Artificial air pocket devices
Although the device is termed an AAPD, it does not create an air pocket but instead is intended to enable a completely buried avalanche victim to divert exhaled CO2 away from the airway. An AAPD separates carbon dioxide–rich exhaled air from oxygen-rich inhaled air, delaying asphyxiation by preventing rapid dilution of inhaled air with excess CO2. The device consists of a mouthpiece that connects to tubing containing a 1-way inspiratory valve and a 1-way expiratory valve. Inspired air comes directly from air in the snowpack and expired air is diverted to the back of the user via an exhaust port (Figure 3).

The artificial air pocket device that diverts expired air away from inspired air during avalanche burial is intended to prolong survival of fully buried avalanche victims. The white arrows show the flow of inspired air, and the gray arrows show the flow of expired air.
In addition to delaying asphyxia caused by rebreathing CO2, breathing through the tube reduces the likelihood of forming an ice mask in the intake area. The mouthpiece may help keep the airway free of snow if employed prior to being caught in an avalanche.
In a randomized, crossover controlled trial, breathing with an AAPD sustained adequate oxygenation for up to 60 minutes. 19 During the control burial study, participants who breathed directly into a small, 500-mL air pocket experienced hypoxemia within 5 to 14 minutes. Many cases of survival associated with the use of an AAPD have been reported.55,56 No study comparing the mortality of users and nonusers has been conducted.
At least 1 manufacturer builds a backpack with both an airbag and AAPD (Figure 2). The advantages of integrating these 2 devices are minimization of separate pieces of equipment and decrease of total cost. No evidence exists regarding advantages or disadvantages of using the 2 devices simultaneously. The potential benefit of tandem use could be significant as they complement each other by targeting different aspects of avalanche survival.
Recommendation
Travelers entering avalanche terrain should consider using an artificial air pocket device. Grade: 1C.
Rescue
Avalanche rescue can be accomplished through self-rescue, small-group rescue, or professional rescue. A systematic approach to avalanche rescue maximizes the efficiency and effectiveness of rescuers. 57
Avalanche Rescue Sequence
A rescue sequence (Figure 4) can be adapted to an avalanche rescue regardless of the number of victims or rescue personnel. In a small-team setting, a single individual may be tasked with multiple elements of this approach, while a large-team response may allow for each role to be assigned to a different rescuer. Some steps may be completed simultaneously.
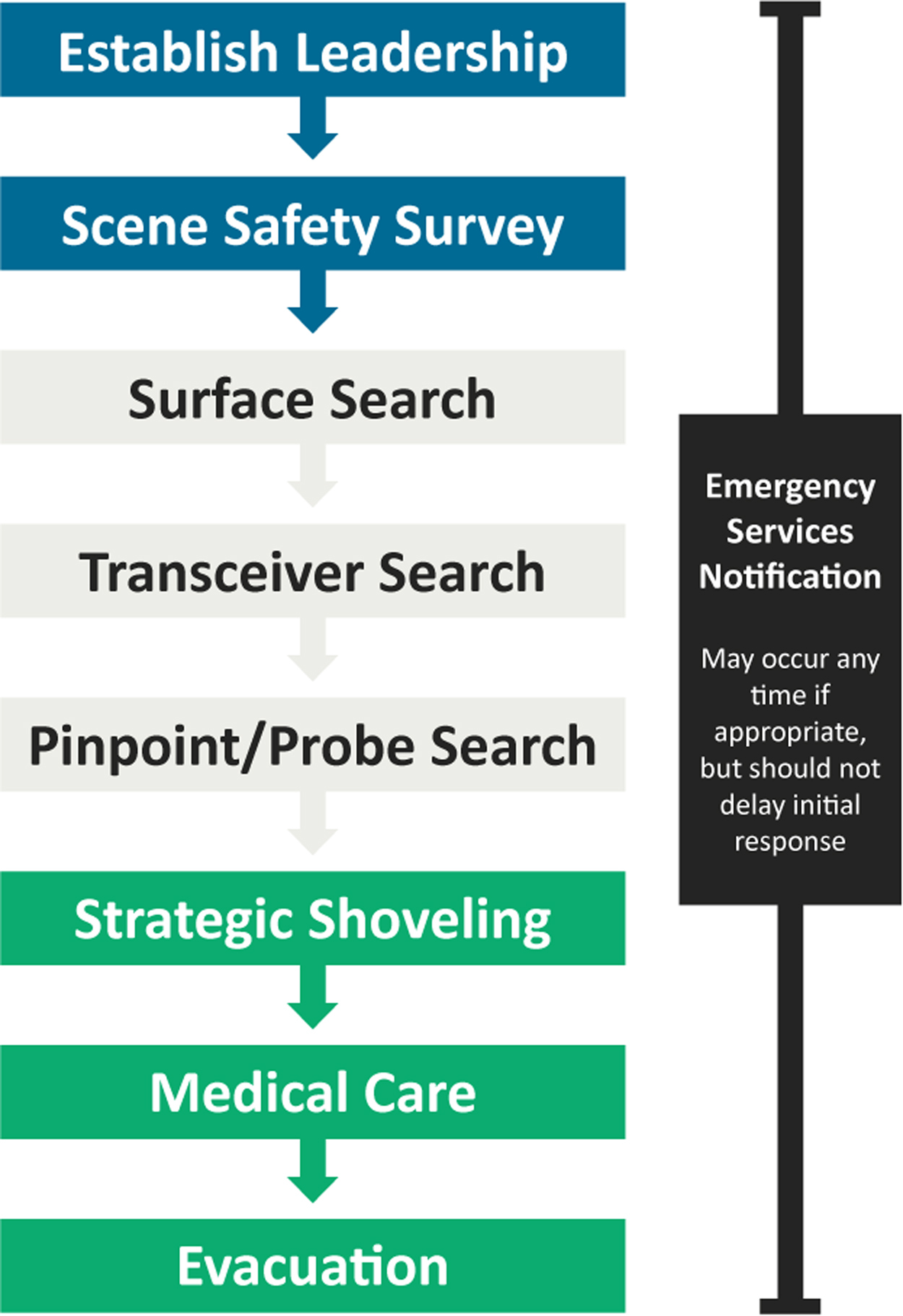
Avalanche rescue sequence.
Leadership should be established immediately. The leader should assess the scene for risks, formulate a rescue plan, manage the available resources, and adapt to changing conditions.
Scene safety should be constantly reassessed throughout a rescue. As circumstances and risks change, immediate corrective actions should follow. Ideally, depending on the number of rescuers, at least 1 person should identify potential hazards and work to formulate plans to mitigate hazards. At least 1 person, if available, should be positioned at a vantage point that allows for visualization of the entire scene while also being physically removed from the hands-on aspects of the rescue.
The surface search then commences. Often, especially with small groups, this begins simultaneously with the transceiver search, described in the following section. This initial search looks for visible clues. If rescuing from above the accident, the surface search should begin at the point at which the victim was last seen. If responding from below, personnel can begin searching at the bottom edge of the debris and progress uphill. The point at which the victim was last seen should be delineated with a physical marker such as a ski pole or avalanche probe.
After the surface search, the next 3 components of locating a buried victim are a transceiver search (both coarse and fine searches), a pinpoint search (also called probe search), and shoveling to extricate the found victim. These components will be discussed further.
Local emergency services should be notified after an avalanche that requires additional rescue or medical assistance. However, notification should not delay the initial rescue response; 58 additional time is required to turn on a phone, acquire a signal, and report an accident. Small groups should be cautious in pausing a rescue to divert personnel to contact emergency services, as this extra time could mean the difference between life and death for the victim.
Recommendation
During an avalanche accident, the rescuers should establish leadership; secure the scene; perform surface, transceiver, and pinpoint (probe) searches; shovel strategically; and notify emergency services when appropriate. Ungraded: Expert consensus.
Transceiver Search
When used by both victims and rescuers, avalanche transceivers decrease morbidity and mortality. Transceivers reduce the time from complete burial to companion rescue: One study found a reduction in burial time from 102 minutes to 20 minutes. However, mortality of completely buried victims was only reduced from about 68% to about 54%. 59
Electronic devices, such as mobile phones, portable radios, global positioning systems (GPS), and other digital communication devices may interfere with avalanche transceiver searches because similar radio frequencies are susceptible to electromagnetic interference. 51 Medical devices such as cardiac pacemakers, implanted defibrillators, and insulin pumps can also interfere with transceivers. 50 It is not yet known whether electronic battery-operated fan airbags interfere with transceivers, but devices, such as fans, that do not transmit a signal are less likely to cause interference than those that do. Current literature suggests that transceivers in transmit mode should be kept at least 20 cm from other electronics and those in receive mode during a search should be kept at least 50 cm from electronic devices. 57 ,60,61
Recommendation
All travelers in avalanche terrain should carry avalanche transceivers, know how to perform effective searches, and practice these skills regularly. Grade: 1B.
Recommendation
Rescuers should keep transceivers a minimum of 20 cm from other electronics and metal objects in transmit mode and a minimum of 50 cm in search mode. Grade: 1B.
Other location devices
Telecommunication devices other than avalanche transceivers have been studied and have not been found useful for avalanche companion rescue. GPS transceivers are ineffective due to imprecision of the signal.62,63 No studies have evaluated personal locator beacons, but these devices rely on GPS technology and are not designed for companion rescue.
Cell phones, satellite phones, and handheld very high frequency/ultrahigh frequency radios have not been studied for use in avalanche rescue but can aid in summoning help. Cell phone avalanche applications have been reviewed and found to be insufficient to find a buried victim in a reasonable amount of time. 64
Recommendation
Electronic devices other than avalanche transceivers are not recommended for locating buried avalanche victims during small-group rescue. Grade: 2C.
Pinpoint search
A probe can be instrumental to pinpoint the location of a buried victim. A 3-m probe length is standard. One study suggested that a 2-m probe was adequate because most avalanche victims who are found are buried 1.5 m or less.65,66 The main advantage of the shorter length is that it saves weight and space in a backpack.
After a rescuer has used an avalanche transceiver to find the location at which the signal of the buried beacon is closest to the snow surface, probing should be completed in a systematic fashion. The probe should be inserted perpendicular to the snow. A concentric circular method should be used for efficiency, beginning at the closest transceiver reading location. The spacing between each of the probe holes should be 25 cm.67,68 Rescuers should feel for inconsistencies within the snowpack and monitor changes in the depth at which the probe stops, which might indicate a victim strike. Whenever a possible strike occurs, the probe should be left in place as a target for shoveling. If necessary, additional probes should be used to confirm the strike or to attempt to determine the orientation of the buried victim.
Recommendation
All travelers in avalanche terrain should carry and know how to use a 3-m collapsible probe for the pinpoint search. The technique should include probing in a perpendicular fashion using a concentric circular pattern with probe holes spaced 25 cm apart. Grade:1C.
Strategic shoveling
Shovels are essential to extricate a buried victim. A metal shovel blade is more durable than a composite blade. 69 Efficient shoveling techniques are essential to minimize extrication time and increase survival. 66 Shoveling should begin downhill from the probe strike at a minimum distance of 1.5 times the burial depth, as indicated by the probe. A body-width working area, level with the buried victim, should be created as a working platform to help conserve the rescuer’s energy. The shovel can be used like a paddle to scrape or plow snow downhill. Initially, snow should be moved to the sides of the pit, leaving the middle for snow from deeper in the pit.
When multiple rescuers are available to shovel, a conveyor belt method may be used.70,71 In this method, rescuers rapidly paddle snow downhill in succession, usually fanning the snow to the sides to eliminate buildup of excess snow. Rescuers should rotate positions frequently, typically every few minutes, to prevent fatigue. The goal is to excavate a wide, flat platform to place the extricated victim and aid in resuscitation and packaging for transport.
Recommendation
All travelers in avalanche terrain should carry and know how to use a metal shovel designed for avalanche debris. Shoveling techniques should include using the shovel like a paddle to plow snow downhill. A conveyor belt should be used if multiple rescuers are available. Ungraded: Expert opinion.
Professional Rescue
Organized rescue groups may include mountain guides, volunteers, or professionals such as ski patrollers. Professional rescue differs from companion rescue because the response time is typically longer, resources are more plentiful, and group size is larger. Because an organized group takes longer to mobilize than the typical 30 minutes during which a victim will asphyxiate, the incidence of live recovery from an organized rescue response is low. 1
Incident Command System
The Incident Command System (ICS) or a similar system should be used to establish a standardized approach to command and control in an emergency avalanche response. This concept has been successfully applied to avalanche rescue. 72 –74
Recommendation
All members of organized rescue groups should receive training in ICS, or local equivalent, and its practical application in avalanche rescue. Grade: 1C.
Avalanche scene management
Avalanche scene management becomes increasingly important as more rescuers and resources become involved in an avalanche response. Effective scene management can reduce false positive signals from well-intentioned bystanders wearing transceivers and can help ensure effective search of an avalanche path while minimizing missed areas or clues. Avalanche path boundaries should be marked to keep unauthorized people from introducing erroneous clues and to help ensure that rescuers have a clear view of the avalanche site. The entry and/or exit tracks, the last-seen point, visible clues, and probe locations should be marked with physical markers such as climbing wands, ice axes, skis, ski poles, or backpacks. 75
Recommendation
Active scene management techniques such as boundary control and scene marking should be employed. Ungraded: Expert opinion.
Probe line
After completion of an initial search using a transceiver or in situations with buried victims without transceivers, a probe line should be initiated. Professional rescue teams must maximize probe line efficiency to increase the likelihood of recovering a live victim. A leader will ensure accuracy and efficiency of the probe line.
The first probing depth should be restricted to 1.5 m to maximize efficiency. Probing restricted to a depth of 1.5 m would reach the depth of 88% of victims who were recovered alive in the United States and 95% of those recovered alive in Switzerland. 65
The probe technique should follow the Three Holes per Step method, which has been shown to be 30% faster than standard coarse probing. 65 This method involves a rescuer inserting the probe into the snow 3 times: 20 cm to the rescuer’s left, center, and right while standing. The rescuer then takes a step forward and repeats the process.
Slalom probing is another organized probe technique. In this method, organized rescuers probe 3 areas in a left-to-right pattern 50 cm apart while walking in a zig-zag fashion through a strip of avalanche debris. 76 The advantage of this pattern is that it can take less time to cover the same surface area compared with the Three Holes per Step method, but it may be less effective.
Probe line grid spacing will influence the overall probability of detection. A small grid will give a greater chance of finding a buried victim but may cause the probe line to move slowly. A large grid may cause rescuers to miss a buried victim. A 50 × 50 cm grid may offer the best probability of detection without prolonging search time. 77
Recommendation
For probe lines, initial probe pass should be limited to a depth of 1.5 m using Three Holes per Step or Slalom Probing methods to cover a 50 × 50 cm grid. Grade: 1C.
RECCO
The RECCO search system uses harmonic radar to detect an avalanche victim. The searcher uses a RECCO detector to identify a RECCO reflector diode embedded into the victim’s clothing. The reflector diodes are small, light, and do not require a power source. Many manufacturers have incorporated these reflectors into clothing such as snow pants, jackets, and helmets.
The RECCO detector, however, is larger than traditional transceivers and requires frequent practice for rescuers to remain proficient. For these reasons, it is only intended for professional rescue. Other disadvantages of the RECCO system include a short detection range due to attenuation of the signal, especially in dense, wet snow and the potential for false positive signals from searchers or other reflective matter.78,79
Recommendation
Professional rescue teams should have RECCO search capabilities and an established search protocol. Grade: 1C.
Dog search
Avalanche rescue dogs are trained to detect buried victims by scent. One study found that survival of victims found by dogs was no better than that of victims found by organized probe line searches. 80 Additional limitations of dog searching include the time needed to transport a team to the site and canine distraction caused by contamination of the debris field by bystanders. Training avalanche rescue dogs also requires a significant time and resource commitment.
Recommendation
Professional rescue teams should consider using dogs trained in avalanche rescue to facilitate searching debris for a buried person, despite the disadvantages described, particularly if the victim is not wearing a transceiver and the initial sequence has failed. Ungraded: Expert consensus.
Helicopters
Helicopters can decrease response time to remote locations, decrease risk by moving rescuers over potentially hazardous terrain to reach avalanche sites, and evacuate patients quickly. Helicopters can be used to search from the air with transceiver and RECCO technology.78,81 Helicopter Emergency Medical Services are separate but complementary resources to search and rescue helicopters. Some specially trained Helicopter Emergency Medical Services programs can perform avalanche search as well as provide medical transport. 82
Helicopters are high-value resources that also have potential risks. Conditions such as time of day, weather, and pilot proficiency in mountain environments can significantly affect the performance of helicopter use in search and rescue as well as the risk to the rescue crews.
Recommendation
Professional rescue teams should consider using helicopter teams that are specifically trained in avalanche rescue, if available. Rescuers should employ a risk assessment before helicopter use and follow strict safety guidelines Ungraded: Expert consensus.
Resuscitation
Resuscitation at the scene of an avalanche can be challenging. A rescuer may have to start cardiopulmonary resuscitation (CPR) and advanced life support (ALS) in a confined space in an austere environment with limited equipment and personnel. Resuscitation can start when the head and chest are exposed, before complete extrication of the body. Early in the resuscitation, information about patency of the airway, presence of an air pocket, and vital signs upon extrication are important to guide treatment and transport decisions. 11
Prognostic factors for survival after avalanche burial are the severity of injury (if present), duration of complete burial, airway patency, core temperature, and initial serum potassium (if available in the field). 22
Guidelines for the on-site triage of avalanche victims in cardiac arrest and for transport decisions were updated and published by the European Resuscitation Council (ERC) in 2015. 11 Recent retrospective observational studies have found survival rates of avalanche victims who received prolonged CPR and extracorporeal life support (ECLS) to be as low as 11%. 83 –85 Many asphyxiated victims without a chance of survival have been transported to ECLS facilities. Completely buried avalanche victims will succumb to hypoxia in <10 minutes and likely die soon thereafter if the airway is totally obstructed. The cooling rate of a completely buried avalanche victim while buried ranges from 0.6°C·h−1 to 9°C·h−1. 16 ,20,86,87 Moderate to severe hypothermia may become important only after 60 minutes of burial, and only if the airway is patent. In addition, there have been no successful ECLS rewarming resuscitations of avalanche victims in cardiac arrest who were recovered with a core temperature >30°C because they most likely experienced cardiac arrest from asphyxia. Importantly, due to the insulating properties of snow, increased activity, and exposure to the ambient environment, afterdrop can accelerate core cooling once the buried victim is uncovered. Based on these data, the criteria for prolonged CPR and ECLS have been made more stringent in the 2015 ERC guidelines than in the previous 2010 edition.
The algorithm for resuscitation is outlined in Figure 5. Each component will be fully discussed. The new guidelines set cutoffs for hypothermic resuscitation at >60 minutes’ duration of burial and core temperature of <30°C in order to reduce the number of futile resuscitation attempts and to forestall ECLS efforts that are unlikely to lead to neurologically intact hospital discharges.
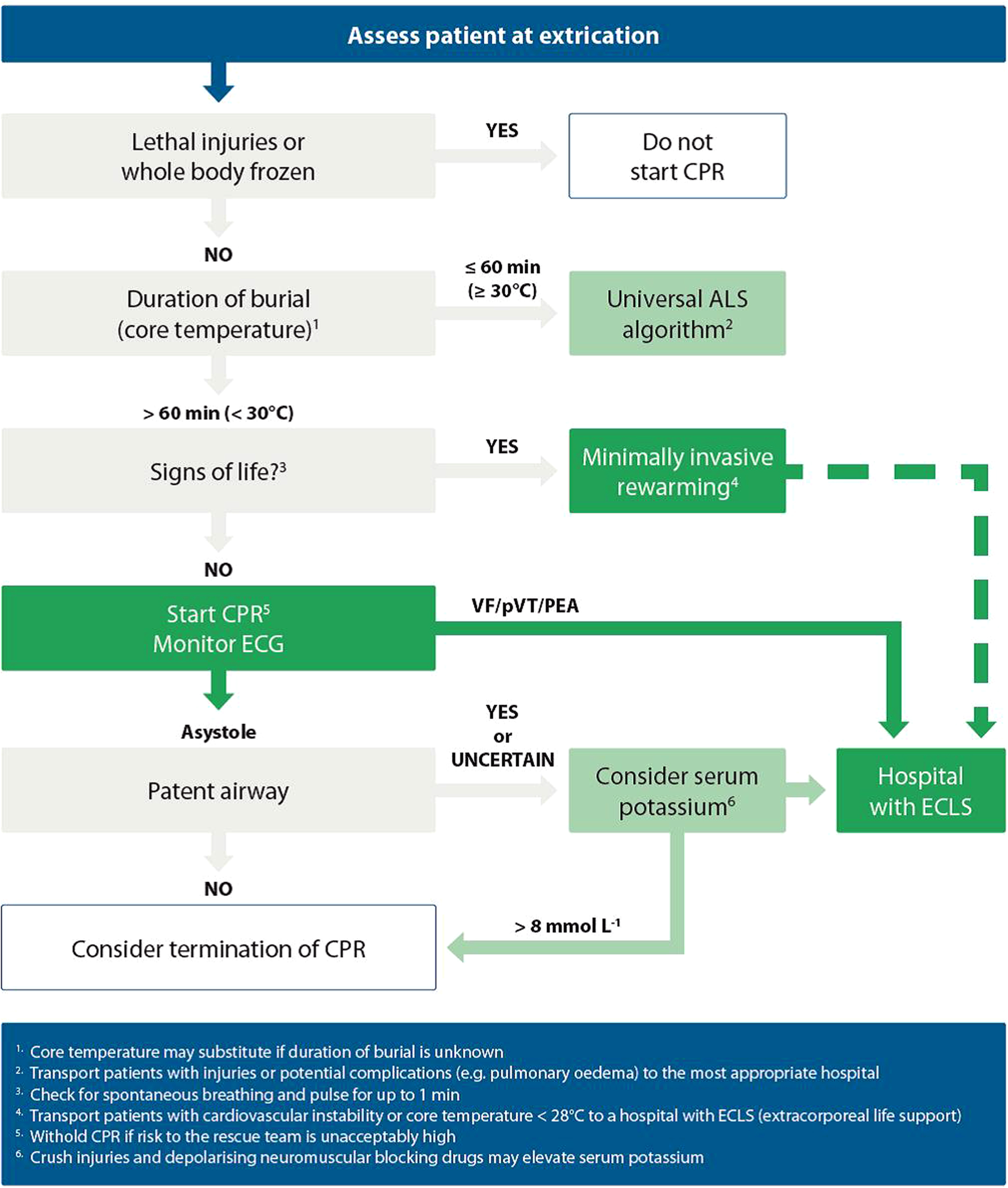
Avalanche accident algorithm for management of completely buried victims. ECLS, extracorporeal life support. 11
Uninjured Full Burial
If a patient is alert and responsive after full burial, cold stress or mild hypothermia is still a possibility, especially with burials exceeding 30 minutes. Rewarming can occur through shivering thermogenesis. Completely buried avalanche victims rarely develop pulmonary edema several hours after extrication. The etiology seems to be a combination of negative pressure–induced pulmonary edema and hypoxia-induced left heart failure.88,89
Recommendation
A completely buried patient, even if uninjured, should be transported to the nearest medical facility capable of evaluating and stabilizing the patient. Grade: 2C.
Management of Trauma
Trauma can exacerbate hypothermia and asphyxia. Patients with injuries such as head trauma, suspected spinal injuries, and long bone fractures can be treated in accordance with generally accepted practice. Suspected cervical spine injuries can be managed using validated guidelines such as NEXUS 90 or the Canadian C-Spine Rules. 91 The WMS Practice Guidelines for Spine Immobilization in the Austere Environment present further recommendations for evaluating and managing spine injuries in the wilderness, but these guidelines have not been validated. 92
Recommendation
Avalanche resuscitation should include trauma care. Suspected spine injuries should be managed according to the specific recommendations of validated guidelines such as NEXUS or Canadian C-Spine Rules. Ungraded: Expert consensus.
Management of Hypothermia
Moderate or severe hypothermia should be suspected in a cold and unconscious avalanche victim. The WMS Practice Guidelines for Out-of-Hospital Evaluation and Treatment for Accidental Hypothermia 23 and the ERC guidelines 11 present recommendations for the treatment of hypothermia.
Recommendation
Avalanche resuscitation should include treatment of hypothermia according to the WMS Practice Guidelines for Out-of-Hospital Evaluation and Treatment for Accidental Hypothermia or the European Resuscitation Council guidelines. Ungraded: Expert consensus.
Initiating Resuscitation
All victims who are extricated should be assessed for airway, breathing, and circulation according to local protocols. Unless an indication for withholding resuscitation exists, as outlined below, CPR should commence and ALS should be performed if the rescuer is trained.
If duration of burial is ≤60 minutes and core temperature is ≥30°C, cardiac arrest is likely due to trauma or asphyxia. Cardiac arrest is unlikely to be due to hypothermia, so ECLS rewarming is not indicated. If standard CPR or ALS does not lead to return of spontaneous circulation (ROSC) within 30 minutes, chance of survival is minimal and further attempts at resuscitation are not necessary. 93 –95
If duration of burial is >60 minutes, the core temperature is <30°C, and the victim had a patent airway at extrication, cardiac arrest may be attributed to hypothermia, and an attempt at extracorporeal rewarming is indicated. Survival of avalanche victims who present with unwitnessed cardiac arrest at extrication is lower when compared with avalanche victims with witnessed cardiac arrest after extrication. 83 Prolonged CPR and ALS may be indicated beyond 30 minutes, especially with arrest due to suspected hypothermia and/or witnessed cardiac arrest after extrication. If core temperature is <30°C, defibrillation of a shockable rhythm may be unsuccessful, but prolonged CPR, for hours if necessary, until the patient is rewarmed to 30°C may be successful. 11
Recommendation
If vital signs are not detectable and there are no indications for withholding resuscitation, rescuers should start CPR and ALS while further assessment is performed. Grade: 1B.
Recommendation
If ROSC is not achieved after at least 30 minutes, resuscitation attempts may be stopped (with certain exceptions below). Grade: 1B.
Recommendation
If duration of burial is >60 minutes, the core temperature is <30°C, and the victim had a patent airway, arrest may be due to hypothermia; CPR should be continued and the patient transported to a hospital with ECLS capability. Grade: 2B.
Defibrillation
If a defibrillator is available, rescuers should place pads and analyze the rhythm. The core temperature at which defibrillation should be initiated and the power and number of shocks in the severely hypothermic (<30°C) arrested patient have not been established. Animal data and case reports indicate that >30°C (and even >28°C), defibrillation may be successful, but experimental and clinical experience suggests that with higher core temperature (≥30°C) ROSC after defibrillation is more stable and rarely degenerates back to ventricular fibrillation (VF). Delaying continued defibrillation attempts until core temperature is ≥30°C may be reasonable because every shock may cause further myocardial injury. CPR and rewarming may have to be continued for several hours to facilitate successful defibrillation. 96
Several regional guidelines exist based on local protocols. The WMS Hypothermia Guidelines recommend 1 defibrillation in an arrested person <30°C. 23 The American Heart Association recommends defibrillation attempts for hypothermic cardiac arrest similar to normothermic cardiac arrest, every 2 minutes. 97 The ERC guidelines recommend up to 3 defibrillation attempts with a core temperature <30°C and, if VF persists after 3 shocks, delaying further attempts until core temperature is ≥30°C. 11
Recommendation
If a defibrillator is available and a shockable rhythm is detected, defibrillation attempts, according to standard local protocols, should be performed. If VF persists after 1 to 3 defibrillations, provide or withhold further defibrillation attempts according to local protocols. If defibrillation is not successful, CPR should continue beyond 30 minutes until the patient is rewarmed to a core temperature ≥30°C. Grade: 1B.
Advanced life support
An unconscious avalanche burial victim may benefit from endotracheal intubation for airway control and assisted ventilation. Hypocapnia from overventilation (end-tidal CO2 <25 mm Hg) decreases cerebral blood flow due to vasoconstriction and is likely to be detrimental, especially to a patient with traumatic brain injury or hypothermia. Ventilation targeted to normocapnia (end-tidal CO2 35–45 mm Hg) is recommended. 20 ,27,98 If intravenous fluids are available, volume resuscitation via intravenous or intraosseous access with warmed isotonic fluids can help support circulation.
Recommendation
If duration of burial is ≤60 minutes or core temperature is ≥30°C, standard resuscitation and ALS, if possible, should be performed, including volume resuscitation and endotracheal intubation with normocapnic ventilation if indicated. Grade: 1B.
Mechanical chest compressions
Mechanical chest compression has been shown to be of higher quality than manual CPR in technically difficult settings and/or prolonged transport conditions. 99 However, 1 study found no improvement with mechanical chest compressions compared to manual compressions. 100
Recommendation
If available, mechanical chest compression should be used for difficult and long transports. Grade: 1C.
Delayed and intermittent resuscitation
If continuous CPR is not possible for safety reasons, because of a limited number of rescuers, or because of the difficulty of performing CPR during extrication and transport, CPR can be delayed or intermittent. 101 Successful use of delayed and intermittent CPR has been documented. 86 ,102,103 Gordon et al proposed 2 different regimens for a severely hypothermic patient in cardiac arrest, depending on core temperature: A patient with severe hypothermia and unknown core temperature or core temperature known to be 20–28°C should receive at least 5 minutes of CPR alternated with periods of ≤5 minutes without CPR. In a patient with a measured core temperature <20°C, pauses in CPR could be extended to ≤10 minutes. 101
Recommendation
If continuous CPR is not possible in a patient with a core temperature <28°C or with unknown core temperature but unequivocal hypothermic cardiac arrest, intermittent CPR can be performed with ≥5 minutes of CPR alternated with ≤5-minute interruptions. If core temperature is <20°C, interruptions can be ≤10 minutes. Grade: 2C.
Withholding or Terminating Resusciation
Trauma
The chance of survival after traumatic cardiac arrest in an avalanche is extremely low. 104 –106 No survivor with traumatic cardiac arrest from an avalanche has been reported.
Recommendation
If a completely buried victim is in cardiac arrest that has clearly been caused by trauma, rescuers should withhold resuscitation. Grade: 2B.
Duration of burial, core temperature, and airway
Completely buried victims will likely die from asphyxia within 60 minutes of burial if the airway is blocked or if the air pocket is insufficient for breathing. 7 ,8,19 Standard ALS can be successful in an asphyxiated victim and can lead to ROSC but poses the risk of permanent neurological damage. Avalanche victims who are found pulseless and apneic or in asystole with core temperature ≥30°C upon extrication have most likely died from asphyxia. 83
An avalanche victim with core temperature <30°C and a patent airway at extrication who has ventricular fibrillation, pulseless electrical activity, pulseless ventricular tachycardia, or a perfusing rhythm who experienced a witnessed cardiac arrest has a good chance of survival. 83 ,86,107,108
Recommendation
If an avalanche victim is found pulseless and apneic regardless of cardiac rhythm and duration of burial is ≤60 minutes or core temperature is ≥30°C, rescuers can withhold or terminate resuscitation if ROSC does not occur after at least 30 minutes, depending on local regulations or statutes. Grade: 1B.
Recommendation
If a victim is found pulseless and apneic with an obstructed airway and duration of burial is >60 minutes or core temperature is <30°C, rescuers should withhold or terminate resuscitation. Grade: 1B.
Serum potassium
The highest recorded potassium in an avalanche victim who was successfully resuscitated is 6.4 mmol·L−1. 16 One avalanche victim with serum potassium 8.0 mmol·L−1 had ROSC but did not survive. 109 In an avalanche victim with unwitnessed cardiac arrest and other factors as previously described that would lead to a termination of resuscitation, it may be reasonable to undertake transport to the nearest medical facility to determine serum potassium and assess for eligibility for invasive rewarming techniques.
Recommendation
In an avalanche victim who has a serum potassium of >8 mmol·L−1, rescuers can withhold resuscitation. Grade: 1B,
Risk to the rescuers
After an avalanche occurs, ongoing hazards may include additional avalanches, dangerous weather, and rescuer illness such as exhaustion, hypothermia, or frostbite. Rescuers should exercise caution when approaching an avalanche accident to avoid putting themselves in danger. The first priority of rescuers, whether small group or professional, is their own safety. Safety of other rescue team members is the second priority. Only after these are assured should rescuers access and treat any victims. 108
Recommendations
If rescuers are at high risk from terrain or weather, further rescue attempts should be delayed until conditions improve or risks can be mitigated. Ungraded: Expert consensus.
Transfer to Definitive Care
ECLS, when available, should be used to resuscitate severely hypothermic patients who are in cardiac arrest. 110 –112 Transport to a facility with ECLS may be helpful for hypothermic patients (<30°C) with cardiac instability (eg, systolic blood pressure <90 mm Hg, ventricular arrhythmias). 113 Patients with trauma should be transferred to a trauma center.
Recommendation
A hypothermic avalanche victim with cardiac arrest or instability should be transferred as rapidly as possible to a facility with ECLS capabilities appropriate to manage the victim in areas where such centers exist. Grade: 1A.
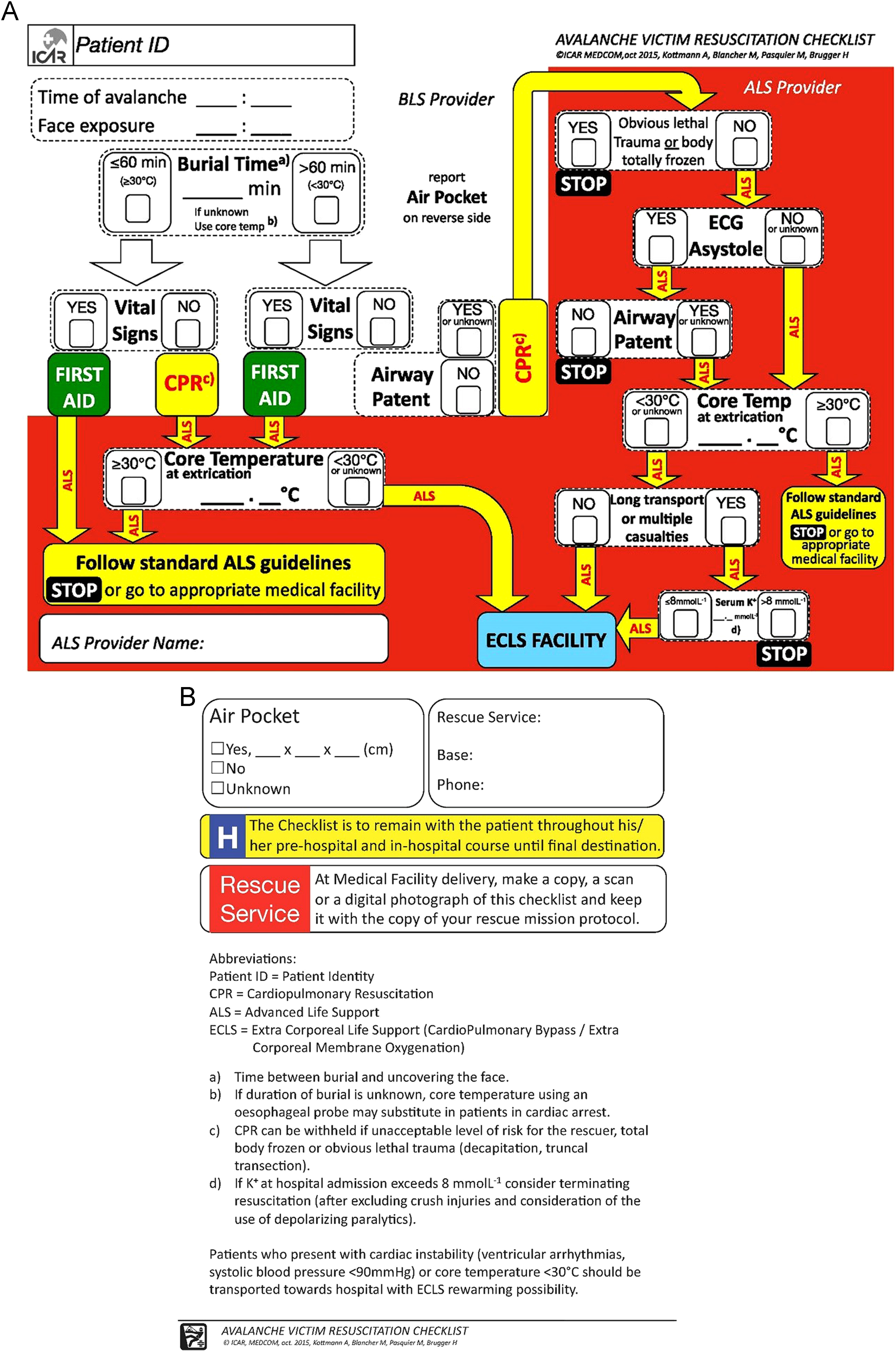
Avalanche Resuscitation Checklist
Adherence to avalanche resuscitation guidelines has not been optimal. 114 Use of an avalanche resuscitation checklist shown in Figures 6A and B is intended to improve adherence to current guidelines and to help collect medical data for further refinement of guidelines and treatment. 115 The checklist is designed to be completed at the site of the accident and to remain with the patient until hospital admission.
Recommendation
An avalanche resuscitation algorithm should be used whenever possible. A checklist may be employed to improve adherence to the resuscitation algorithm. Grade: 1C.
Nonavalanche snow burial
Nonavalanche snow burial (NASB), also called “nonavalanche-related snow immersion,” differs from avalanche burial. NASB has been reported to affect skiers, snowboarders, snowshoers, and snowmobilers who fall head first into tree wells or deep powder snow. Victims who are unable to extricate themselves may die from asphyxia after snow compacts around the head.
Only 1 review article and 1 small burial simulation study exist in the published literature.116,117 Self-extrication is difficult. Buried subjects who remove their skis sink deeper. Position seems to affect the chance of successful self-extrication; being flexed at the waist was common among those were able to extricate themselves. A few case reports suggest that asphyxiation can occur rapidly, but no evidence exists regarding how rapidly death occurs or the exact mechanism of asphyxia. 118 –122
The best way to prevent NASB is to recognize and avoid tree wells and avoid burial in soft snow by staying within skill limits. Other possibly effective preventive measures include maintaining vocal and visual contact with a partner, yelling to alert a partner to a fall, and grabbing tree branches while falling in an attempt to stay upright. No evidence exists to confirm the effectiveness of these preventive measures.
One study suggested that buried victims could use a gentle rocking motion to try to pack snow to get purchase for an attempt to self-extricate. 116 A simulated burial study found that struggling caused subjects to sink deeper; in 1 study, when a subject was upside down, the parka acted as a funnel to collect more snow, which was accentuated when skis or snowboards were removed. 116 It is unclear from limited studies what, if any, strategies can successfully achieve self-extrication.
Whether skis and snowboards should remain attached or be jettisoned is unclear. In 2 cases, victims were spotted via skis and snowboards that were still attached. 118 –120,122
No data exist on use of an avalanche transceiver, radio, or mobile phone in NASB. One deceased victim was recovered using an avalanche beacon and 1 patient was found alive using a voice-activated 2-way radio. 122 It is unknown if avalanche safety equipment, such as transceivers, airbags, or AAPDs, is useful for nonavalanche burial.
No data exist on the utility of avalanche airbags or artificial air pocket devices to prevent nonavalanche snow burial. One manufacturer has speculated that an air pocket may be created by deploying an airbag.121,122
Recommendation
Avoiding falling into tree wells and deep powder snow are the only known means of preventing NASB. A victim of NASB should keep skis or snowboard attached to avoid sinking deeper and to provide visual clues to rescuers. Grade: 2C.
Recommendation
Evidence is insuffient to recommend use of transceivers, avalanche airbags, or AAPDs to prevent NASB. Ungraded: No recommendation.
Discussion
The guidelines presented in this article are general evidence-based recommendations for prevention, rescue, and resuscitation for avalanche accidents.
The foundation of avalanche safety is avoidance of high-risk avalanche-prone areas. This should be emphasized for both professional personnel and recreational enthusiasts. Avalanche safety should be learned through education about avalanche phenomena, proper route finding, and traveling in appropriate snow and weather conditions; knowledge of local avalanche forecasts; routine practice with equipment; and employment of good judgment. Good judgment is the single most important factor in avalanche safety.
As with all wilderness medicine conditions, data are limited regarding avalanche safety techniques and management of avalanche injuries. It is difficult to conduct randomized, controlled trials, and it is challenging to simulate avalanche accidents. Future research should be directed at evaluating the efficacy of helmets, the effects of avalanche airbag balloon configurations in trauma prevention, the causes of airbag nondeployment, the use of AAPDs in combination with airbags, and the use of new transceiver technology. Advances in ALS, ECLS, canine search, and aeromedical evacuation may lead to improved methods for managing avalanche victims.
Author Contributions: All authors contributed to acquisition of data, analysis of data, drafting the manuscript, critical revision of the manuscript, and approval of final manuscript. Funding for illustration was acquired by CVT and CG.
Financial/Material Support: Wilderness Medical Society provided funding for illustrations.
Disclosures: None.
Footnotes
Supplementary Materials
Supplementary material associated with this article can be found in the online version at
Submitted for publication June 2016.
Accepted for publication October 2016.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.