
Abstract
Objectives
Avalanche victims are subjected to a number of physiological stressors during burial. We simulated avalanche burial to monitor physiological data and determine whether wearing head and face insulation slows cooling rate during snow burial. In addition, we sought to compare 3 different types of temperature measurement methods.
Methods
Nine subjects underwent 2 burials each, 1 with head and face insulation and 1 without. Burials consisted of a 60-minute burial phase followed by a 60-minute rewarming phase. Temperature was measured via 3 methods: esophageal probe, ingestible capsule, and rectal probe.
Results
Cooling and rewarming rates were not statistically different between the 2 testing conditions when measured by the 3 measurement methods. All temperature measurement methods correlated significantly.
Conclusions
Head and face insulation did not protect the simulated avalanche victim from faster cooling or rewarming. Because the 3 temperature measurement methods correlated, the ingestible capsule may provide an advantageous noninvasive method for snow burial and future hypothermia studies if interruptions in data transmission can be minimized.
Keywords
Introduction
Avalanche burial can be a significant hazard for the backcountry traveler. Those who are buried face a high risk of mortality and morbidity. Most avalanche deaths result from asphyxiation, approximately 25% from trauma, and a minority from hypothermia. 1 –6 In the avalanche victim, asphyxia begins immediately as rebreathing expired air in the enclosed space results in progressive hypoxia and hypercapnia if the victim is not unburied within 15 to 20 minutes. Cooling from the surrounding snow begins immediately as well. In snow burial, the body loses heat primarily via radiation and conduction. Hypothermia may be accelerated via heat loss from the head and face, as these body areas are extremely vascular areas. Core temperature drops approximately 1° to 3°C/h during snow burial.2,7 The fastest documented drop in core body temperature is 9°C/h, described in a backcountry skier. 8
An avalanche burial victim with an air pocket in front of his or her oral cavity may survive longer before death occurs from asphyxiation and may experience hypothermia. In addition, an emergency-breathing device that diverts expired air away from inspired air during avalanche burial—the AvaLung (Black Diamond Equipment, Salt Lake City, UT)—may delay asphyxiation during prolonged snow burial, increasing the potential to develop hypothermia. 9 Hypothermia is a common medical problem requiring treatment in avalanche victims who are extricated alive and especially those with extended burial times. The degree of cooling will be minimal in those extricated early, but becomes more significant as time elapses, if the victim has an air pocket, or is wearing an AvaLung.
Helmets have been advocated for use during backcountry recreation to prevent head injury. 10 Although asphyxiation is usually the cause of death in an avalanche, many victims sustain head trauma that is thought to be the main cause of trauma-related fatalities. 6 Helmets may have the additional benefit of slowing the progression of hypothermia by providing insulation to the head. Although only limited data exist, more skiers and snowboarders are thought to be wearing helmets in resorts 11 and in the backcountry.
We evaluated the rate of temperature change (via 3 different methods) during snow burial simulating avalanche conditions and rewarming in participants wearing full head and face insulation and without. Our primary hypothesis was that core body temperature would drop slower when wearing the head and face insulation. Our secondary hypothesis was that the 3 temperature measurement methods would correlate. By conducting this study, we aimed to further describe physiology and heat exchange during avalanche burial and propose strategies for preventing heat loss and therefore improving hypothermia care during these events.
Methods
Based on a previous publication 7 by members of our group, 0.7°C/h represents a significant difference in mean cooling rate. The SD of core temperature in this prior study was 0.5°C. Eleven subjects would be needed for 80% power to detect a difference in cooling rate of 0.7°C/h. The recruiting goal of 11 participants was ultimately not achieved, and therefore 9 participants were recruited and gave written consent according to the approved University of Utah Institutional Review Board protocol. Volunteers were healthy adults, nonpregnant nonsmokers with no cardiac, pulmonary, renal, gastrointestinal, endocrine, or infectious disease history. Height and weight were measured, and body mass index (BMI) was calculated.
Burials were performed at 2600 m elevation at Alta Ski Resort in the Wasatch Mountains, Utah. Ambient and snow temperatures were recorded along with measurements of the snow density. Snow density was determined in multiple sites using a 1000-mL wedge density cutter (Snowmetrics, Ft. Collins, CO) that measured the weight of snow per cubic meter, reported as a percent (ie, 300 kg/m3 is 30% density snow, or 70% air). Snow temperature was measured with a dual thermocouple thermometer (Model 600-1040, Barnant Company, Barrington, IL).
Study burial protocols paralleled those used by Grissom et al.7,9 The experimental setup consisted of creating a large mound of snow, approximately 8 by 8 by 8 feet, compacted with body weight and allowed to age-harden for 1 hour. A shoulder-width trench was dug into 1 end of the snow mound and a sitting platform created for the subject so that the head would be approximately 50 cm under the top surface of the mound after burial. Subjects were then quickly buried by shoveling snow into the trench while study personnel packed the snow around the subject and AvaLung pack. A new site was constructed each day.
Each participant underwent 2 burials on 2 different days, 1 with face and head insulation (FHI, intervention) and 1 with no face and head insulation (NFHI, control). Each was randomly assigned to receive 1 experimental condition first, such that half of the participants started with intervention and half started with control conditions. During each burial, participants wore medium-weight synthetic material underwear (Capilene 1 or equivalent, Patagonia, Ventura, CA), warm boots and mittens, and a one-piece Gore-Tex suit (Patagonia). For the FHI burial, the participant wore an insulated helmet, ski goggles, and balaclava. In the NFHI burial, each volunteer wore the above-mentioned gear without the insulated helmet and facemask; only swim goggles and Gore-Tex hood covered the head.
Patients breathed with a device that diverts expired from inspired air during snow burial (AvaPack, Black Diamond Ltd, Salt Lake City, UT). This allowed for oxygen to be inhaled from the snow pack via mesh-protected respiratory tubing. A 1-way valve expelled exhaled air behind the back of the participant. A diagram of this setup is shown in Figure 1.

a. AvaPack (Black Diamond Equipment, Salt Lake City, UT) mechanism of operation. Open arrows show flow of inspiratory air, and shaded arrows show flow of expiratory air. b. Experimental lines used during study. The subject breathes in and out through the mouthpiece (A). An emergency oxygen backup line (B) is attached directly into the mouthpiece apparatus and is used only if the subject becomes hypoxemic or requests to end the study. Monitoring lines (C and D) are connected to a capnometer and record inspiratory P
Time zero began once the head was buried. Body temperature was measured by 3 methods placed or swallowed before burial: 1) rectal probe (Tre) inserted to 15 cm (model 401, YSI Incorporated, Yellow Springs, OH), 2) esophageal probe (Tes) inserted to the level of the mediastinum (measured before placement from the nose along its anticipated course in the esophagus to half the distance between the sternal notch and xiphoid process, then the probe was inserted this distance), and 3) remotely transmitting swallowed capsule (Tcap; VitalSense Philips Respironics, Bend, OR; Figure 2).

Ingestible telemetric body core temperature sensor.
Heart rate and rhythm, end-tidal CO2, and 2 independent pulse oximetry sites were also monitored throughout. Measured ventilation parameters included partial pressure of end-tidal CO2 (P
Verbal contact was maintained by an intercom system buried in the snow near the face of the subject. Criteria for termination of the burial were 60 minutes, core temperature of 35°C, oxygen saturation less than 85%, or at the request of the subject.
Approximately 10 minutes before completion, study personnel began extricating the subjects from the trench. At 60 minutes, the participant was extracted from the snow. The participant was then placed inside a “hypothermia wrap,” which consisted of a sleeping bag atop a thick insulating ground pad, all of which was surrounded by a vapor barrier plastic tarp. Subjects continued to breathe through the AvaPack while being placed in the hypothermia wrap and for the next 60 minutes so that physiological data could be recorded during the rewarming process. Core temperature and monitored data were again observed every minute for another 60 minutes or until the core temperature returned to baseline.
After each burial, participants completed a questionnaire that asked them to subjectively rate the degree of cold sensation for each burial: “On a scale of 1–10, how cold did you feel during the (control/intervention) burial?” Questions were rated on a 1 to 10 Likert scale (1 = extremely cold, 10 = extremely hot).
Primary outcome was the rate of core temperature drop during the burial and rewarming period. Secondary outcome was comparison of esophageal, rectal, and capsule temperatures. An additional secondary outcome measured participants’ cold perception and comfort during each burial.
Statistics
Evaluation of the slopes of the temperature curves during the hour of burial was performed for both intervention and control by fitting a curve to the data points using ordinary least squares regression. Comparison between the slopes was then performed using the paired Student’s
Correlations between Tes, Tre, and Tcap were performed using the Pearson correlation coefficient for each participant. The correlation coefficients for each individual under each test condition were then evaluated by the paired Student’s
Results
Mean snow temperature during the burials was –8.1°C, air temperature –4.0°C, and mean snow density 35.3% (mean snow density of dry slab avalanche debris is approximately 30% 12 ).
One participant declined to perform a second burial, stating severe anxiety during the first FHI trial, and was therefore eliminated from analysis. A different participant could not swallow the esophageal temperature probe before both burials. Additionally, this participant’s capsule did not function properly on 1 trial. This participant was also eliminated from analysis. (See Figure 3 and the Table for description of subject flow and analyses.)
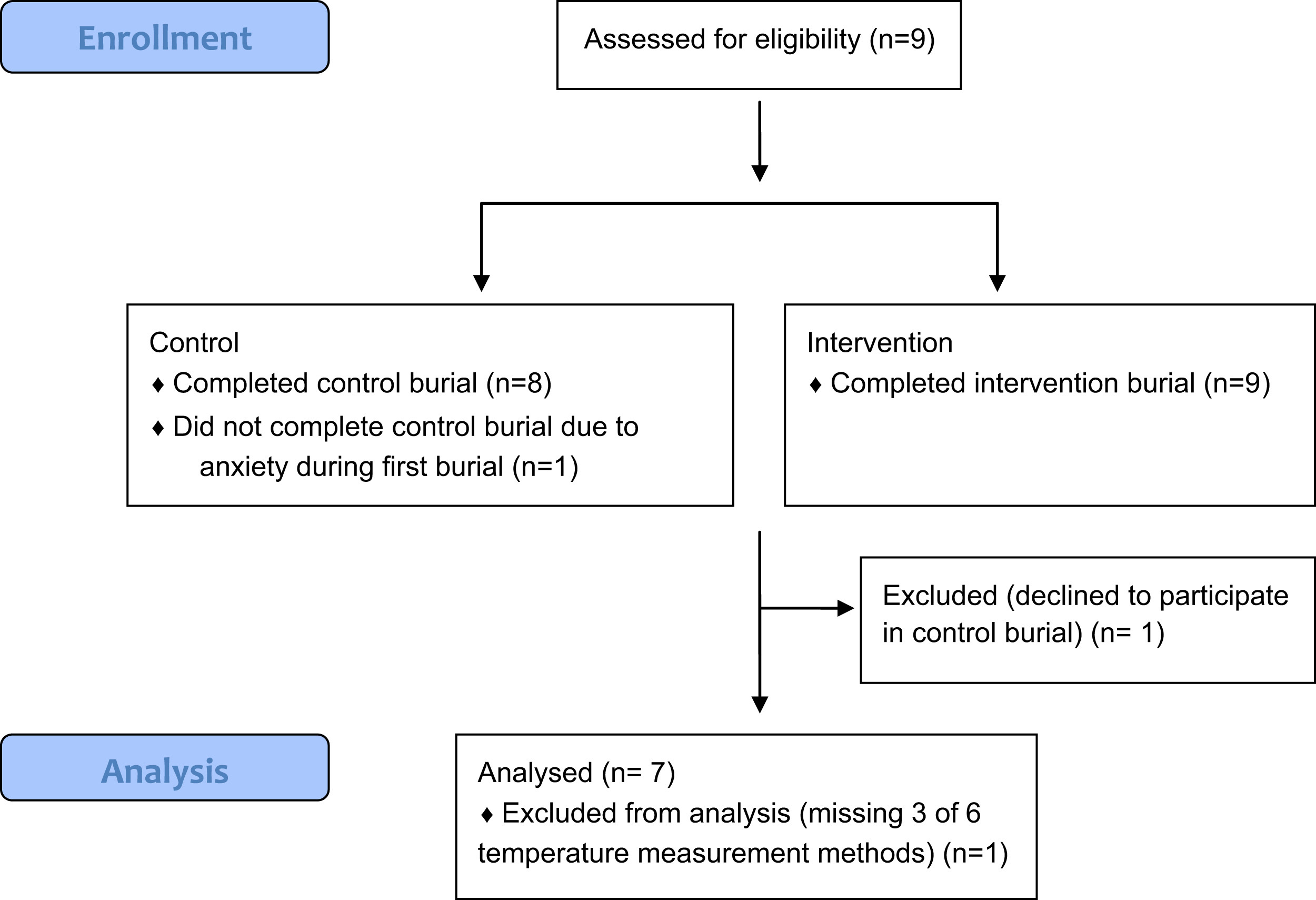
Participant enrollment, exclusion, and analysis.
Summary of data recorded for each participant
FHI, face and head insulation (intervention); NFHI, no face and head insulation (control); Tcap, ingestible capsule; Tes, esophageal probe; Tre, rectal probe.
These participants were excluded from analysis.
The 7 participants having rectal and capsule temperature recordings able to be analyzed had a mean age of 27.2 years (range, 22 to 35 years), height of 176.3 cm, weight of 73.1 kg, and BMI of 23.5 kg/m2. Of these 7 participants, one could not swallow the esophageal probe for either burial, and another participant was unable to swallow it for the NFHI.
Capsule Temperature
For the 7 subjects who had Tcap data for analysis, the mean slope for the NFHI cooling rate was –0.39°C/h (SD ±0.52) and the mean slope for the FHI cooling rate was –0.60°C/h (SD ±0.41;
Subject 7 had only 25 data points (during the 60 minutes) available for Tcap during FHI. When this subject is removed from the analysis, the average slope for NFHI cooling rate was –0.49°C/h (SD ±0.49) and for FHI cooling rate was –0.63°C/h (SD ±0.45;
When the curves were plotted with time on the x-axis and temperature on the y-axis, some individuals maintained temperature better with FHI, but in others the NFHI maintained temperature better.
Esophageal Temperature
For the participants who had Tes for analysis, mean slope for controls was –0.81°C/h (SD ±0.89) and mean slope for intervention was –0.81°C/h (SD ±0.37;
Rectal Temperature
The mean slope for Tre during NFHI was –0.74°C/h (SD ±0.46) and the mean during FHI was –0.74°C/h (SD ±0.43;
Temperature Measurement Correlations
Tes was missing for participant 3 (NFHI) and 5 (NFHI and FHI), so correlations for those 3 participant/state combinations were not possible. In addition, Tcap for participant 7 (FHI) captured only 25 of the 60 measurements during the burial hour, so that participant/state was excluded from temperature comparison analysis. A total of 14 participant/temperature measurement correlations were therefore possible after the 4 exclusions mentioned above. Figure 4 presents a summary of mean temperatures for the measurement methods.
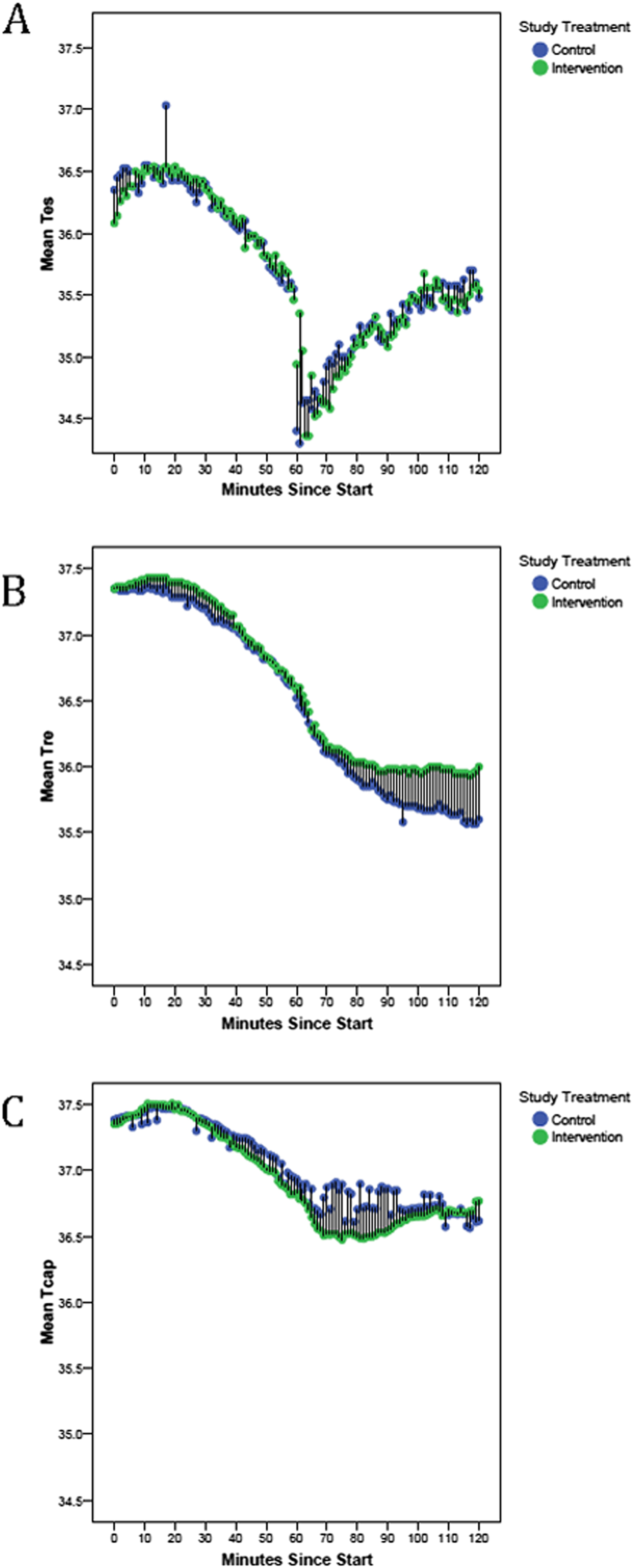
Comparison of the mean temperatures of all participants between the control (blue symbols) and intervention (green symbols) periods for each method of temperature measurement: esophageal (A), rectal (B), and capsule (C). Bars indicate the magnitude of difference between mean temperatures for control vs intervention at a specific time point.
All correlations between the capsule, esophageal, and rectal temperatures were significant at a probability value of less than .001 within the control period and within the intervention period of each participant. Those correlations were then averaged, and the average correlation among the 3 measurement sites were evaluated, with the finding that there were no significant differences in the average correlations, with Tcap vs Tes,
Cold Perception
Postburial questionnaires were received from all except 1 participant. The mean reported cold perception score for FHI was 4.3 (95% CI, 3.6 to 5.0) and for NFHI was 2.4 (95% CI, 1.4 to 3.5).
Discussion
We found that the rate of cooling during snow burial was no different when wearing head and face insulation (FHI) vs without (NFHI). Rates during rewarming followed similar predictable temperature increase patterns. Slopes of temperature measurement methods correlated significantly. These curves demonstrated a steep drop in temperature immediately after extrication, with esophageal temperature showing the steepest drop. This afterdrop phenomenon is attributable to recirculation of peripheral blood after the subject begins to move the body and extremities. During cooling, peripheral vascular beds constrict to decrease the cooling of warm blood in the extremities. During rewarming, these peripheral vascular beds expand, allowing cooled blood to return to the core. The phenomenon has been shown both in snow burial and cold-water immersion. 13 –15
Hypothermia may be accelerated via heat loss from the head and face, as these body areas are extremely vascular areas. Blood flow through each common carotid artery is approximately 350 mL/min and that of the basilar artery ranges from 100 to 200 mL/min. 16 After the common carotid artery bifurcates, the external carotid artery branches into the superficial thyroid, lingual, facial, maxillary, and superficial temporal arteries to supply the face. The superficial temporal and occipital arteries course through the scalp and supply most of the vasculature to these areas. The internal carotid artery also contributes to the face vasculature via the ophthalmic artery, which branches into the supraorbital artery, supplying much of the forehead. The vasculature of the face and scalp runs close to the skin surface and therefore greatly contributes to heat loss.
As anticipated, participants felt subjectively colder without head and face insulation. This is because of the extremely vascular and nervous innervation to the scalp and face. In addition, the cold perception was likely enhanced by a small amount of moisture from snowmelt on the scalp and face that likely accompanied the NFHI burials.
Heat loss during snow burial follows a relatively expected rate of decline. Cooling rates in water are faster than in snow because of higher conductive properties of water vs air (25:1). Cooling rates during cold-water immersion for a similar insulation system as in our study are about 3° to 5°C/h. 17 Studies of cold-water immersion hypothermia show that core body temperatures fall faster when the head is submerged along with the rest of the body. 18 When shivering thermogenesis was inhibited by meperidine, the rate of core temperature decline was faster (39%) in subjects who have their head and face submerged than the increased total body surface area of 7% would predict. 19 Our results during snow burial did not show a similar trend.
Other studies have shown a variable effect of local face and neck cooling on core temperature. Devices used to induce hypothermia by cooling the head and neck produce steep drops in local skin cooling and tympanic temperatures20,21 but not a similar drop in core temperature. The effect of head and neck insulation on our small study group of subjects could be similarly variable.
The gold standard for core temperature measurement is the blood temperature in the pulmonary artery. For obvious reasons, this is not practical in many studies outside the operating room or intensive care unit. Temperature measurement in research and field environments can be challenging because of the invasive and uncomfortable nature of rectal and esophageal probes. Esophageal probes are the closest simulation of core temperature by proximity, but as this study showed are poorly tolerated by many subjects. Prior studies have described the correlation of temperature monitor systems in an effort to find the most accurate and perhaps least invasive measurement. 22
All 3 of our temperature measurement methods (Tcap, Tes, Tre) correlated significantly when mean slope was examined. We did observe potentially clinically important differences in absolute temperature, however, as both Tre and Tcap were higher overall than Tes. Most, 23 although not all, support the ingestible capsule thermistor (Tcap) as a reliable estimation of core temperature. We support the less invasive and more comfortable ingestible temperature capsule for measuring core temperature in future studies of this nature. Calibration of the device, ingestion timing, and electromagnetic interference must, however, be tested and controlled before study with subjects. 23 The capsule data in our study showed good reliability during cooling but variable measurements during rewarming, which will require further study.
Baseline temperatures measured by the esophageal probe were lower than those of the other measurement methods. This was an unexpected finding. Although the esophageal probe placements were performed carefully, it is conceivable that they could have been placed more cranially than anticipated. If this did occur, cold air from the trachea could have cooled the esophageal probe slightly.
Many physical and physiological mechanisms are involved during an actual avalanche. Cooling rates will be affected by insulation on other parts of the body as well as associated trauma and other local conditions such as density and temperature of snow. Although the results of this study showed no difference in cooling rates with head and face insulation, other uncontrollable factors such as these will affect overall cooling rates.
Limitations
Our study included a limited number of participants, and a study with larger numbers may show different results. Although we did not recruit our goal sample size, the results of the 7 subjects did not suggest that we missed a clinically significant difference between conditions. Certain participants did not tolerate the esophageal probe, which slightly limited data comparisons. The ingestible temperature capsule did not record reliable data for certain trials, and reception was variable during the rewarming phase. One disadvantage of the swallowed temperature capsule is that it is a free-floating probe; its position may change more rapidly in some people, and gastrointestinal contents and conditions can influence measurements, resulting in slight variability. 23
During burial, the body melts the snow with which it has direct contact, creating a thin air cavity. Because the body is placed in a seated position, the cavity forms most significantly around the head and face. This air cavity forms an insulating barrier between the head/face and the snow that may slow cooling by limiting direct contact with surrounding snow. Certain subjects may have positioned their head and face in such a fashion to minimize direct contact and therefore lower the rate of heat loss. The use of the Gore-Tex hood prevented melted snow from wetting the head directly. Even though Gore-Tex is thin, the barrier likely prevented some unmeasurable conductive heat loss. These 2 factors may have limited the cooling rate vs that of an actual avalanche burial.
Conclusions
Those who enter avalanche terrain should take protective measures to prevent injury and fatality if caught. Helmets should be worn to prevent head trauma. Based on the results of this study, however, helmets and face gear do not prevent cooling during simulated avalanche burial. The ingestible temperature capsule provides a comfortable alternative to measuring core temperature in avalanche burial studies.
Footnotes
Acknowledgments
The authors thank Nicholas Kroll, MD, and Heather Beasley for their support and assistance during the study.