
Abstract
Introduction
The popularity of adventure recreation in wilderness areas across the world continues to increase. Nevertheless, the risk of injury and illness remains significant. The purpose of this study is to analyze the mountain rescue operations performed in Slovenia between 2011 and 2015.
Methods
This retrospective study reports mountain rescue operations documented by the Slovenian National Mountain Rescue Association. The annual number of ground-based and helicopter-based rescues were identified and compared. For 2015, the indication for rescue and the severity of injury were also analyzed, specifically for interventions requiring the use of a helicopter.
Results
From 2011 through 2015, the number of rescues remained consistent with an annual average of 413 (SD ±15; range, 393–434) rescues. However, the percentage of ground-based rescues varied significantly year by year (P=0.016), with highest rate in 2014 (68%) and the lowest in 2015 (56%). In 2015, 434 mountain rescue operations were reported in Slovenia. Injury accounted for 44%, illness for 10%, and fatality for 9% of the rescues. In 37%, no illness or injury was reported. Helicopter rescue was used in 190 (44%) of all interventions. Among the 190 helicopter rescues, 49% of patients had nonfatal injuries, 29% required no medical treatment, 15% had illness, and 7% had fatal injuries.
Conclusions
A significant number of mountain rescue operations were conducted in Slovenia from 2011 through 2015. Most of these were needed for injured, ill, or deceased persons. A notable number of rescues in 2015 required a helicopter.
Introduction
The outcome of patients in a mountain environment can be dramatically improved by rapid evacuation and treatment.1,2 In Slovenia, this is facilitated by ground-based mountain rescue teams working in close collaboration with helicopter-based medical services. Slovenia’s mountain rescue system has been established for more than 100 years. However, it was not until 1968 that a helicopter-based mountain rescue took place. In 2003, the first major professional helicopter rescue service in the country since Slovenia’s independence from Yugoslavia was introduced as a pilot project. In 2006, the first helicopter emergency medical service (HEMS) was established and registered as Helikopterska Nujna Medicinska Pomoc (HNMP).
In Slovenia, 2 different types of HEMS provide rapid medical care and transport in either urban or remote areas. The first, Slovenian HEMS, mostly handles incidents away from the mountainous areas and covers the majority of secondary transports with teams that include a physician and an emergency paramedic. The second, Slovenian Mountain Rescue Service HEMS, is associated with Slovenian Mountain Rescue Service (Gorska Resevalna Zveza Slovenije [GRZS]) and covers mountainous terrain; special skills and equipment are required to navigate these difficult areas.
GRZS was established in 1912 and is organized as a federation of partly independent and geographically determined voluntary nonprofit units carrying out the humanitarian task of public interest. Its mission is to protect, rescue, and aid people having emergencies in difficult, remote terrains. Members of GRZS include mountain climbers, mountain guides, and specially skilled members such as doctors, paramedics, and rescue dog guides. The GRZS teams are composed of mountain rescuers and a physician; however, they do not include an emergency paramedic. GRZS provides its members with education and training in first aid and specialized rescue techniques. Becoming a mountain rescuer with GRZS requires 3 years of training followed by a final examination and licensing. To maintain a license, all helicopter mountain rescuers and doctors are required to complete a training program and medical examination. The training program content is regulated by government agencies. The GRZS’s Commission for Helicopter Mountain Rescue follows strict guidelines to keep the technical knowledge and equipment standards high. The main safety criteria are appropriate mountain rescue and flight training, competence of air and ground crews, and adequate means of communication between the air and ground crews.
Until recently, HNMP covered the entire country from an airport situated near the country’s capital city of Ljubljana. In November 2016, a second HNMP center was established at the airport in Maribor, situated in the east of the country. The division of service between the 2 HNMP units is based on proximity of the site where the service is needed (Figure 1A).
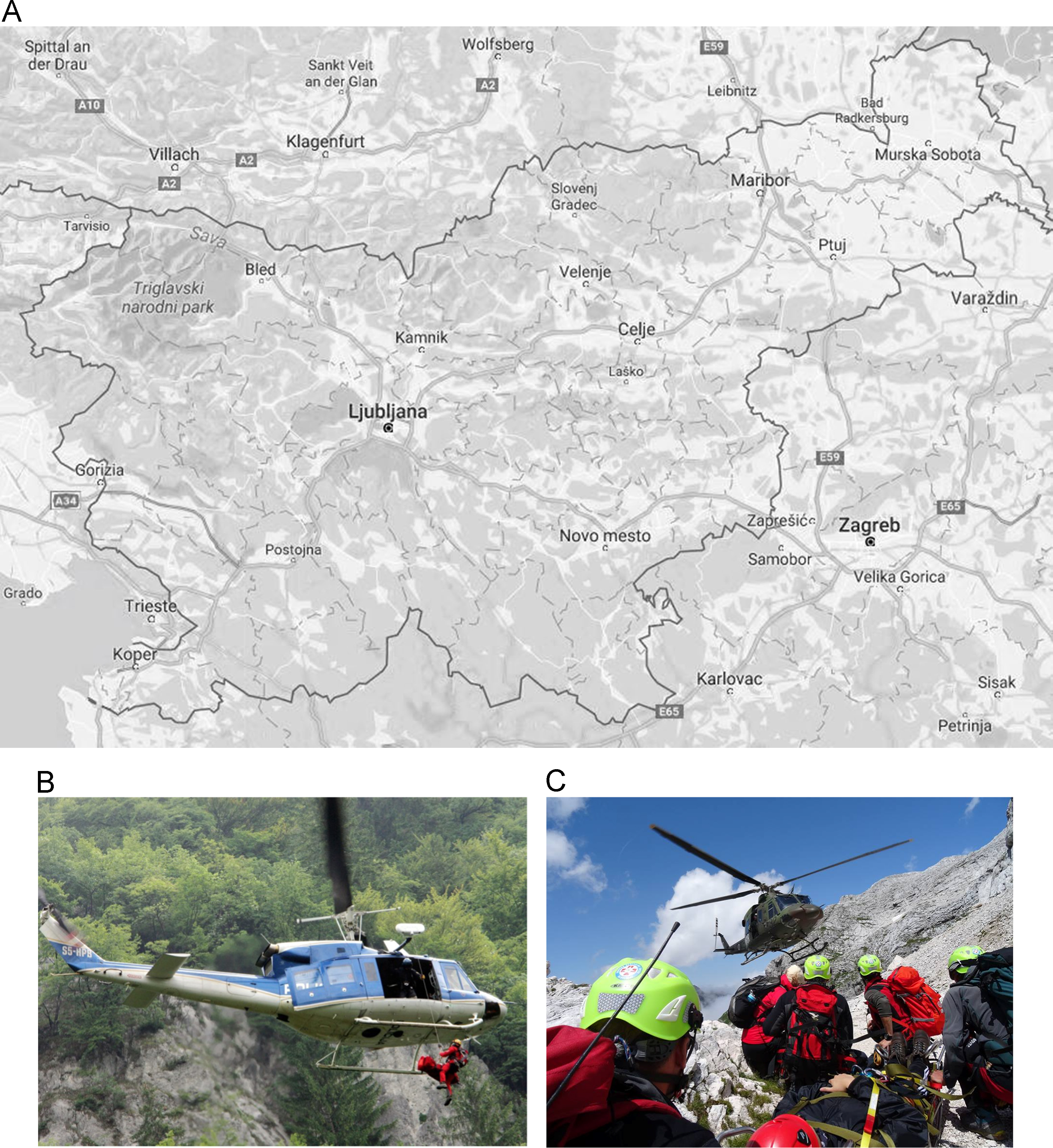
A, Map of Slovenia with the sites of the rescue helicopters and mountain rescue centers included. The airport base near Ljubljana also serves as the base for mountain rescue teams. B, Police helicopter evacuation. C, Military helicopter evacuation. Source: A, Google maps. B and C, Miha Gašperin, MD, Slovenian Mountain Rescue Association.
HNMP HEMS teams work in tandem with ground-based GRZS teams dispatched to a rescue scene. Slovenian helicopter mountain rescue operations are performed using both police (Figure 1B) and military (Figure 1C) helicopters and are crewed by HNMP HEMS teams. There are 2 professional helicopter teams that have pilots and winch operators specially trained and equipped for mountain rescue. Both are located at Slovenia’s main airport near Ljubljana. Military and police helicopter teams are not trained or equipped for search and rescue operations in the mountains; thus, the country relies on the specially trained HNMP teams for all mountain rescues. The responsible authorities in Slovenia are currently working on further integrating the 2 services and providing specially equipped medical and rescue helicopters that would be specifically used for mountain rescue operations.
Slovenia is a small and geographically diverse country covering 20,273 km2. The Julian Alps, situated in the northwest of the country, attract a considerable number of visitors each year, which has led to the development of an extensive trail system connecting large numbers of mountain huts. Heliports established along much of this trail system can be used by HNMP for extrication. The main tourist season extends from June to October. During this time, 3 emergency helicopter teams are available, with 1 dedicated solely to mountain rescue. This is reduced to 2 teams for all services during the rest of the year. When an accident is reported, a dispatcher activates the nearest ground-based GRZS mountain rescue team. There are 17 local GRZS groups in the country, each headed by a chief rescuer. Helicopter assistance can only be requested by a chief rescuer provided that there is a suitable medical indication and favorable flying conditions. Once a flight has been approved, a police officer, a helicopter mountain rescuer, and a doctor are dispatched. The majority of patients evacuated from the Julian Alps are transported to the General Hospital in Jesenice, located close to Triglav National Park. Patients with more severe injuries or illnesses are transported to the University Medical Centre in Ljubljana.
This study documents the mountain rescue operations performed in Slovenia from 2011 to 2015. For 2015, the indication for rescue and the severity of injury was also analyzed. The aim of this study was to identify causes of accidents requiring rescue and to stratify the severity of injuries assessed in the field as requiring evacuation by helicopter.
Methods
This study is a retrospective data analysis detailing rescue and recovery operations from the Slovenian National Mountain Rescue Association combined with those of police and military helicopter operators. Incident data were gathered from standardized report forms generated by medical and rescue personnel on the scene.
The numbers of ground-based and helicopter-supported rescue operations from 2011 to 2015 were compared. A more detailed analysis of rescue interventions was performed for 2015. This examined the indication for activation of the search and rescue operations and aimed to determine specifically which interventions required the use of a helicopter. Indications for intervention were divided into 4 groups: injury, illness, death, and no medical indication. The severity and epidemiology of injuries requiring evacuation in 2015 were also studied. The 7-level National Advisory Committee of Aeronautics (NACA) scoring system of patients was used for stratifying incident severity and determining the necessity for air transport (Table 1). NACA scoring is a risk stratification tool widely used in helicopter rescue that provides a reliable prediction of morbidity for patients who might require helicopter transport. 3 NACA scores were assigned to patients by the team physician to assess the severity of their clinical state.
National Advisory Committee of Aeronautics (NACA) scoring systems used as risk stratification tool to predict morbidity of patients who might require helicopter transport
Data are presented as mean±SD with range, as appropriate. Statistical analysis included χ2 tests, which were performed using SAS EG v. 6.1 with significance accepted at P≤0.05.
Results
Results for the 5-year period from 2011 through 2015 show 413±15 (393–434) rescues performed annually in Slovenia. The number of ground rescues ranged from 236 to 279, and the number of helicopter rescues ranged from 133 to 190 (Figure 2). During this time, an average of 38% of all rescues used helicopter transport. The total number of rescues remained stable annually, however, there were significant differences in the rate of helicopter rescues over the years (P=0.016). The rate of situations using helicopter rescue intervention was highest in 2015 (45%) and lowest in 2014 (32%). The rates for 2011 through 2013 ranged from 38 to 40% (Figure 2). A more detailed analysis of rescue operations in 2015 revealed that among the 470 persons involved, 176 (37%) did not require treatment, 206 (44%) were injured, 48 (10%) were ill, and 40 people (9%) were already dead (Figure 3). Among the 190 helicopter rescues, 49% had nonfatal injuries, 29% required no medical treatment, 15% had illness, and 7% had fatal injuries. Data on the reported reason for rescue were not significantly different between rescues using a helicopter and those done on foot (P=0.094), although when combined into 2 categories (Injuries/Illness and Death/No treatment required), there were significant differences in the rate of helicopter rescues (P=0.024). Patients with injuries and illnesses were rescued with a helicopter 25% of the time compared with 17% for deaths and evacuations, for which no medical treatment was required.
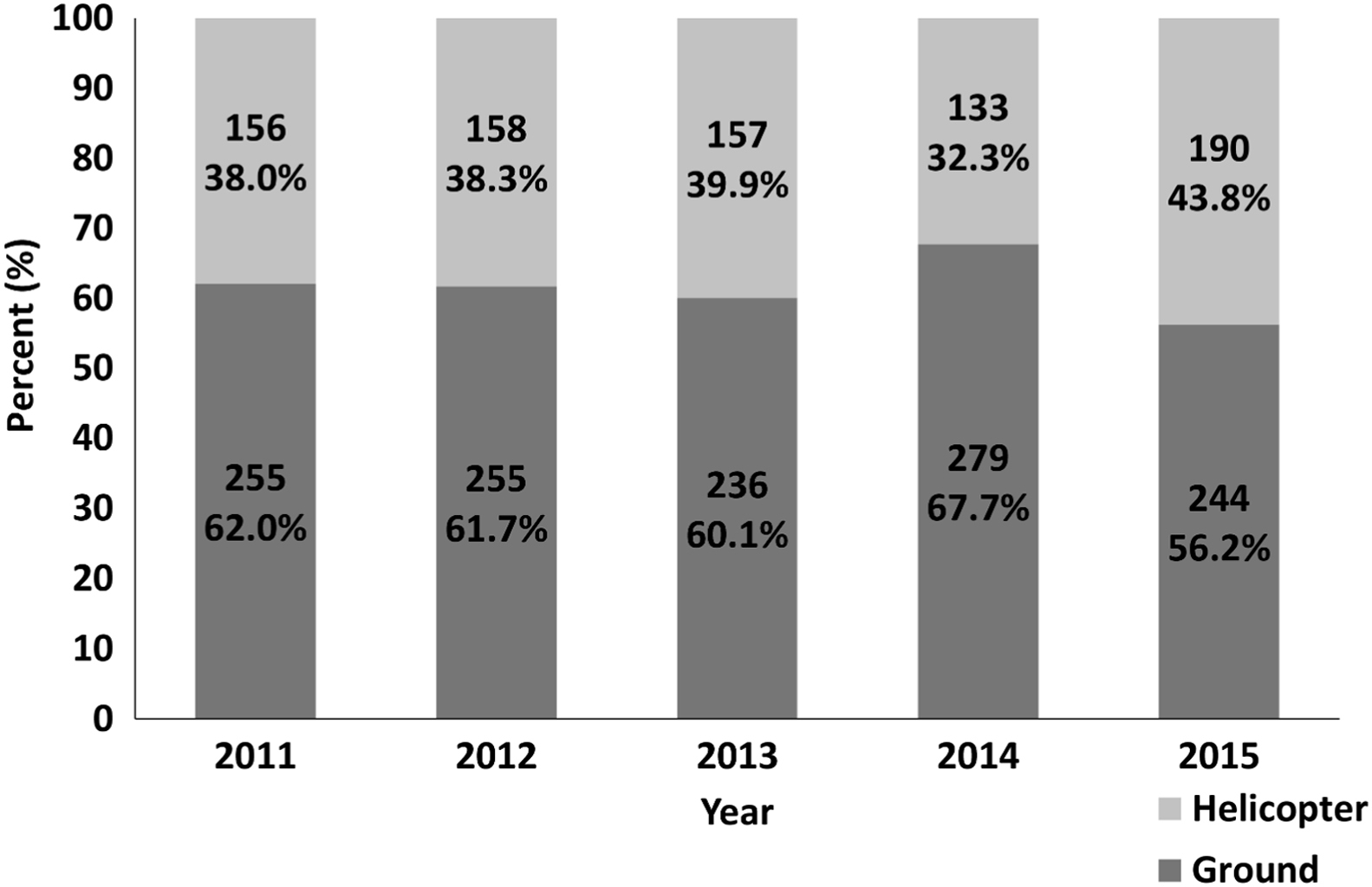
Number and percentage of rescues by ground-based and helicopter-based transportation for years 2011 through 2015.
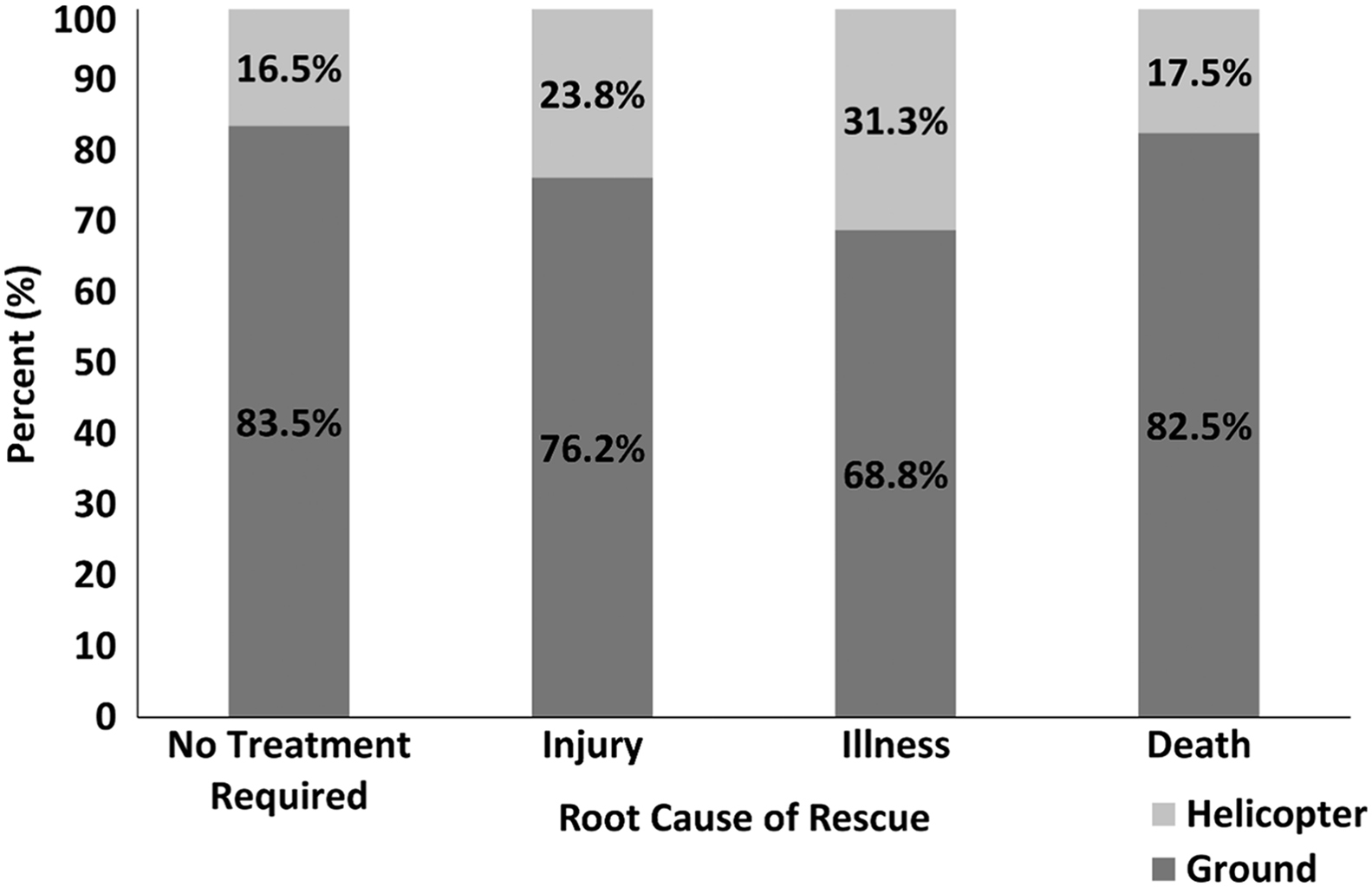
Root cause of interventions and rescue type for 2015 rescues (n=470).
The most frequently encountered injury in 2015 was to the lower extremities and the most common illness was exhaustion. Of the NACA scores determined by a physician at the scene of the incident, the majority of patients received scores requiring moderate to no emergency intervention (scores 1–3). Thirty-seven percent of patients received a score of 3 or higher (Figure 4). The NACA scores reported in Figure 4 were assessed in the summer, when evacuations tend to be easier. However, the true overall average NACA score for the year, including off-season rescues, is most likely higher.
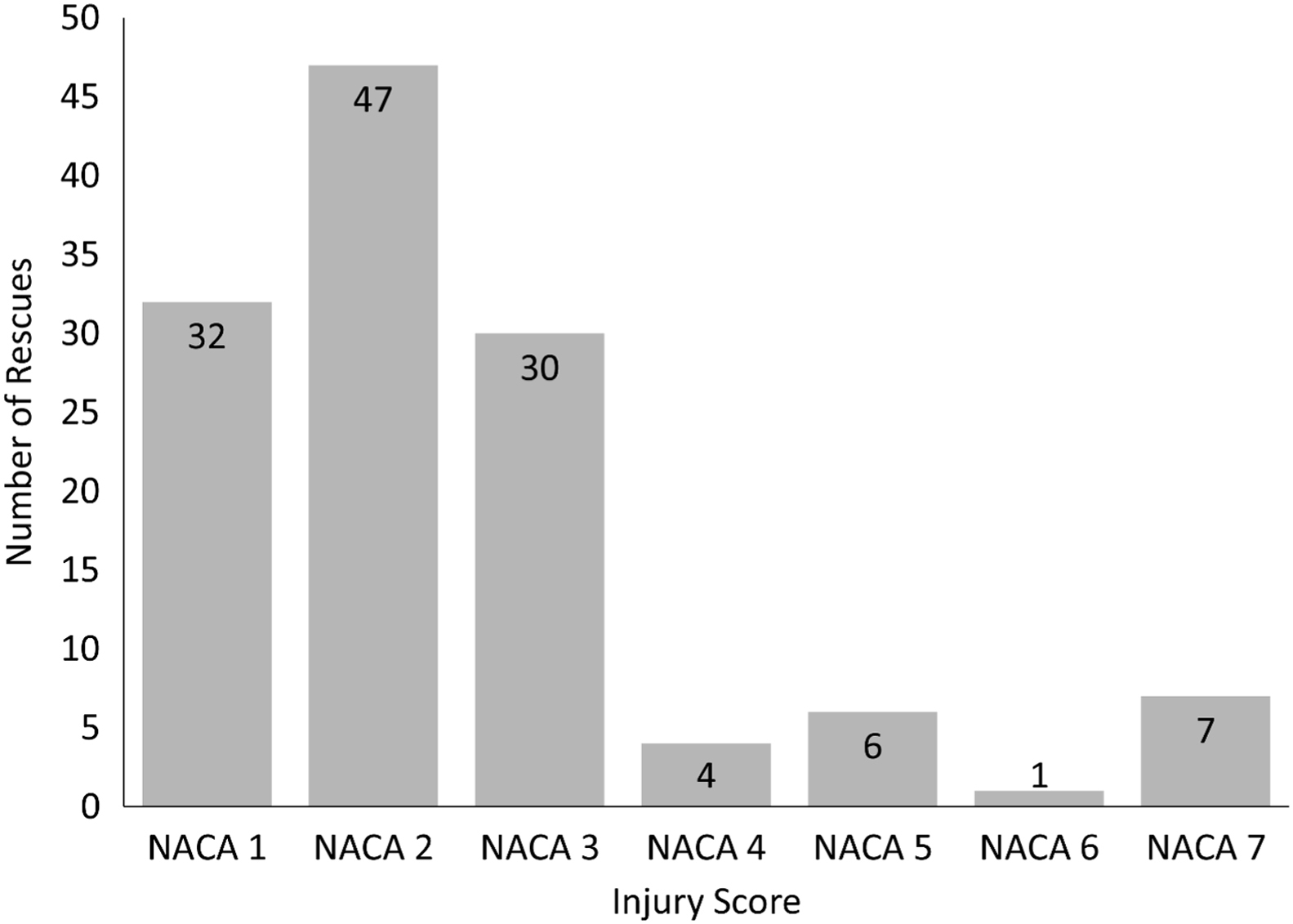
Severity of injuries by NACA scores assessed to patients by team physician (n=127) in 2015.
Discussion
In the 2 decades before the study period, there was thought to be an increase in the total number of mountain rescues due to the growing number of tourists visiting the Slovenian mountains. However, our study found that the total number of reported rescues remained relatively stable throughout the 5-year study period, despite reported increases in total mountain rescues seen throughout previous years in neighboring countires.4,5
Our analysis of data gathered in 2015 revealed only root causes and characteristics of the incidents and found no major deviations from year to year. Generally, the distribution of significant root causes of rescues involving evacuation and injury in the Slovenian mountains was similar to that reported in epidemiological studies done in recreational areas in the United States and other countries, with injured and uninjured or lost persons being the most common. 6 –10
A notable number of operations in the year 2015 (44%) required the use of a helicopter, with the majority involving an injured patient. When compared to all rescues, rescues using a helicopter most frequently involved injuries and illnesses, rather than evacuation only (no medical treatment) or death. In similar studies that analyzed rates of helicopter use by wilderness rescue services, the values varied widely from 27 to 64%.8,9 These findings, when combined with NACA scoring discussed below and previous studies looking at Slovenia’s HEMS systems, seem to reflect the impactful use of helicopters by HNMP services. 4 ,10–14
However, a concerning trend in the data is the increasing number of interventions in which no medical treatment was needed. In a previous study, interventions for patients given NACA scores 1 and 2 were seen to be increasing. 3 Our data similarly reflect a significant overuse of HEMS services based on NACA risk stratification. Of those patients given a NACA score, 37% met the criteria for air transport, whereas the actual percentage of patients transported with a helicopter in 2015 was 44%. We theorize that this is most likely due to overuse of a helicopter team by ground-based teams because the helicopter team is on call and readily available for mountain rescue operations in the summer season. In the off-season, the helicopter service is not as easily available, resulting in decreased demand by ground-based rescue operation leaders. The helicopter-based team is called only in cases in which patients are very sick, severely injured, or very remotely located. Overall, we suspect that the average NACA scores of off-season patients are likely higher, due to this variability in helicopter utilization. Thus, seasonal variations can be explained by the availability of an on-call helicopter mountain rescue team ready and waiting in the helicopter base during the summer season. The ground mountain rescuers are more likely to decide to use a readily available on-call team. In the off season, on-ground rescuers would have to wait 1 to 2 hours for the helicopter mountain rescue team to gather and arrive to the scene and are therefore more likely to complete the intervention on-ground.
In the future, reorganization of helicopter rescue operations to include purposive helicopters and fully professional teams might bring an end to the tradition of volunteer-based helicopter mountain rescue in Slovenia.
Study Limitations
The primary limitation in our data is that some patients who were rescued by a helicopter team in 2015 did not receive a NACA score. This was due to off-season helicopter rescue situations in which a team physician was not available to assess patients or emergency assessment forms were missing. All emergency physicians are required to fill out the emergency protocol paperwork. During the 85- to 90-day summer season, the mountain rescue helicopter team on call includes a team physician who provides every rescued patient with a NACA score. However, in the off season, the protocols are not followed consistently. This could be contributed to the inconsistent composition of the rescue teams or the absence of a team physician. This has been a problem during the off-season since this system was established.
An additional limitation of our data gathering is that the data did not capture activity at the time of the incident, thus making it impossible to draw conclusions about the rigor of an activity causing the injury or illness. Quantitative data on root causes of injury and illness in 2015 are not presented here, but the most common causes were addressed for completeness.
Conclusions
These new data further validate trends seen in international professional rescue organizations. They also serve to characterize a rescue operation that coordinates resources from multiple professions and agencies in a small country with a rich history of mountain sports and tourism. By further integrating helicopter mountain rescue teams with the HEMS teams in Slovenia, professional teams could be available all year. However, as our data indicate, care must be taken when considering the appropriate use of helicopters in wilderness rescue. We have demonstrated that a well-established service with well-trained volunteers and professionals with a “typical” backcountry patient population often makes significant use of helicopters when there is no medical indication. This is likely due to seasonal variations in rescue crew members and helicopter availability. Drawbacks to overuse of helicopters include risk to flight crews and wasteful use of costly medical resources. We hope with further dissemination of standardized scoring systems and evaluation protocols that overuse of HEMS will be reduced. Future reorganization of helicopter rescue operations in Slovenia with purposive helicopters and fully professional ground and HEMS teams should continue to improve the quality of patient care and resource use. International collaboration between the Mountain Rescue Association of Slovenia and International Commission for Alpine Rescues is ongoing and puts this 100-year-old mountain rescue service on par with other rescue services worldwide.
Acknowledgment: We acknowledge the Slovenian National Mountain Rescue Association for sharing their data and experiences.
Author Contributions: Study concept and design (GRD); acquisition of the data (NW, MG); analysis of the data (CC); drafting of the manuscript (GRD, NW, MG, JGD); critical revision of the manuscript (JGD); and approval of final manuscript (JGD, CC, NW, MG, GRD).
Financial/Material Support: None.
Disclosures: None.
Footnotes
☆
Presented in abstract form at the World Congress of Wilderness Medicine, Telluride, CO, August 2, 2016.