
Abstract
Objective
To continuously monitor oxygen saturation (SpO2) by pulse oximeter and assess the development of acute mountain sickness (AMS) using the Lake Louise Score (LLS) during ascent from 1154 to 4559 m in 2 groups of subjects: 10 moderate-altitude residents (MAR; ≥1000–≤2500 m) and 34 low-altitude residents (LAR). MAR are reported to have a lower incidence of AMS during ascent to higher altitudes compared with LAR. Whether this is related to higher SpO2 is still open to debate.
Methods
Seventy subjects were recruited; 24-hour SpO2 monitoring with finger pulse oximetry was performed. All subjects rode a cable car from 1154 to 3275 m and then climbed to 3647 m, where 60 subjects (LAR) overnighted. The second day, 34/60 LAR reached the highest altitude. Ten subjects who lived permanently at 1100 to 1400 m (MAR) climbed directly to 4559 m without an overnight stop.
Results
One LAR was excluded from the analysis because he performed a preacclimatization. We compared data of 10 MAR with data of 33 LAR who reached 4559 m. Two MAR had an LLS of 3, and 8 scored <3. Six LAR had an LLS of 3 to 4, 8 scored ≥5, and 19 scored <3. SpO2 monitoring showed higher mean SpO2 in MAR during ascent above 3600 m compared with LAR (MAR, 79±4% vs LAR, 76±5%; analysis of variance, P = .03).
Conclusions
The results of this preliminary study suggest that residence at moderate altitude allows maintenance of higher SpO2 and reduces risk of developing AMS during rapid ascent to higher altitude.
Introduction
Progressive exposure to high altitude is characterized by progressive hypoxemia, which worsens with exercise. Travel to elevations above 2500 m is associated with the risk of developing acute mountain sickness (AMS) or other more severe high-altitude diseases. 1 AMS is assessed by the Lake Louise Acute Mountain Sickness Scoring System (LLS), a well-validated questionnaire for field evaluation of AMS. An LLS score ≥3 is diagnostic of altitude sickness. 1 The best way to prevent AMS is to undertake an adequately slow ascent to high elevation, which allows time for acclimatization. Other nonpharmacologic prophylactic measures for AMS are repeated exposures to hypoxia in the time preceding a high-altitude excursion or spending up to 6 to 7 days at approximately 2200 to 3000 m.2,3 In an article regarding the development of AMS at the Regina Margherita Hut, pre-exposure is defined as having spent more than 4 days above 3000 m during the 2 months preceding the climb. 4
Likewise, individuals who usually reside at moderate altitude (≥1000–≤2500 m) achieve more rapid acclimatization to higher altitude and have reduced incidences and severity of AMS compared with those who usually reside at low altitude.5,6 The few studies that have addressed this topic reported higher oxygen saturation measured by pulse oximeter (SpO2), above 4000 m in moderate-altitude residents (MAR) compared with low-altitude residents (LAR).5,6 In these studies, SpO2 was measured at rest for only a few minutes, and no data during exercise were available. Only 1 study 7 reported a comparison between endurance performance and SpO2 during exercise in MAR and LAR in a well-controlled laboratory setting at 4300 m. This study reported that MAR were able to exercise at a higher intensity and maintained higher exercise SpO2 compared with LAR. However, these results were obtained at the third day of residence at altitude, 7 when the first changes involved in acclimatization have already occurred, especially the ventilatory acclimatization that contributes to increased SpO2.
No study has continuously monitored SpO2 during progressive high-altitude ascent from moderate to high altitude in MAR compared with LAR, particularly during exercise that induces physiologic responses that may exacerbate the development of AMS.
We had the opportunity to monitor SpO2 and LLS during the entire ascent from Alagna (1154 m) to the Regina Margherita Hut (4559 m) in both MAR and LAR. In a previous article, we reported data among LAR. 8 Now we report data of SpO2 monitoring and LLS in MAR compared with LAR.
Methods
Recruitment
We designed a 4-week study on Mt. Rosa at the beginning of the climbing season, aiming to monitor SpO2 for 24 hours and assess the development of AMS in climbers during the ascent to the Regina Margherita Hut (4559 m). The study purpose was explained in flyers posted in the Alpine Guide office and at the cable car base. Seventy subjects intending to climb to the Regina Margherita Hut were successively enrolled and provided informed consent. All subjects were asked about anthropometric data, altitude of residence, occupation, habitual physical activity, medical history, and previous AMS events. We defined “moderate altitude residents” as subjects who have resided at an altitude between 1000 and 2500 m for at least 12 months. Subjects taking drugs for AMS prophylaxis were excluded from the study. The study complied with the principles of the Declaration of Helsinki and was approved by the Ethics and Research Committee of the Medical School of the University of Ferrara, Italy.
Study Design
All 70 subjects were equipped with a 24-hour data memory pulse oximeter with a finger sensor (Pulsox-300i, Konica Minolta, Osaka, Japan) to monitor SpO2 and heart rate (HR). The pulse oximeter was removed on arrival at the Regina Margherita Hut.
Subjects were asked to complete 2 questionnaires: The Lake Louise Questionnaire for the assessment of AMS while in Alagna, at the Gnifetti Hut (on arrival, in the evening, and on the following morning), and on arrival at the Regina Margherita Hut. On the same sheet, the subjects also recorded the starting and arrival time and any exposure to altitude in the previous 2 months. The Baecke questionnaire
9
for the measurement of habitual physical activity. This is a self-administered questionnaire separated into 3 dimensions: work, sports, and leisure activity. Each activity is scored in a range from 1 to 5.
On the first day, subjects rode a cable car from 1154 to 3275 m. They then climbed to the Gnifetti Hut (3647 m), where 60 subjects (all LAR) stayed overnight. On the second day, only 34/60 subjects climbed to the Regina Margherita Hut (4559 m). Twenty-six subjects ceased further climbing due to bad weather (11), poor health (7), or because the ascent was too demanding (8). Ten of the 70 subjects (3 females), permanently residing in Alagna and surrounding area (1100–1400 m, MAR), intended to climb directly from 3275 m to 4559 m. These subjects were excluded from the previous article. 8
Data Collection and Analysis
Data were stored at 1-second intervals and processed by DS-5 Minolta software.
For the analysis, we divided the data into 4 frames: at rest at 1154 and 3275 m, during the ascent to the Gnifetti Hut, and during the ascent to the Regina Margherita Hut. The mean values of HR, SpO2, and time spent under different SpO2 values (90%, 85%, and 80%) were evaluated. Exercise was identified by the time recorded by the subjects in the information and LLS sheet and confirmed by the HR.
Statistical Analysis
Statistical analysis was performed using a statistical software package (GraphPad Prism 5; GraphPad Software, San Diego, CA). Data are presented as mean ± standard deviation where appropriate. Demographic data were analyzed with the unpaired Student’s t test. Comparison among groups at different altitudes was performed by repeated-measures analysis of variance (mixed model). The Pearson’s correlation analysis was used to test the effect of age, body mass index (BMI), and habitual physical activity on LLS score. The level of significance was set at P < .05.
Results
One LAR performed a staged ascent, 2 spending the previous week at 2300 m with daily climbing to 3325 m, and was excluded from the analysis. We therefore compared the data of 10 MAR with the data of the remaining 33 LAR who ascended to 4559 m.
No differences were found in age and BMI. Age was 42±10 years and 35±11 years and BMI was 22.6±3.3 kg/m2 and 22.5±2.1 kg/m2 for MAR and LAR, respectively. Two MAR were alpine guides, whereas the others worked in an office. Five LAR had an active job, and 28 worked in an office.
The mean scores of the 3 physical activity items were not significantly different, including physical activity at work (MAR: 2.65±0.89; LAR: 2.70±0.93), sport during leisure time (MAR: 5.86±2.67; LAR: 5.19±3.3), and physical activity excluding sport during leisure time (MAR: 2.87±0.34; LAR: 3.16±0.82). The P values were .47, .29, and .07, respectively.
Regarding pre-exposure to hypoxia, none of the remaining 43 subjects performed a true preacclimatization, according to the definitions reported in the literature2,4: 2/10 MAR and 5/33 LAR spent 6 to 7 days at 1800 m hiking up to 2300 to 2500 m during the previous 2 months. Six additional LAR and one MAR made a 1-day excursion above 3500 m in the previous 2 months.
We considered only the LLS at arrival at 4559 m. Two MAR had an LLS of 3. The remaining 8 had an LLS <3. Among the 33 LAR, 6 reported an LLS ≥3 but <5; 8 reported an LLS ≥5, and the remaining 19 scored <3 (Figure). No significant correlation was found between LLS and BMI, age, or physical activity.
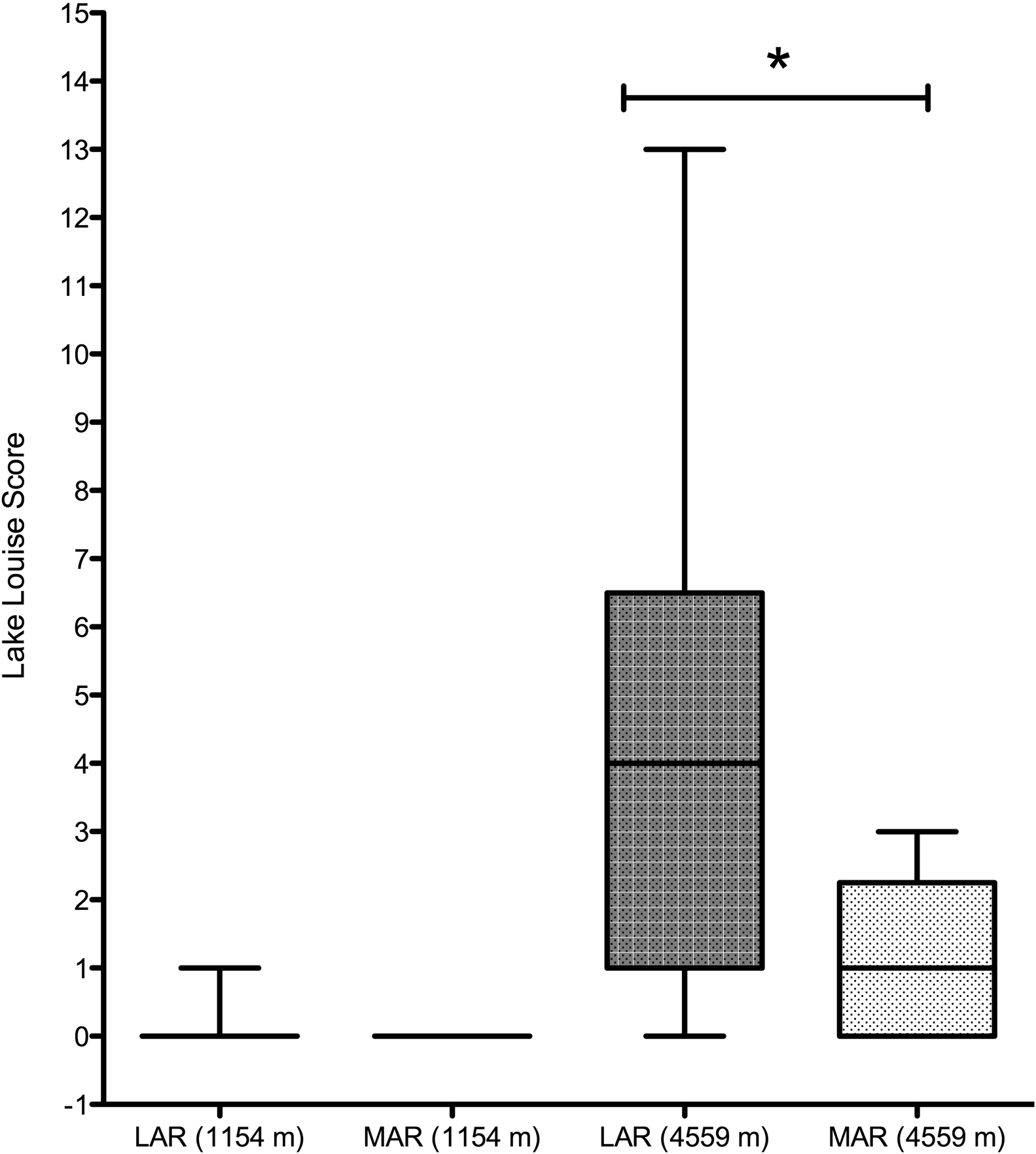
Lake Louise Score (LLS) in the 2 groups at 1154 and 4559 m. The central box represents the values from the lower to the upper quartiles. The middle line represents the median. The vertical line extends from the minimum to the maximum value. *P < .05, Student’s t test. LAR, low altitude residents; MAR, moderate altitude residents.
We did not find any difference in resting SpO2 at 1154 and 3275 m nor during exercise from 3275 to 3647 m (Table). However, MAR maintained a significantly higher SpO2 during exercise from 3647 to 4559 m (analysis of variance, P = .004) and spent less time with SpO2 <90% (Table).
Mean SpO2 at rest, during exercise and % of time spent with different SpO2 in MAR and LAR.
SpO2, oxygen saturation by pulse oximeter; E1, exercise from 3275 to 3647 m; E2, exercise from 3647 m to 4559 m; MAR, moderate-altitude residents; LAR, low-altitude residents.
All data are represented as mean±SD.
The mean HR during exercise was not different between MAR and LAR (MAR: 108±24 beats/min, LAR: 115±16 beats/min).
Regarding the duration of ascent, MAR spent 3 hours and 28 minutes (±43 minutes) whereas LAR spent 4 hours and 17 minutes (±1 hour and 15 minutes) to climb from 3647 to 4559 m.
Discussion
In this study, we had the opportunity to monitor SpO2 during the entire ascent from Alagna to the Regina Margherita Hut and assess the development of AMS in 2 groups of subjects who permanently resided at low (<1000 m) or moderate altitude (≥1000–≤2500 m). Continuous monitoring of SpO2 allowed us to show that subjects resident at moderate altitude have higher SpO2 during ascent above 3600 m in comparison with lowlanders. Less severe desaturation is associated with greatly reduced incidence of AMS. The acclimatization acquired while living at moderate altitude presumably allows maintenance of higher SpO2 during the strenuous exertion required to reach higher altitudes, when hypoxic stress is more evident and the need for acclimatization is greater. This peculiarity facilitates tolerance to a hypoxic environment, thus permitting a faster ascent rate than normally recommended. 2
As reported in the literature,5,6 the higher SpO2 in MAR results from ventilatory acclimatization. 6 A brisk hypoxic ventilatory response is critical during exercise at altitude because it limits the drop in SpO2 and contributes to a left shift of the oxyhemoglobin dissociation curve through induced respiratory alkalosis. Nevertheless, pulmonary limitations affecting SpO2 are still evident in people exercising at moderately high altitudes (3000–5000 m). In particular, during high-intensity exercise at altitude, hypoxia-induced pulmonary vasoconstriction impairs the ventilation-perfusion ratio, and interstitial pulmonary edema can develop. 10 Both can worsen SpO2.
Despite the knowledge of the protective effect of residence at moderate compared with low altitude, few studies have focused on the topic. In all but one, SpO2 was measured at rest. In the only article in which SpO2 was measured during exercise, it was measured at the third day of residence at 4300 m when acclimatization had already started. 7
We have shown that MAR maintain a significantly higher SpO2 during a fast ascent to 4559 m and have a low incidence of AMS. In particular, no MAR experienced moderate to severe AMS, whereas 8/33 LAR did experience AMS on arrival at higher altitude. Because we have no data on ventilation, pulmonary artery pressure, or the presence of interstitial pulmonary edema, we cannot know what might be the prevailing mechanism in maintaining better oxygenation during exercise above 3600 m.
Because SpO2 was predominantly different during exercise, we analyzed HR as a marker of exercise intensity between the 2 groups. In fact, if the approach to climb had been slower in MAR, cardiac output would be lower, resulting in less pulmonary diffusion limitation and higher SpO2. According to the available data, we propose that the higher SpO2 observed in MAR is not due to lower exercise intensity. In fact, HR during exercise was similar in the 2 groups.
The mean difference in SpO2 between the 2 groups during ascent to the highest altitude was 3.6±1%. This represents a lower degree of hypoxic stress. If we consider that the average decline in SpO2 from 1154 m to 3647 m amounts to 3.5 to 4% per 1000 m, then it is as if MAR were at an altitude of at least 800 m lower, which is an advantage. 8
Limitations
The first limitation of this study is the small number of MAR and the variable ascent profile that does not allow the authors to draw firm conclusions. A further limitation is the lack of detailed investigation of physiologic mechanisms influencing SpO2. As such, we cannot identify the reason why differences in SpO2 may exist between MAR and LAR during exercise at high altitude. It should also be noted that the presence of 2 alpine guides among the MAR could have affected the results if they had climbed many times at higher altitudes during the previous weeks. However, this was not the case because we performed the study at the beginning of climbing season (late June to mid-July) and only 1 guide had climbed to 4559 m 6 weeks previously without overnight stay. Furthermore, alpine guides can be a self-selected group not only in relation to the hypoxic stressor but also to strenuous exercise and fatigue. However, also most recreational climbers planning the ascent to the Regina Margherita Hut without pharmacological prophylaxis can be a similarly self-selected group. Regarding hypoxic pre-exposure, neither MAR nor LAR followed a true preacclimatization, but both groups included subjects who had already spent some days above 2200 m. This is not unusual for subjects intending to climb Mt. Rosa. Therefore, we do not believe that these differences significantly affected the results.
Conclusion
This is a preliminary study performed on a small sample of subjects. The results seem to suggest that acclimatization developed during residence at moderate altitude allows maintenance of higher SpO2 during rapid ascent to higher altitude. This reduces the risk of developing AMS. Further research in this area is needed to confirm the results. For example, the study could be repeated with a larger number of subjects, all following the same ascent profile.
Author Contributions: Study concept and design (LP, GM, AC); acquisition of the data (EB, LP, GM); analysis of the data (EB, LP, GM, DC); drafting of the manuscript (EB); critical revision of the manuscript (AC); and approval of final manuscript (AC).
Financial/Material Support: None.
Disclosure Statement: None.
Footnotes
Submitted for publication May 2016. Accepted for publication February 2017.