
Abstract
Objective
The purpose of this trial was to establish whether changes in resting oxygen saturation (Sp
Methods
A prospective trial was conducted on Jade Mountain, Taiwan from October 18 to October 27, 2008. Resting oxygen saturation (Sp
Results
Subjects who developed AMS had significantly lower Sp
Conclusions
Subjects with AMS had a lower Sp
Introduction
Acute mountain sickness (AMS) is a pathophysiological symptom complex that occurs in high altitude. Although it is benign in nature, AMS may be associated with the development of high altitude cerebral edema and high altitude pulmonary edema. The availability of transportation has allowed increasing numbers of travelers to visit high altitude areas. 1 However, the convenience of transportation allows for rapid ascent to altitudes that can compromise acclimatization and expose inexperienced climbers to the hazards of high altitude. High altitude illnesses have accounted for 33% of mountain rescues in Yu-Shan National Park (YSNP). 2 Between April 2007 and March 2008, a prospective, observational study was conducted at Paiyun Lodge on Jade Mountain that reported the prevalence of AMS to be 36%. 3 Jade Mountain is the highest peak in Taiwan at 3952 m above sea level. Most trekkers arrive at the park entrance (elevation, 2600 m) by car. From sea level this trip takes approximately 4 hours. A typical ascent of Jade Mountain normally involves an overnight stay at Paiyun Lodge (8.5 km from the entrance; elevation, 3402 m) before climbing a further 2.5 km to the summit (11 km from the entrance; elevation, 3952 m). 4
An effective means of predicting AMS remains elusive.
3
Studies using simple physiological measurements to predict AMS have shown promise in some studies,3,5 but others have shown that these measurements have a number of limitations.
6
–8 It has been suggested that oxygen saturation (Sp
Materials and Methods
Study Design and Setting
A prospective observational trial was conducted on Jade Mountain, Taiwan, from October 18 to October 27, 2008. A total of 1132 subjects were asked to participate in the study at the trail entrance; a total of 888 agreed to participate. All measurements were taken at rest. Heart rate and Sp
Participants
To be included in the trial, trekkers needed to stay overnight in the Paiyun Lodge on day 1 and reach the summit on day 2. Trekkers were excluded if they used Diamox (acetazolamide), suffered injury during the ascent, or failed to reach either Paiyun Lodge or the summit. Worth noting, trekkers were allowed to use other AMS prophylaxis, and were not restricted by age or medical history. Informed consent was obtained from all subjects, as reviewed and approved by the Institutional Review Board at Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Tao-Yun, Taiwan.
Statistical Analysis
Subjects diagnosed with AMS were compared with those without AMS (non-AMS) using independent 2-sample Student's t tests for continuous variables and χ2 or Fisher's exact test for categorical variables. Continuous variables were represented as mean ± standard deviation (SD), and number (n) and percentage (%) represented categorical data. To establish a predictive model of AMS development, all patients were randomly classified into a hypothesis-testing group or validation group (7:3 ratio) by using the random number generator provided with SPSS 18.0 statistical software (SPSS Inc, Chicago, IL). 12 Statistical comparisons between the hypothesis-testing group and validation group were performed to confirm that no significant differences existed between the 2 randomly allocated groups. The hypothesis-testing group was used to build models, and the validation group was used for model validation. Multivariate logistic regression analysis using a conditional forward stepwise selection method was performed to analyze the odds ratio (OR) of significant parameters associated with subjects who developed AMS. Furthermore, a receiver operating characteristic curve was used in the hypothesis-testing group to obtain the area under the curve (AUC), sensitivity, and specificity. All statistical assessments were two-sided, and a probability value of less than .05 was considered significant. Statistical analyses were performed using SPSS.
Results
A total of 888 questionnaires were collected, and 787 were considered appropriate for further analysis; 101 questionnaires were excluded because they were incomplete (n = 47) or the study criteria were not met (n = 54). Almost two thirds of the subjects were men (522 men and 265 women), with an average age of 42 ± 11 years (range, 9 to 80 years). Of those, 258 (33%) subjects were diagnosed with AMS.
Demographic characteristics, past high altitude mountaineering experience, and the medical history for subjects in the AMS and non-AMS groups are presented in Table 1. Overall, subjects with AMS were significantly younger (P < .001) and reported less high altitude mountaineering experience than those without AMS; specifically, the number of high altitude (>3000 m) mountains climbed (P = .001) and the number of high altitude (>3000 m) mountaineering climbs (P < .001), and high altitude (>3000 m) travel in the last 3 months (P = .024) were significantly different between groups. Smoking, alcohol use, heart disease, and hypertension were not significantly different between groups.
Demographic characteristics, mountaineering experience, and medical history of subjects with and without acute mountain sickness
All numbers are mean ± standard deviation unless otherwise specified.
AMS, acute mountain sickness; BMI, body mass index.
Probability values based on independent 2-sample Student's t test.
Probability values based on χ2 test.
Significant difference between AMS and non-AMS groups.
Sp
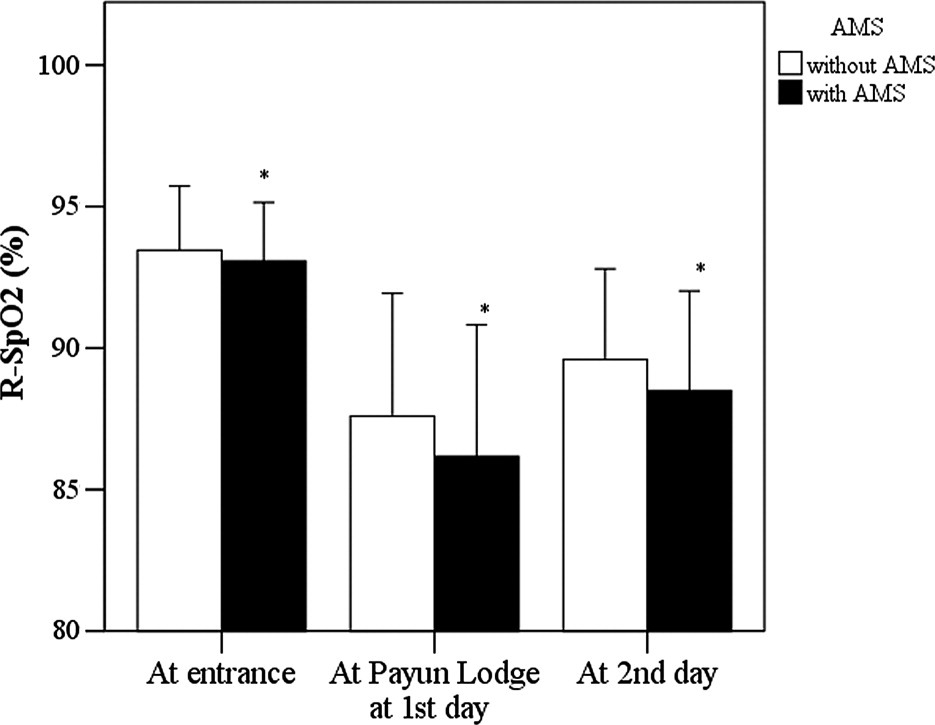
Resting oxygen saturation (R-Sp
No significant difference in HR between the 2 groups was observed (P > .05, data not shown). The change of Sp
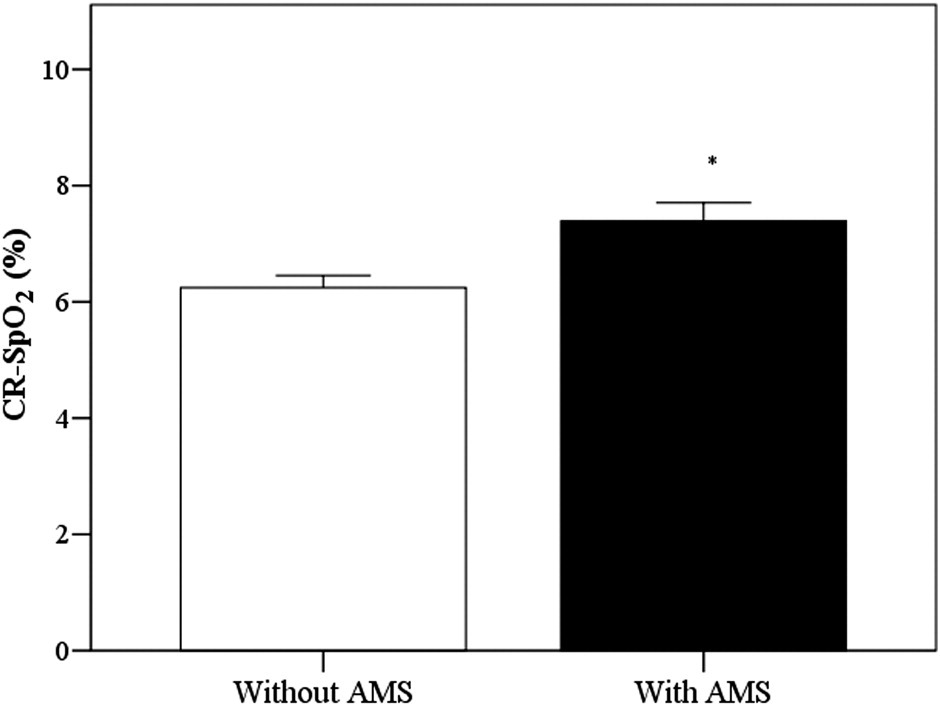
Change of resting oxygen saturation (CR-Sp
When stratified by symptoms associated with AMS, reports of fatigue or weakness, dizziness/lightheadedness, and difficulty sleeping in the AMS group were associated with significantly higher C-Sp
Change of resting oxygen saturation between subjects with and without acute mountain sickness stratified by symptoms commonly associated with altitude sickness
All numbers are mean ± standard deviation.
AMS, acute mountain sickness; CR-Sp
P < .05, significant difference between AMS and non-AMS groups using independent 2-sample Student's t test.
To establish a predictive model of development of AMS, all subjects were randomly assigned into a hypothesis-testing group (n = 552) or validation group (n = 235). There were no statistically significant differences in subjects' characteristics between the hypothesis-testing group and the validation group (Table 3). High CR-Sp
Demographic characteristics, mountaineering experience, and medical history between groups
All numbers are mean ± standard deviation unless otherwise specified.
AMS, acute mountain sickness; BMI, body mass index.
Probability values based on independent 2-sample Student's t test.
Probability values based on χ2 test.
The AUC was 0.59 (P < .001; 95% CI, 0.54 to 0.65). A C-Sp
Discussion
The current investigation reports that trekkers on Jade Mountain, Taiwan, diagnosed with AMS had a lower Sp
An observation in this study is that change in resting oxygen saturation (C-Sp
Our results are in agreement with the data that have been reported in previous publications, which demonstrate that reliable prediction of who is susceptible to AMS based on measurements of Sp
Potential predictors of AMS have been reported in the literature, including high altitude trekking experience or preexposure, history of AMS, age, and ascent speed. 3 In the current study, trekkers with AMS were younger, had less high altitude mountain summiting, less high altitude mountain experience, and less high altitude preexposure (Table 1); these associations have been reported elsewhere. 5 Jade Mountain provides a unique opportunity for exposure to high altitude and rapid ascent to 2600 m. Transportation is available to take trekkers directly to the park entrance (2600 m). Because less experienced trekkers are able to reach what could be considered high altitude via car, possibly before acclimatization, safer, quicker, and more objective measurements are needed as a way to screen for susceptibility to AMS.
The Jade Mountain trail commonly attracts inexperienced trekkers compared with other trails in YSNP, and reports the highest rate of high altitude-related mountain illness in the time YSNP has been open. 2 Because AMS is often characterized by a delayed onset and most Jade Mountain trekkers developed AMS during the night at Paiyun Lodge, 3 it would be helpful to more clearly identify trekkers prone to developing AMS.
Limitations
The elevation of the entrance to the Jade Mountain trails is 2600 m—it is possible that some trekkers in this study had AMS soon after arrival. The data collection was concentrated only in October. There are several items to consider regarding the measurement of Sp
Conclusions
Subjects with AMS had a lower Sp
Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.
Footnotes
Acknowledgments
We thank Mr Jih-Ting Chen, Teacher of YunLin Elementary School, Mr Lung-Sheng Chen, Director of YSNP Administration; Mr Bagkall, Chief of Tourism and Recreation at YSNP; Mr Wu Wan-Chang, Chief of Paiyun Hiking Services Center; and Mr Wu Her-Jong, Chief of Conservation and Research at YSNP for their great help.
⁎
Hang-Cheng Chen and Wen-Ling Lin are co-first authors of this paper.