
Abstract
To provide guidance to the general public, clinicians, and avalanche professionals about best practices, the Wilderness Medical Society convened an expert panel to revise the evidence-based guidelines for the prevention, rescue, and resuscitation of avalanche and nonavalanche snow burial victims. The original panel authored the Wilderness Medical Society Practice Guidelines for Prevention and Management of Avalanche and Nonavalanche Snow Burial Accidents in 2017. A second panel was convened to update these guidelines and make recommendations based on quality of supporting evidence.
Introduction
Snow and ice avalanches are widespread in mountain regions. Worldwide avalanche-related morbidity and mortality are difficult to estimate because many countries lack reporting systems. Europe and North America have relatively accurate systems for capturing data on avalanche fatalities. Approximately 130 fatalities occur annually in Europe and 36 in North America.1-4 During the 31 winter seasons between 1983 and 2015, Europe and North America had 5123 avalanche fatalities. 5 Although internet databases exist for North America and some European countries, scholarly articles that document the number of fatalities have not been published. From 2002 to 2022, online databases showed a 20-y average of 36 avalanches in North America and 130 in Europe, according to email correspondence with Swiss avalanche expert Jürg Schweizer (January 10, 2022). In the United States, a partnership between the American Avalanche Association and the US Forest Service National Avalanche Center keeps statistics regarding avalanche fatalities at https://www.avalanche.org/avalanche-accidents. Avalanche Canada maintains statistics at https://www.avalanche.ca/incidents. European statistics for the Alps and Pyrenees are maintained by the European Avalanche Warning Services at https://www.avalanches.org/fatalities/fatalities-statistics.
Avalanche fatalities in mountain regions outside North America and Europe are not systematically recorded. Catastrophic avalanches with large death tolls have included the serac fall on Mount Everest in 2014 that killed 16 Sherpas; the earthquake-caused avalanche at Everest Base Camp in 2015 that killed 22; the serac collapse on the Marmolada Glacier, Italy, in 2022 that killed 7; the avalanche in Rigopiano, Italy, in 2017 that killed 29; the avalanche in Galtur, Austria in 1999 that killed 31; an avalanche in Turkey in 2020 that killed 42 motorists followed by a second avalanche that killed 33 rescuers; and an avalanche in 2012 that killed 148 Pakistani Army members in the Siachen Glacier region. 6 A reasonable estimate of annual global avalanche deaths is 300 to 500, based on media reports, websites, and other sources, according to email correspondence with American avalanche expert Dale Atkins (January 10, 2023). Nonfatal avalanche events are extremely difficult to quantify because many accidents are not reported.
Most documented North American and European avalanche fatalities are recreational users, such as snowmobilers, skiers, snowboarders, mountaineers, and snowshoers. Occupational-related avalanche fatalities among ski patrollers, mountain rescuers, mountain guides, and transportation workers occur less frequently, although job requirements may place these personnel at greater risk. 1
Avalanche avoidance should be the main method to mitigate risk of injury and death. If an avalanche incident occurs, rescue by one's companions, with appropriate resuscitation and advanced life support measures, is critically important to reduce avalanche morbidity and mortality. 7
Methods
The Wilderness Medical Society (WMS) convened an expert panel to develop evidence-based recommendations for 3 primary aspects of avalanche accidents: prevention, rescue, and resuscitation. We also included nonavalanche deep snow and tree well burial 8 as related conditions with pathophysiology and recommendations similar to avalanche burial. The Wilderness Medical Society Practice Guidelines for Prevention and Management of Avalanche and Nonavalanche Snow Burial Accidents were initially published in 2017. 9 A second panel convened upon request in 2022 to update the guidelines.
We searched the PubMed database for articles from 2016 to 2022 for keywords including avalanche rescue, avalanche burial, avalanche transceiver, avalanche location, avalanche search, avalanche shoveling, avalanche command, avalanche scene, avalanche probe, avalanche RECCO, avalanche dog, avalanche helicopter, deep snow burial, deep snow asphyxiation, deep snow suffocation, tree well asphyxia, tree well suffocation, tree well submersion, tree well immersion, deep snow submersion, deep snow immersion, and nonavalanche-related snow immersion death.
We considered peer-reviewed randomized controlled trials, observational studies, case series, and case reports for inclusion. Because a limited number of studies of avalanche accidents have been published in peer-reviewed journals, we also reviewed conference proceedings, avalanche center data, letters to the editor, review articles, websites, personal communication from experts, and books for background information.
We developed recommendations by consensus. We graded recommendations based on strength of the recommendation and quality of the evidence using the classification scheme of the American College of Chest Physicians (Supplemental Table). 10 When no evidence existed, we made recommendations based on expert consensus based on review articles, textbooks, clinical experience, rescue experience, and first-hand knowledge of equipment, techniques, and avalanches.
Pathophysiology
Avalanche morbidity and mortality depend mainly on the degree of head and chest burial, duration and depth of burial, patency of the airway, presence of and volume of an air pocket, snow density, and traumatic injuries. 11 The chance of survival after critical burial (head and chest below the snow) is about 50%.2-4,12 For victims not buried critically (head and chest out of the snow), the likelihood of survival is nearly 100% unless trauma is a contributing factor.2,12,13 Avalanche deaths are most frequently caused by asphyxia (75% of fatalities) and by trauma (25%).13-20 These percentages vary by region. Few deaths are caused solely by hypothermia. 15
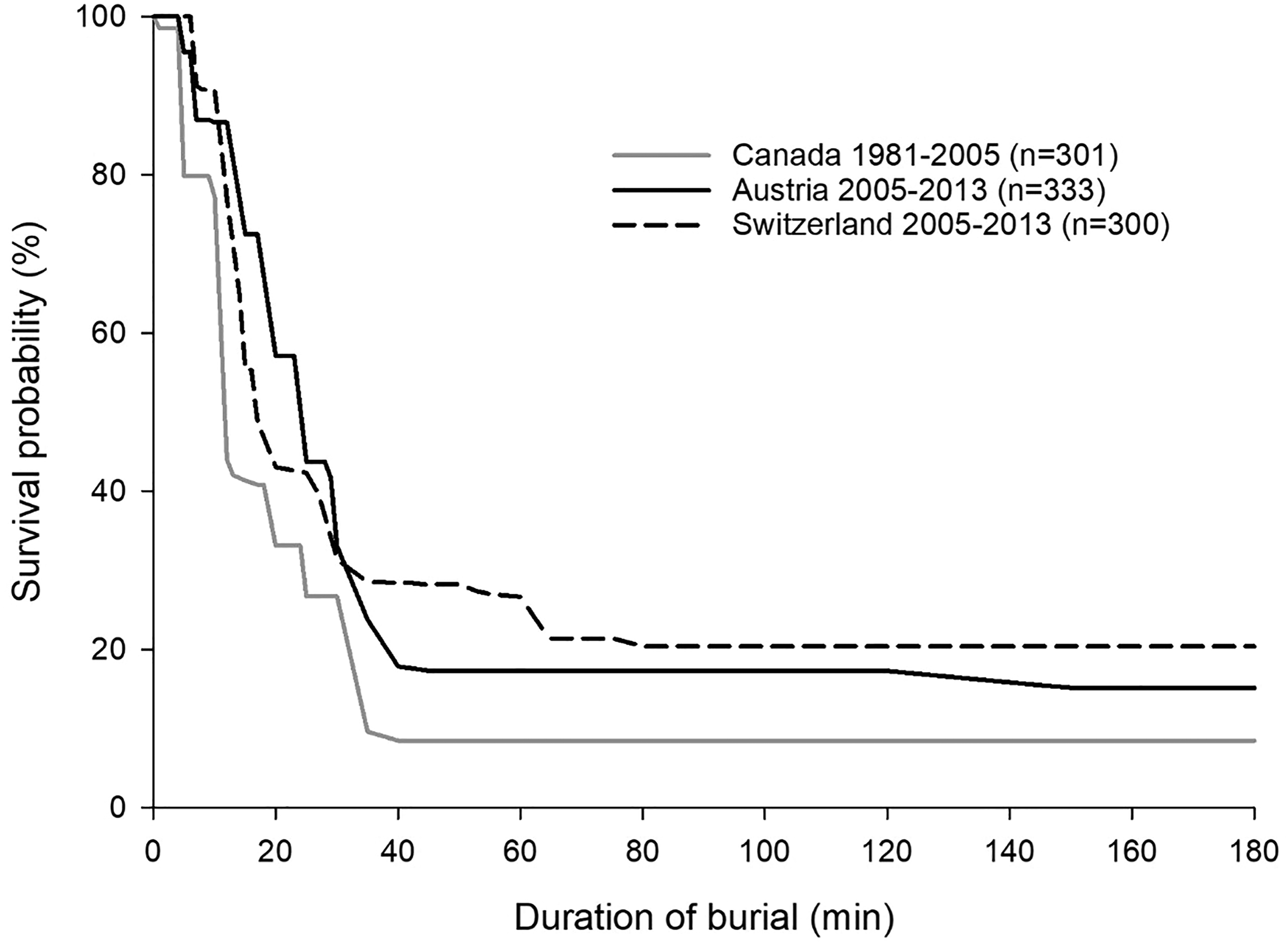
If an avalanche victim is critically buried, the time to extrication is the main determinant of survival. 21 Critically buried victims have greater than 90% chance of survival if extricated within about 15 min, but only a 30% chance of survival if extricated after approximately 30 min (Figure 1).21,22 Survival of a buried victim after more than 35 min requires a patent airway and the presence of an air pocket.2,23,24 A case report described a victim who survived 45 min with a patent airway but no air pocket with a poor neurologic outcome. 25 A victim can be found in almost any position. About 45% of buried avalanche victims are found lying prone, 24% supine, 16% sitting or standing, and 15% lying on their sides. 26 Mortality increases with increasing depth of burial.24,27
Asphyxia
Asphyxia (deprivation of oxygen) during avalanche burial occurs primarily by 3 mechanisms: 1) Complete or partial obstruction of the upper airway caused by inhaled snow or debris can result in hypoxia and hypercapnia within 10 min and cause death from asphyxia within 35 min of avalanche burial11,28-33; 2) High density snow or lack of an air pocket may not allow sufficient inflow of oxygen and removal of carbon dioxide (CO2) through the surrounding snow, leading to asphyxia from rebreathing expired air. 30 Inspired air contains 21% oxygen and less than 0.03% CO2. Expired air contains about 16% oxygen and 5% CO2. Rebreathing expired air during avalanche burial results in a progressive decrease in the fraction of inspired oxygen and a progressive increase in the fraction of inspired CO2, leading to hypoxia, hypercapnia, and increased ventilatory drive.30,32,34 Lack of an air pocket may also increase work of breathing and metabolic rate.13,24,35 Increased snow density and decreased porosity of snow surrounding the air pocket can decrease diffusion of gases30,32,36; and 3) The weight and compaction of snow may limit chest expansion and impair ventilation. 13
Case reports and human trials have demonstrated that long-term survival is possible without hypoxic brain damage if the buried victim is able to breathe under the snow. The presence of a patent airway and an air pocket (any space in front of mouth and nose) may enable a buried victim to breathe and to survive for far longer than with an obstructed airway or without an air pocket.3,13,14,22,24,31,32,37 Increasing the volume of an air pocket can increase the duration of survival after burial. 32 If the density of the surrounding snow is low enough to allow sufficient diffusion of oxygen into the air pocket from the snowpack and diffusion of expired CO2 into the snowpack, a buried victim may survive for several hours.30,33,38,39 If snow density is high (>350 kg m−3), hypoxia and hypercapnia will occur more quickly. 30 High-density snow is more common in maritime climates and during spring conditions. With climate change, wetter and warmer climates are likely to have higher density snow.3,40
Delayed onset of acute respiratory distress syndrome has been reported in avalanche victims after burials as short as 5 min and as long 207 min. This may be noncardiogenic pulmonary edema, triggered by high negative intrathoracic pressures from upper airway obstruction, aspiration, or pulmonary contusion.41-45
Trauma
Trauma accounts for 6 to 29% of avalanche deaths in North America and Europe.12,14,15,18,19,34,46,47 In catastrophic avalanches and in summer avalanches, trauma often accounts for a higher percentage of fatalities.48-50 The proportion of avalanche deaths associated with trauma in Canada is higher than in Europe and the United States.3,20,51,52 Traumatic injuries may become more frequent with climate change. 40
Avalanche victims can sustain any type of injury during turbulent descent in an avalanche.18,47 Severe injuries are frequently the result of collisions with trees or rocks or from falls off cliffs. Minor injuries are likely to be unreported. Injuries of the head, cervical spine, chest, and extremities are the most common life-threatening injuries.12,16,18,20,51 In a study of avalanche victims with trauma, the majority had evidence of traumatic brain injury. Altered level of consciousness and chest injury may further decrease survival by accelerating asphyxiation.53,54
Hypothermia
Hypothermia causes few fatalities in avalanche victims because death from asphyxia usually occurs sooner.2,32,54-56 The severity of hypothermia is best determined by core temperature measurement in the field.57-59 If core temperature cannot be measured, the stage of hypothermia can be estimated in the field as mild, moderate, or severe, using the WMS Accidental Hypothermia guidelines. 58 The Revised Swiss System (RSS) can also be used. 60 Both the WMS and RSS staging may be inaccurate if there is associated trauma or asphyxia contributing to a decreased level of consciousness.19,37,43,61-63
Reported cooling rates of critically buried avalanche victims vary widely from 0.1°C h−1 to 9°C h−1, but are typically 1°C h−1 to 3°C h−1.19,37,38,62,63 At least 1 h of avalanche burial is usually required to reach a core temperature <30°C, at which fatal arrythmias become more likely. 64 In human simulations of avalanche burials, hypercapnia caused a 70% increase in cooling rates.37,61 Core temperature cooling rate increases during and after extrication from snow burial because of exposure to the air, removal from the insulation of snow, and vasodilation of the extremities if the victim stands or walks.61,65,66
Prevention
Prevention of avalanche morbidity and mortality depends on avoiding being caught in an avalanche, avoiding being critically buried, preventing trauma if caught, and avoiding asphyxiation if buried. The primary goal of education is to teach how to avoid avalanche accidents. Public safety measures for prevention and mitigation of avalanche accidents, such as the use of explosives, barriers, snow fences, deflectors, and snow sheds across roads, are beyond the scope of these guidelines.
Avalanche Avoidance
In the majority of avalanche accidents, the victim or someone in the victim's party triggered the avalanche. 67 Avalanche risk can be decreased by avoiding hazardous terrain, snow, and weather conditions and by taking group dynamics and human factors into account. A detailed discussion of decision-making and selecting safe routes in avalanche terrain is beyond the scope of these guidelines.
Education and experience are cornerstones of risk mitigation.7,68 Some techniques used to avoid avalanches include avoiding slopes >30 degrees, traveling on ridges, traveling in thickly forested terrain, and avoiding travel in avalanche terrain during high-hazard conditions, such as during and immediately after heavy snowfall, especially with significant wind, and during rapidly increasing temperatures.69,70 Avalanche education can help prevent accidents, including avalanche safety courses, textbooks, videos, and local avalanche advisories.69-71
Decision aids can facilitate assessment of avalanche hazards, reducing misleading human factors.72-76 Although it can be difficult to measure their impact, decision aids can be effective in recreational settings.77-79 In addition to education, training, and the use of decision aids, good judgment and regular training with safety equipment are vital to avalanche safety.
In a large Italian study (n=5576), adherence to minimum safety procedures, such as carrying personal rescue equipment, was less than 42%. Adherence was significantly greater for skiers than for snowshoers and greater in people who were younger, reported more tours per season, traveled in larger groups, and started earlier in the day. 57
Recommendations
We recommend travelers in avalanche terrain attend training courses through accredited organizations, supplemented by educational books and videos, avalanche advisories, and decision aids. We recommend travelers in avalanche terrain regularly practice safety and rescue skills. Strong recommendation, low quality evidence.
Burial Avoidance
Physical Maneuvers
When entering a high-risk avalanche path for rescue or avalanche control work, use of a belay line, securely anchored outside the path, can prevent an individual from being swept downslope by an avalanche.70,80 Travelers should cross dangerous slopes one at a time, while being watched by a partner, and should move between safer areas such as rock outcroppings, tree clusters, or safer adjacent slopes. Planning an escape route before entering an avalanche-prone area can increase the likelihood of avoiding being caught in an avalanche. Avalanche professionals commonly use slope-cutting techniques in which one person rapidly traverses a potentially unstable slope from one safe zone to another to test stability. This technique may trigger an avalanche, possibly reducing avalanche hazard because the slope is less likely to slide again.70,80
A person about to be caught in an avalanche should immediately attempt to escape to adjacent terrain outside the avalanche. When descending suspect slopes, a traveler should maintain a speed at which momentum has a chance to carry them off the moving snow to a preplanned safety zone. This may reduce the odds of being caught and buried but requires expert skill.
The next priority, if unable to escape sliding snow, is to avoid burial. One should attempt to remain on the surface and fight to move toward the starting zone of the avalanche where the flow is less turbulent. It may be possible to self-arrest by anchoring into the bed surface with a ski pole or ice ax. 81 One may be able to grab a tree or rock. Some experts recommend swimming motions to stay on the surface. While this practice has been challenged, 81 case studies and theoretical considerations regarding the flow of avalanches support using any type of motion to stay at or near the top of the debris flow. 46
A victim on skis, snowboard, or snowshoes will likely be buried deeper than a victim without impediments. Extrication will likely be more difficult. Kicking off skis or removing a snowboard may improve the likelihood of survival. Victims should not remove backpacks. A backpack might provide protection from trauma. Equipment in the backpack may be necessary for survival.
Recommendations
We recommend that if caught in an avalanche, immediately attempt to escape the moving snow, or, if engulfed, use any motion possible to avoid critical burial. Strong recommendation, low quality evidence.
Recommendation
We suggest if caught in avalanche and unable to escape, attempt to jettison skis or a snowboard but do not remove a backpack. Ungraded: Expert consensus.
Avalanche Airbags
Avalanche airbags are the only avalanche safety devices that can prevent burial. 4 Airbags are backpacks or vests that contain 1 or 2 balloons. When caught in an avalanche, the user manually deploys the balloon by pulling a handle and inflating the balloon(s) to a total volume of about 150 L. Airbags use 1 or 2 cylinders of compressed gas or a battery-powered fan to inflate the balloon(s). A deployed airbag increases the effective volume of an avalanche victim, taking advantage of the physical process of granular convection. In a flow of various-sized particles, larger particles are sorted toward the surface.48,52,82 Increased effective volume reduces the chance of deep or complete burials.
Use of avalanche airbags is supported by simulations and epidemiologic studies. Trials with intentionally-triggered avalanches and crash test dummies showed that dummies with an inflated airbag had a lower probability of burial.83-85 Statistical evaluations of accidents have compared the mortality rates of avalanche victims with and without airbags.4,86,87 In a retrospective analysis of avalanche accident records from Europe and North America, 22 inflated airbags reduced mortality from 22% to 11%. This study also found that noninflation was a problem with the use of airbags. The noninflation rate from all causes was 20%. Overall mortality for airbag users was 13%.
In another study, dummies with and without airbags were deployed into artificially triggered avalanches. Of the dummies without airbags, the mean burial was 42 cm (range 25−63 cm) and visibility on debris surface was 20% (1/5 dummies). Of the dummies with airbags, the mean burial was 15 cm (18−26) and visibility was 100% (14/14). 88
Operator error is the most important limitation of airbags, with 60% of noninflations attributable to the user failing to trigger the airbag. Other obstacles to use of airbags include cost, weight, and regulations limiting most compressed gas canisters on commercial airplanes. Airbags are also ineffective if a victim is swept off a cliff or into thick trees, where trauma is a greater risk than asphyxia. Death from asphyxia can occur despite airbag deployment in deep burials, if a second avalanche causes a critical burial, or if the airbag is destroyed by the avalanche.
There are no safety or survival data comparing airbags inflated by different systems. Airbags with fans have the advantage that users can practice or use the devices in the field multiple times. Fan airbags are allowed on commercial airplanes. Canister-actuated airbags require additional canisters for practice or for multiple deployments in the field. Most canisters are not allowed on commercial airplanes. Canister airbags are generally less expensive than fan-actuated airbags.
Travelers have been slow to adopt airbags, possibly because they are expensive, heavy, and bulky. 89 In the Italian study of 5576 skiers and snowshoers, less than 4% were carrying an airbag. 57 At least one manufacturer makes a backpack with both an airbag and an artificial air pocket device.
Recommendations
We recommend that travelers entering avalanche terrain should use airbags. Familiarity and regular practice with airbags are essential. Strong recommendation, moderate quality evidence.
Trauma Prevention
Helmets
A retrospective review of autopsies of avalanche victims in Utah suggested that traumatic brain injury contributed to death from asphyxia. 90 Helmets can prevent minor and major trauma in resort skiers and snowboarders. 91 Helmets are less effective at preventing morbidity and mortality in avalanches, but there is little downside to their use. 92 There are no studies on the effectiveness of helmets in reducing death from head trauma in avalanche accidents. Velocities of medium and large avalanches may exceed the protective capabilities of helmets designed for recreational skiing and climbing, 92 but most recreational fatalities are in small- to medium-sized avalanches with lower velocities in which helmets might prevent or ameliorate traumatic brain injuries. 67 Helmets may also help to prevent lacerations, minor head injuries, and hypothermia.
Recommendations
We recommend helmets should be worn when traveling in avalanche terrain. Strong recommendation, low quality evidence.
Avalanche Airbags
Some models of avalanche airbags surround the head and neck once deployed. Generally, these are backpacks with single airbags in a “U” shape. They may help to prevent or mitigate injuries from an avalanche or from collisions with objects in the avalanche. Although there are theoretical benefits, there are no data on the use of airbags to reduce the risk of head and neck trauma.
Recommendations
We suggest airbag backpacks may provide head and neck protection from trauma. Ungraded: expert consensus.
Asphyxia Avoidance if Buried
Physical Maneuvers
An unobstructed airway and an air pocket are critical for surviving avalanche burial, but turbulence often forces snow into the mouth and nose of a victim. One technique for protecting the airway during an avalanche is to reach across the face with one arm, holding the crook of the elbow over the mouth. 80 This may help decrease the amount of inhaled snow, protect against facial trauma, and create an air pocket.
Recommendations
We recommend if caught in an avalanche, a victim should attempt to protect the airway and create an air pocket by reaching across the face with one arm, holding the crook of the elbow over the mouth. Strong recommendation, low quality evidence.
Avalanche Airbags
Some airbags deflate automatically, 3 min after deployment, to create an air pocket. A study that buried 12 subjects, monitoring vital signs for 1 h, tested the hypothesis that an air pocket could prolong survival. 91 Eleven subjects maintained normal vital signs for 60 min, while 1 subject maintained normal vital signs for 49 min before requiring extrication with increasing heart rate, increasing end-tidal carbon dioxide (EtCO2), and anxiety.
Recommendations
We recommend that an airbag that deflates after burial may help prevent asphyxia by creating an air pocket. Strong recommendation, low quality evidence.
Air Diverters
Air diverters are intended to enable critically buried avalanche victims to channel exhaled CO2 away from the airway, thus separating carbon-dioxide-rich exhaled air from oxygen-rich inhaled air. The system also diverts moisture-rich air, delaying formation of ice on the surface of the snow in an air pocket that can interfere with gas exchange. The device consists of a mouthpiece that connects to tubing with a one-way inspiratory valve and a one-way expiratory valve. Inspired air enters from the front of the user, via an intake port. Expired air is diverted to the back of the user via an exhaust port. In addition to delaying asphyxia caused by rebreathing CO2, the mouthpiece may help keep the airway free of snow.
In a randomized, crossover-controlled trial, in simulated avalanche debris, breathing with an air diverter allowed adequate oxygenation for up to 60 min. 35 In the control group, participants breathing directly into a 500 mL air pocket experienced hypoxemia in 5 to 14 min. There have been many any cases of survival with the use of air diverters.92,93 There has been no study comparing the mortality of users and nonusers. Currently, air diverters are commercially available in Europe but not in North America. In the Italian study, less than 0.5% of 5576 skiers and snowshoers carried an air diverter. 57
Recommendations
We recommend that a traveler entering avalanche terrain should consider using an air diverter. Strong recommendation, low quality evidence.
Rescue
Avalanche rescue can be accomplished by companions or professionals. A systematic approach to avalanche rescue maximizes the efficiency and effectiveness of rescuers. 94
Avalanche Rescue Sequence
A rescue sequence (Figure 2) can be adapted to avalanche rescue regardless of the number of victims or rescue personnel. In a small team, a single individual may be responsible for multiple tasks. In a large team, each role may be assigned to a different rescuer. Some steps may be completed simultaneously. The team should immediately establish leadership. The leader should assess the scene for hazards, formulate a rescue plan, manage available resources, and continuously assess scene safety. If possible, at least 1 person, should be stationed at a vantage point that allows a view of the entire scene.
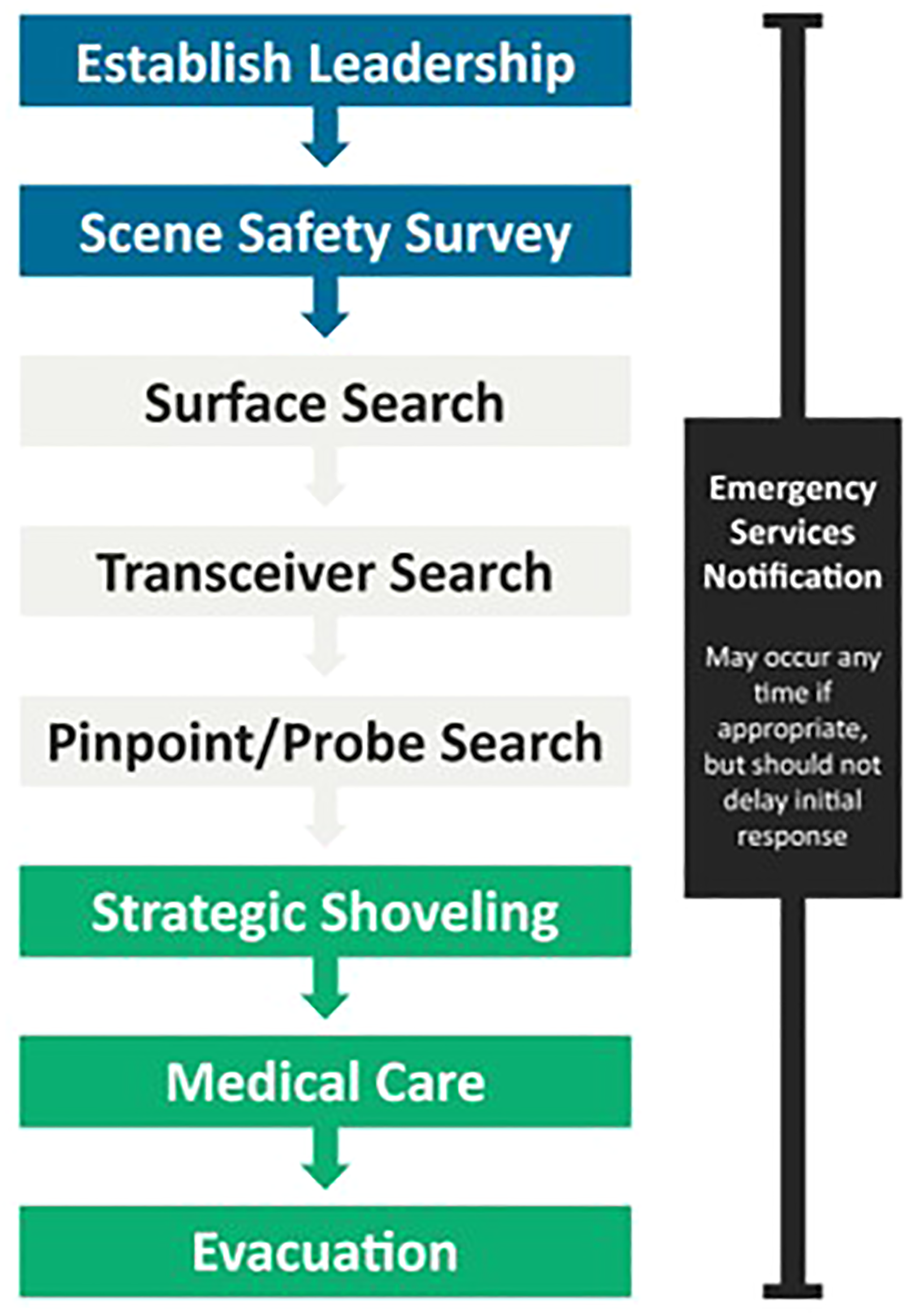
Avalanche rescue algorithm.
The surface search for visible clues should occur simultaneously with the transceiver search, especially with small groups. The surface search should begin at the last-seen point from above or at the bottom edge of the debris from below. The last-seen point should be identified with a physical marker such as a ski pole or avalanche probe.
In addition to the surface search, methods of locating a buried victim are transceiver searches (coarse and fine), pinpoint searches (probe searches), and shoveling to extricate the victim. A manikin study simulating avalanche rescue found that it takes an average of 7 min to free the airway after locating a simulated avalanche victim buried in a supine position at a depth of 1 m. It takes an additional 3 min to start cardiopulmonary resuscitation (CPR). 95 One rescuer tended to be slower than 2 rescuers (10.5±SD min vs 9.3±SD min). The position of the manikin did not impact recovery speed (10.8±SD min with head downhill in prone position; 10.6±SD min with head uphill in prone position; and 8.8 min with head uphill supine). Previous training improved rescue times: 6.1 min vs 11.0 min (P=0.006). 97 A major limitation was that the simulated avalanche debris had a lower density than actual avalanche debris. 96
A retrospective study of 205 fatalities of backcountry skiers and snowboarders, side country (lift-served backcountry) skiers and snowboarders, snowmobilers, and snow bikers concluded that, on average, snowmobilers were buried deepest. Solo travelers had the longest burials. Skiers and snowboarders had the highest proportion of short burials (<15 min). Backcountry skiers and snowboarders were most likely to have avalanche rescue equipment. 7 In the Italian study of 5576 skiers, snowshoers, and snowboarders, a larger percentage of skiers (81%) than snowshoers (14%) carried personal rescue equipment (transceiver, probe, and shovel). 57 On days with low avalanche hazard, travelers are less likely to carry avalanche safety gear. 98
If an avalanche accident requires additional rescue or medical assistance, local emergency services should be notified, but notification should not delay the initial rescue response. 99 Additional time is required to turn on a phone, acquire a signal, and report an accident.
In a Swiss study of 3892 avalanche victims, avalanche burial at night was rare (<2%), but mortality was greater than daytime burial. 100 Survival was highest with burial at midday (63%), followed by sunset (40%), and lowest at midnight (29%). Reasons for declining survival may include longer search for completely buried victims (89 min vs 20 min), lower rates of companion rescue (15% vs 51%), and lower rates of locating victims using avalanche transceivers. 100
Recommendations
We suggest that after an avalanche accident, rescuers should establish leadership; secure the scene; perform surface, transceiver, and pinpoint searches; shovel strategically; and notify emergency services when appropriate. Ungraded: Expert consensus.
Transceiver Search
Avalanche transceivers decrease morbidity and mortality when used by both victims and rescuers. Transceivers reduce the time between critical burial and rescue, from 102 min to 20 min in one study. However, mortality of critically buried victims was only decreased from about 68% to about 54%. 101
Electronic devices, such as mobile phones, portable radios, global positioning system (GPS), and other digital communication devices, may interfere with avalanche transceiver searches because similar radio frequencies are susceptible to electromagnetic interference. 102 Medical devices, such as cardiac pacemakers, implanted defibrillators, and insulin pumps, can also interfere with transceivers. 103 It is not yet known whether electronic battery-operated fan airbags interfere with transceivers. To minimize interference, transceivers in transmit mode should be kept at least 20 cm away from other electronics and 50 cm away in search (receive) mode.96,104,105
Current transceivers have 3 internal antennas and use digital processing. Some transceivers provide audible as well as visual signals to help identify search direction and the depth of the victim. 106
Recommendations
We recommend all travelers in avalanche terrain should carry an up-to-date avalanche transceiver, know how to perform effective searches, and practice regularly. Strong recommendation, moderate quality evidence.
Recommendation
We recommend that rescuers should keep transceivers in transmit mode a minimum of 20 cm from other electronics and metal objects, with a minimum of 50 cm in search mode. Strong recommendation, moderate quality evidence.
Other Location Devices
Telecommunication devices other than avalanche transceivers are not useful for avalanche rescue. Global positioning system transceivers are ineffective because the signal is not sufficiently precise.107,108 Personal locator beacons have not been studied, but they rely on GPS technology and are not designed for companion rescue.
Cell phones, satellite phones, and hand-held very high frequency/ultra high frequency (VHF/UHF) radios can aid in summoning help but are not useful for searching. Cell phone avalanche applications cannot be used to locate a buried victim in a reasonable amount of time. 109
Recommendations
We suggest that GPS transceivers, cell phones, satellite phones, and VHF/UHF radios are not recommended for locating a buried avalanche victim during companion rescue. Weak recommendation, low quality evidence.
Pinpoint Search
A probe can be critical for finding a buried victim. A 2.5- to 3-m probe is standard. 110 A 2-m probe might be adequate because most avalanche victims who are found are buried within 1.5 m of the surface.111,112 The main advantage of the shorter length is to save weight and space in a backpack.
After a rescuer has used an avalanche transceiver to find the closest signal of the buried beacon to the snow surface, rescuers should probe, systematically inserting the probe perpendicular to the snow. A concentric circular method is most efficient, beginning at the location of the closest transceiver reading. Probe holes should be 25 cm apart.113,114 Rescuers should feel for inconsistencies within the snowpack and monitor changes in the depth at which the probe stops. Whenever there is a possible strike, the probe should be left in place as a target for shoveling.
Recommendations
We recommend that all travelers in avalanche terrain should carry and know how to use a 2.5- to 3-m collapsible probe for pinpoint searching. Probing should be perpendicular to the surface in a concentric circular pattern with probe holes 25 cm apart. Strong recommendation, low quality evidence.
Strategic Shoveling
A shovel is essential to extricate a buried victim. Metal shovel blades are more durable than composite blades. 115 Efficient shoveling techniques are critical for minimizing extrication time to increase survival. 112 In a simulation with loose snow (density 651±8 kg/m-3), using a scooped shovel, the amount of snow cleared increased 47% compared to a flat shovel. 116 Men moved 44% more snow per unit time than women. 116 Shoveling should begin downhill at least 1.5 times the distance of burial depth, based on the probe strike or best estimated location. A working platform the width of a body, level with the buried victim, will help conserve rescuer energy. The shovel can be used like a paddle to scrape or plow snow downhill. Initially, rescuers move to the sides of the pit, leaving the middle for snow from deeper in the pit. No studies have investigated the difference between a shovel handle in line with or perpendicular to the blade.
When multiple rescuers are available to shovel, a conveyor belt method may be used,117,118 with rescuers rapidly paddling snow downhill in succession, usually fanning the snow to the sides to eliminate excess snow buildup. Rescuers should rotate positions frequently, typically every few minutes, to prevent fatigue. They should excavate a wide, flat platform for the extricated victim to aid in resuscitation and packaging for transport. In a simulated avalanche study with manikins, 1 or 2 rescuers required approximately 10 min to locate, excavate the manikin from 1 m below the surface and initiate CPR. 97 In real avalanche burials, the time required is likely to be much longer because of psychological and technical demands and higher snow densities of avalanche debris.
Recommendations
We recommend that all travelers in avalanche terrain should carry and know how to use a scooped metal shovel designed for avalanche debris. We suggest shoveling techniques should include using the shovel like a paddle to plow snow downhill. We suggest a conveyor system should be used if multiple rescuers are available. Strong recommendation, low quality evidence.
Professional Rescue
Organized rescue groups may include mountain guides, volunteers, or professionals such as ski patrollers. Professional rescue differs from companion rescue because the response time is typically longer, resources are more plentiful, and group size is larger. Because an organized group takes longer to mobilize than the usual 30 min for a victim to asphyxiate, the incidence of live recovery in organized rescue response is low.1,119
Incident Command System
The Incident Command System (ICS) or a similar system should be used to establish a standardized approach to emergency response for avalanche rescue.120-122
Recommendations
We recommend that all members of organized rescue groups should receive training in ICS or a similar system in avalanche rescue. Strong recommendation, low quality evidence.
Scene Management
Scene management becomes increasingly important as more rescuers and resources become involved in an avalanche response. Effective scene management can reduce false positive signals from well-intentioned bystanders wearing transceivers in transmit mode and can facilitate effective search of an avalanche path while minimizing missed clues or areas. The boundaries of the avalanche path should be marked to keep unauthorized people from introducing erroneous clues and to ensure that rescuers have a clear view of the avalanche site. The entry and exit tracks, the last-seen point, visible clues, and probe locations should be marked with physical markers such as climbing wands, ice axes, skis, ski poles, or backpacks. 123
Recommendations
We recommend active scene management techniques such as boundary control and scene marking should be used. Ungraded: Expert consensus.
Probe Line
For buried victims without transceivers, a probe line should be established. In a professional rescue team, a leader should maximize probe line efficiency to increase the likelihood of recovering a live victim.
The initial probe depth should be 1.5 m to maximize efficiency. This would reach 88% of victims recovered alive in the United States and 95% of victims recovered alive in Switzerland. 111
The probe technique should follow the 3-holes-per-step method, which is 30% faster than standard coarse probing. 111 The rescuer inserts the probe into the snow 3 times while standing: 20 cm to the rescuer's left, center, and 20 cm to the rescuer's right. The rescuer then takes a step forward and repeats the process.
In slalom probing, organized rescuers probe 3 areas in a left-to-right pattern 50 cm apart while walking in zig-zags in the avalanche debris. The width of the zig-zags and the size of the search area depend on the number of rescuers. 124 Slalom probing covers the same surface area faster than the 3-holes-per-step method but may be less effective.
Probe line grid spacing influences the probability of detection. A small grid has a greater chance of finding a buried victim but may cause the probe line to move slowly. A large grid may allow rescuers to miss a buried victim. A 50 × 50 cm grid offers the best probability of detection without prolonging search time. 125
Recommendations
We recommend the initial probe pass should be limited to a depth of 1.5 m using 3-holes-per-step or slalom probing to cover a 50 × 50 cm grid. Strong recommendation, low quality evidence.
RECCO
The RECCO search system uses harmonic radar to detect an avalanche victim. The searcher uses a RECCO receiver to identify a RECCO reflector diode embedded in the victim's clothing. The reflector diodes are small and light and do not require a power source. Many manufacturers have incorporated these reflectors into clothing. Critically buried avalanche victims have been located alive with RECCO. 27
RECCO is intended only for professional rescue as it requires training and practice. Other disadvantages of RECCO include short detection range because of attenuation of the signal, especially in dense, wet snow, and the potential for false positive signals from searchers or reflective items such as cell phones.27,126
Recommendations
We recommend professional rescue teams have RECCO search capabilities with established search protocols. Strong recommendation, low quality evidence.
Dog Search
Avalanche rescue dogs are trained to detect buried victims by scent. Survival of victims found by dogs may be no better than that of victims found by organized probe lines. 127 Limitations of dog searching include the time to transport a team to the site and distractions caused by contamination of the debris field by bystanders. Training avalanche rescue dogs requires substantial time and resource commitments.
Recommendations
We suggest professional rescue teams should consider using dogs trained in avalanche rescue to search debris for buried victims, despite the disadvantages, especially for victims without transceivers. Ungraded: Expert consensus.
Helicopters
Helicopters can shorten response times to remote locations, decrease risk by moving rescuers safely over hazardous terrain to reach avalanche accidents, and evacuate victims rapidly from technical or remote terrain. 128 Helicopters can be used to search from the air with avalanche transceivers and with RECCO.126,129 The helicopter RECCO system and long-range helicopter transceiver units have longer ranges. Helicopter Emergency Medical Services (HEMS) may provide resources that complement capabilities of search and rescue helicopters. Some specially trained HEMS programs can perform both avalanche search and medical transport. 119
Helicopters can be very useful but also present risks. 130 Conditions such as inclement weather and pilot proficiency in mountain environments can significantly affect helicopter performance and safety.119,131
Recommendations
We suggest professional rescue teams should only use helicopters with crews specifically trained in avalanche rescue, if possible. Helicopter teams should consider long-range RECCO and avalanche transceivers. We suggest rescuers should make a risk assessment before launching a helicopter and should follow rigorous safety guidelines. Ungraded: Expert consensus.
Multiple Burial and Multiple Causality Incidents
If there is more than one buried victim, a shortage of resources is likely, especially in the first phases of companion and organized rescue.132,133 Even highly developed and well-equipped emergency medical services can be overwhelmed. 134 Teams may need to use rescue triage during the search and rescue phase, based on parameters such as terrain characteristics, vegetation, snowpack, additional avalanche risk, and burial depth. Prioritization of buried victims requiring less effort to extricate or who were less exposed to trauma may improve the overall outcome of the buried cohort. There are evidence-based search and rescue tools, such as AvaLife, that also include medical treatment protocols, striving for the greatest good for the greatest number in avalanche accidents with multiple burials and limited resources. 133 Other protocols have also been developed. 54
AvaLife contains a search and excavate module (Figures 3 and 4) as well as medical modules. 135 Mountain rescue teams should be prepared to manage accidents with multiple burials according to recommendations of the International Commission for Mountain Emergency Medicine. 136 Good communication on site is essential for an efficient, safe rescue. 134
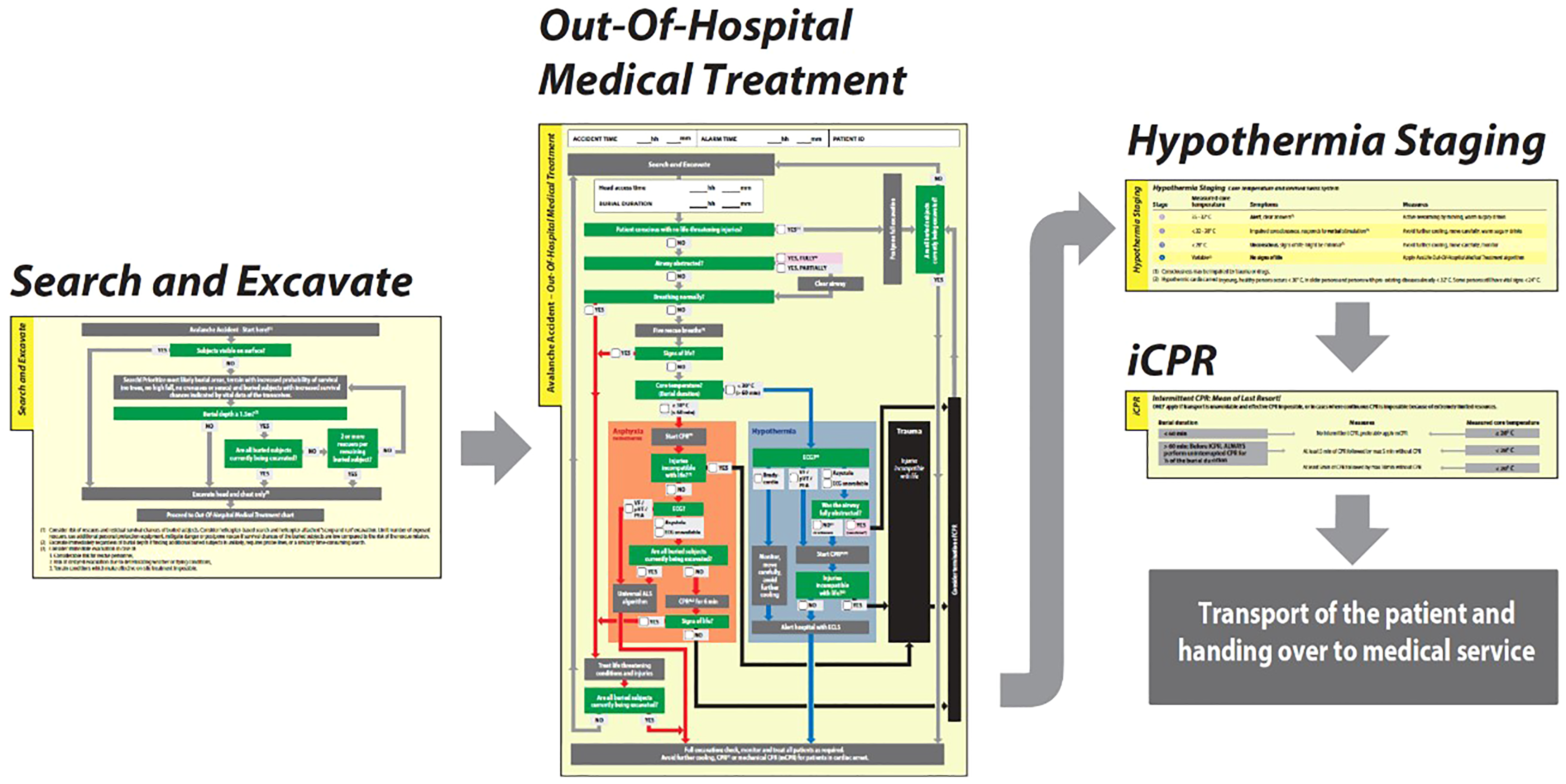
Overview of the AvaLife BLS modules. The modules follow a step-by-step approach to technical and medical avalanche rescue. From Genswein et al. 135 Used under Creative Commons CC-BY license.
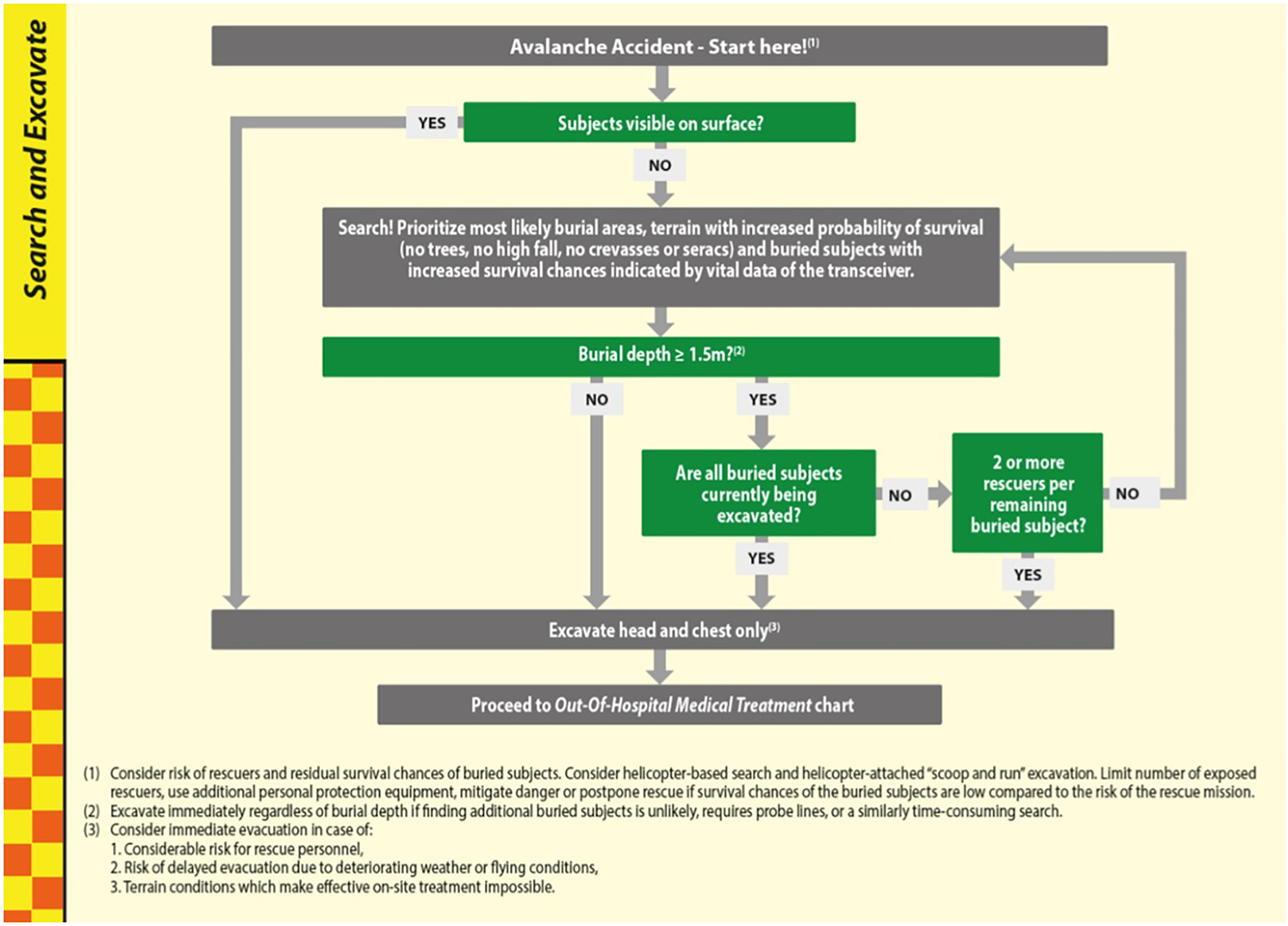
The search and excavate module of AvaLife includes the burial depth threshold of ⩾150 cm and 2 or more rescuers per remaining buried victim. These criteria are required to distinguish victims who should be excavated immediately from cases when excavation should be postponed. From Genswein et al. 135 Used under Creative Commons CC-BY license.
Recommendations
We suggest mountain rescue organizations should be prepared to manage multiple burial accidents. Weak recommendation, low quality evidence.
Resuscitation
Resuscitation at the scene of an avalanche can be difficult. 100 Rescuers may have to start CPR and advanced life support (ALS) in a confined space in an austere environment with limited equipment and personnel. Resuscitation can start once the head and chest have been exposed, even before complete extrication. Information about the duration of burial, patency of the airway, presence of an air pocket, and vital signs at the time of extrication should guide treatment and transport decisions early in the resuscitation. 23
Factors predicting survival after avalanche burial include severity of injury, duration of critical burial, airway patency, core temperature, initial serum potassium, if available in the field, and the Hypothermia Outcome Prediction after Extracorporeal Life Support (HOPE) score.53,137
The European Resuscitation Council (ERC) updated guidelines for on-site triage of avalanche victims in cardiac arrest and for transport decisions in 2021 (Figure 5). 23 Retrospective observational studies have reported survival rates of avalanche victims in cardiac arrest receiving prolonged CPR and extracorporeal life support (ECLS) as low as 11% in unwitnessed cardiac arrest.25,138,139 A Swiss study of 66 victims found that of 126 critical decisions, 117 (93%) conformed to ERC guidelines. Despite high adherence, no victim survived. 140 The likelihood of survival is low for victims cooled slowly to <30°C before cardiac arrest. Victims in ventricular fibrillation and pulseless electrical activity have greater likelihood of survival than victims with asystole. Victims in cardiac arrest with short burial and early initiation of resuscitation by their companions have the best chances of surviving neurologically intact. Published cooling rates of completely buried avalanche victims range from 0.6°C h−1 to 9.4°C h−1.19,37,38,43,63,140-142 Rapid cooling under snow is associated with having an air pocket, sweating before being buried, lean body habitus, thin monolayer clothing, uncovered head and hands, impaired consciousness, no shivering, and hypercapnia. 63
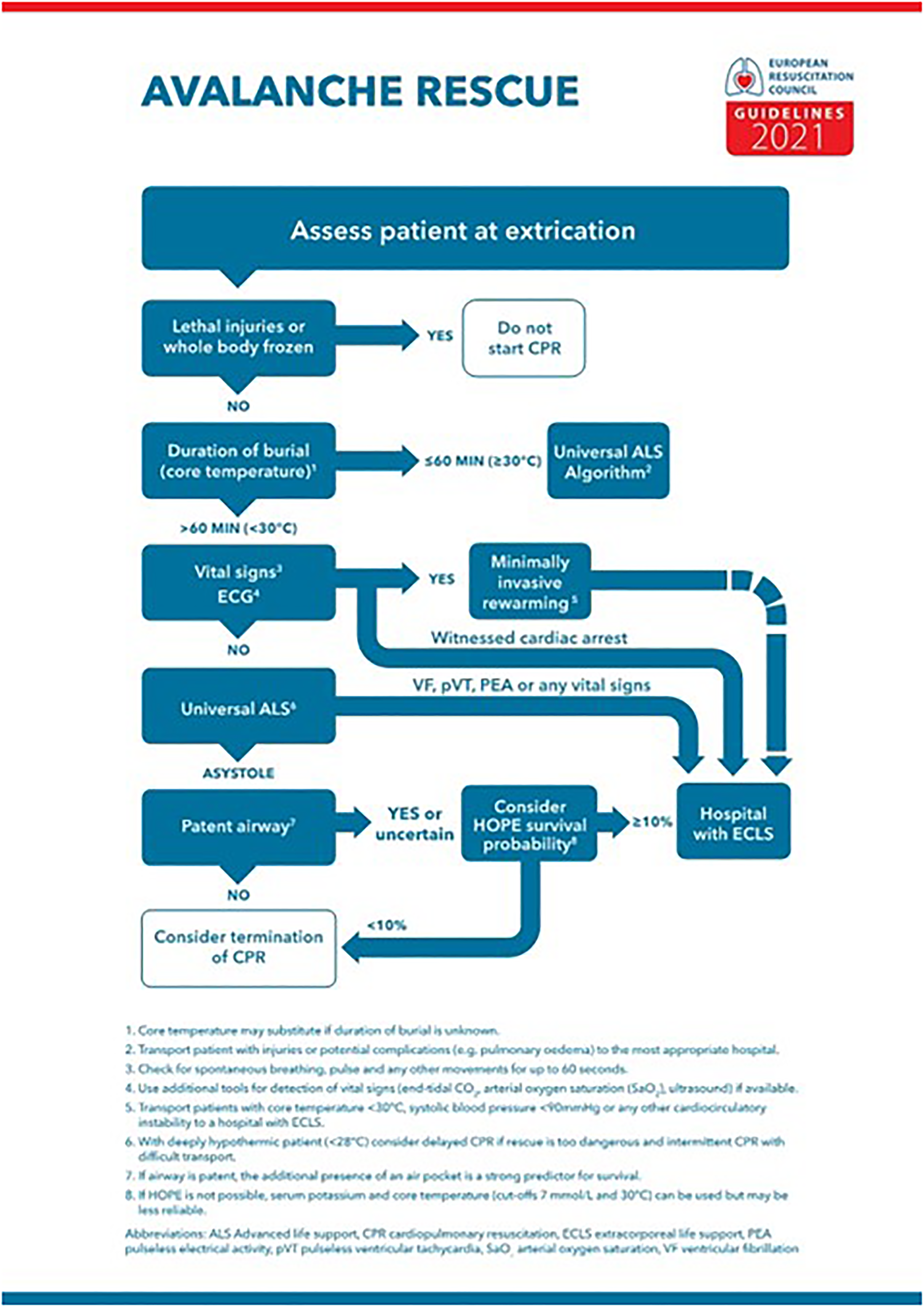
Avalanche accident algorithm for management of critically buried victims. From Lott et al. 23 Used with permission. ECLS, extracorporeal life support.
After 60 min of burial, if the airway is patent, successful resuscitation of victims in cardiac arrest with moderate or severe hypothermia may be possible. There is no reported successful resuscitation of an avalanche victim in cardiac arrest with core temperature >30°C with ECLS rewarming because cardiac arrest is likely caused by asphyxia.
The HOPE score should be used to predict outcome after hypothermic cardiac arrest in avalanche victims being considered for ECLS rewarming (Figure 5).137,143 Serum potassium alone should only be used for triage if the HOPE score cannot be used. If there are signs of death, such as freezing of the entire body or trauma incompatible with life, CPR should be terminated or withheld.144,145
Critical Burial of an Uninjured Victim
If a victim is alert and responsive after critical burial, cold stress or mild hypothermia is still a possibility, especially with burials longer than 30 min. Rewarming can occur with shivering thermogenesis. Critically buried avalanche victims can develop pulmonary edema several hours after extrication. The etiology seems to be a combination of negative-pressure induced pulmonary edema and hypoxia-induced left heart failure.41-43 In a Swiss study of victims buried >60 min but <24 h, the survival rate was 19%. 146 Burial depth is inversely correlated with survival. 24
Recommendations
We suggest that a critically buried victim, even if uninjured, should be transported to the nearest medical facility capable of evaluating and stabilizing the victim. Weak recommendation, low quality evidence.
Management of Trauma
Depending on climate, snow quality, terrain, and speed of rescue, approximately 25% of buried victims will die from trauma. The most common fatal injuries are multiple trauma, head injury, and spinal injury.12,50 Risk factors include steep, forested, and rocky terrain.4,12,16,50 A Swiss study reported that summer avalanches are rare (21/482 accidents) but are more likely to result in fatal trauma (33/35 fatalities). 50
Victims with injuries such as head trauma, spinal injuries, and long bone fractures should be treated using standard advance trauma life support. Suspected cervical spine injuries should be managed using validated guidelines such as NEXUS 91 or the Canadian C-Spine Rule. 92 The Wilderness Medical Society Clinical Practice Guidelines for Spinal Cord Protection present recommendations for preventing, evaluating, and managing spinal injuries in the wilderness but have not been validated.147,148 Hypothermia inhibits coagulation and increases bleeding.149-151 Preventing cooling during long transports may be critical.
Recommendations
We suggest avalanche resuscitation should include trauma care and that suspected spinal injuries should be managed according to the recommendations of validated guidelines such as NEXUS or the Canadian C-Spine Rule. Ungraded: Expert consensus.
Management of Hypothermia
Core temperature is most accurately measured using an esophageal probe, but epitympanic temperatures are more practical in victims who are not fully conscious and without airway protection with endotracheal intubation or extraglottic devices.152,153 Tympanic temperatures are unreliable in hypothermic victims.
Vital signs and core temperatures are positively correlated. Level of consciousness has the best correlation. 154 The RSS for staging accidental hypothermia uses level of consciousness to estimate the degree of hypothermia and the risk of cardiac arrest. (Figure 6). 60 The RSS is reliable only if the victim does not have a coexisting condition affecting the level of consciousness, such as intoxication or traumatic brain injury. The RSS is useful if temperature measurement is not available. A cold, unconscious avalanche victim likely has moderate or severe hypothermia. The WMS guidelines for accidental hypothermia 58 and the ERC guidelines 23 present recommendations for treating hypothermia.

The Revised Swiss System for staging of accidental hypothermia. From Musi et al. 60 Used under Creative Commons CC-BY license. AVPU, Alert, Verbal, Pain, Unresponsive.
Recommendations
We recommend measuring core temperature or using the RSS to estimate the risk of hypothermic cardiac arrest. Strong recommendation, moderate quality evidence.
Recommendation
We recommend that avalanche resuscitation should include treatment of hypothermia according to the WMS guidelines for accidental hypothermia or the ERC guidelines. Strong recommendation, moderate quality evidence.
Initiating Resuscitation
Waiting to start CPR until a victim is supine during the initial extrication is likely to cause a delay. In a manikin study simulating a restricted environment CPR in an over-the-head or straddle position had comparable quality CPR to a standard CPR position. 155 All victims who are extricated should be assessed for airway, breathing, and circulation. Victims with witnessed cardiac arrest should undergo immediate CPR. Witnessed cardiac arrest is often caused by hypothermia.65,156 The chances of survival are far better in hypothermic cardiac arrest compared to those of normothermic cardiac arrest from trauma or asphyxia.157,158 A meta-analysis of 221 hypothermia victims reported an overall survival rate of 27%. Most survivors (83%) had no neurologic deficit. Even unwitnessed hypothermic cardiac arrest presenting with asystole should not preclude ECLS rewarming. In one study, 48% of victims with asystole survived. Of the survivors, 79% had good neurological outcomes. 158
Unless there is a contraindication to resuscitation, rescuers should start CPR as soon as possible. Rescuers who are suitably trained and equipped should perform ALS interventions. 159
In victims buried ≤60 min with core temperatures ≥30°C, cardiac arrest is usually a result of trauma or asphyxia rather than hypothermia. ECLS rewarming is contraindicated. If standard CPR or ALS does not achieve return of spontaneous circulation (ROSC) within 30 min, the chance of survival is minimal and further attempts at resuscitation should be terminated.144,160-162 Definite signs of death, such as trauma incompatible with life or whole body frozen, are indications to withhold or terminate CPR. 145
If duration of burial is >60 min, the core temperature <30°C, and the victim had a patent airway at extrication, cardiac arrest may have been caused hypothermia. Rescuers should attempt resuscitation with prolonged CPR, transfer to definitive care, and extracorporeal rewarming. 84
CPR and ALS may need to continue beyond 60 min, especially when cardiac arrest may have been caused by hypothermia or if there was a witnessed cardiac arrest after extrication. If core temperature is <30°C, defibrillation may be unsuccessful, but prolonged CPR may be successful, even if it takes hours until a victim is rewarmed to 30°C. 23 Delayed and intermittent CPR may be necessary in hypothermic victims with suspected severe hypothermia or core temperatures <28°C, when immediate and continuous CPR is not possible (Figure 7).
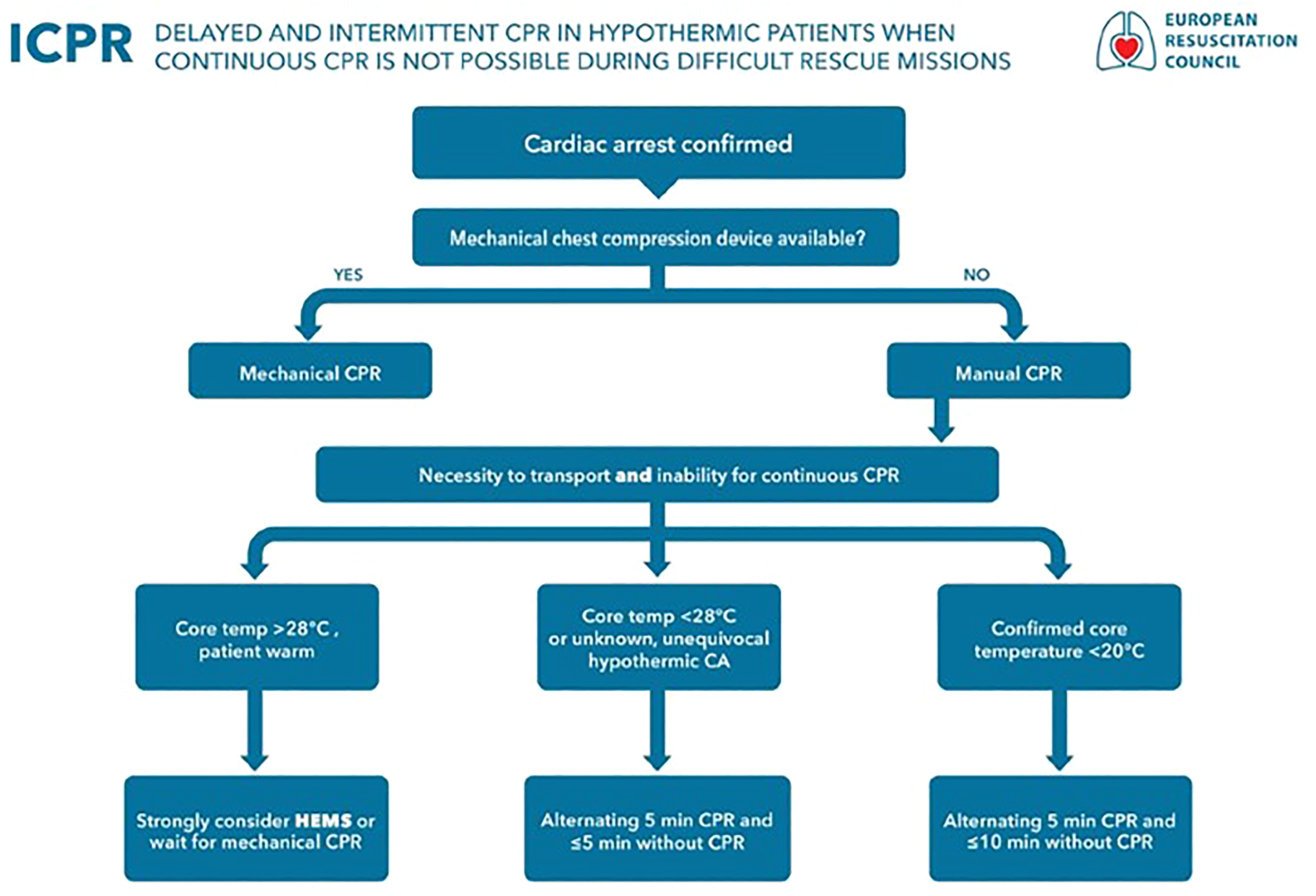
Delayed and intermittent CPR in hypothermic victims when continuous CPR is not possible. From Lott et al. 23 Used with permission. CA, cardiac arrest; CPR, cardiopulmonary resuscitation.
Recommendations
We recommend that if there are no vital signs and no indications for withholding resuscitation, rescuers should start CPR and ALS while performing further assessment. Strong recommendation, moderate quality evidence.
Recommendation
We recommend that in a technically difficult rescue with a severely hypothermic victim (core temperature <28°C), delayed and intermittent CPR may be required. Strong recommendation, moderate quality evidence.
Recommendation
We recommend that if duration of burial is >60 min, core temperature is <30°C, and the airway is patent, cardiac arrest was possibly caused by hypothermia, so CPR should be continued and the victim transported to a hospital with ECLS capability. We recommend that if duration of burial is ≤60 min, core temperature is ≥30°C, and the airway is not patent, resuscitation attempts should be stopped if ROSC is not achieved within 30 min. Strong recommendation, moderate quality evidence.
Defibrillation
If a defibrillator is available, rescuers should place pads and analyze the rhythm before moving or extricating the victim. The core temperature at which defibrillation should be initiated and the power and number of shocks for a hypothermic victim in cardiac arrest with a core temperature <30°C have not been established. Defibrillation may be successful below a core temperature of 28°C or even lower. However, ROSC after defibrillation is more stable and less commonly degenerates back into ventricular fibrillation at higher core temperatures (≥30°C). 163 Delaying continued defibrillation attempts until core temperature is ≥30°C may be reasonable, because every shock can cause further myocardial injury. 23 CPR and rewarming may need to be continued for several hours to allow successful defibrillation. 164 The longest resuscitation in a hypothermic victim in cardiac arrest lasted 8 h and 42 min: mechanical CPR lasted 3 hours and 42 min, followed by 5 h of ECLS.56,165
The WMS hypothermia guidelines recommend 1 defibrillation attempt for a victim in cardiac arrest with core temperature <30°C. 58 The American Heart Association recommends defibrillation attempts every 2 min for hypothermic victims in cardiac arrest. 166 The ERC guidelines recommend up to 3 defibrillation attempts with a core temperature <30°C, delaying further attempts until core temperature is ≥30°C if ventricular fibrillation persists after 3 shocks. 23
Recommendations
We recommend attempting defibrillation in cardiac arrest after avalanche burial according to local protocols. If defibrillation is unsuccessful, we recommend CPR in hypothermic cardiac arrest should continue until the victim is rewarmed to a core temperature ≥30°C. Strong recommendation, moderate quality evidence.
ALS
An unconscious victim of avalanche burial may benefit from endotracheal intubation for airway control and assisted ventilation. Extraglottic airways can be used if part of local protocol. Hypocapnia from hyperventilation decreases cerebral blood flow because of vasoconstriction. This is likely to be detrimental, especially to a victim with traumatic brain injury or hypothermia. Ventilation should be targeted to normocapnia.37,61,167 If intravenous fluids are available, intravenous or intraosseous volume resuscitation with isotonic fluids, warmed, if possible to 40°C, can help support circulation. Hypothermic cardiac arrest is associated with a lower EtCO2 than normothermic cardiac arrest. In contrast to normothermic cardiac arrest, EtCO2 <10 mm Hg should not be used to predict a fatal outcome.165,168
Recommendations
We recommend that if duration of burial is ≤60 min or core temperature ≥30°C, standard resuscitation and ALS should be performed if possible. This should include volume resuscitation and endotracheal intubation or placement of an extraglottic airway with normocapnic ventilation if indicated. Strong recommendation, moderate quality evidence.
Recommendation
We recommend not using EtCO2 <10 mm Hg to predict outcome. Strong recommendation, high quality evidence.
Mechanical Chest Compression
Mechanical chest compression achieves higher quality than manual CPR in technically difficult settings and during prolonged transport. A single study in an urban environment failed to show an improvement in outcome with mechanical chest compressions compared to manual compressions. 169 In a manikin study simulating a technically difficult helicopter rescue, chest compressions with a mechanical device were technically superior to manual chest compressions. 170 The ERC recommends mechanical chest compressions during CPR in long or technically demanding rescues. 23
Recommendations
We recommend that if available, mechanical chest compressions should be used for technically difficult or long transports. Strong recommendation, low quality evidence.
Delayed and Intermittent Resuscitation
If a victim is in cardiac arrest with a known or suspected core temperature <28°C and continuous CPR is impossible for safety reasons because the number of rescuers is limited or performing CPR during extrication and transport is difficult, CPR can be delayed or intermittent 171 according to the WMS hypothermia guidelines and still be successful.38,172,173 Without a mechanical chest compression device, a victim with unknown core temperature, but likely in hypothermic cardiac arrest or with core temperature <28°C, should receive at least 5 min of CPR alternating with periods of ≤5 min without CPR. In a victim with a core temperature <20°C, pauses in CPR can be extended to ≤10 min. 171 Hands-off times should be kept as short as possible (Figure 7). 23
Recommendations
We recommend that if continuous CPR is not possible in a victim with a core temperature <28°C or with an unknown core temperature but likely hypothermic cardiac arrest, CPR can be delayed or intermittent. Strong recommendation, moderate quality evidence.
Witholding or Terminating Resusciation
Trauma
The likelihood of survival after traumatic cardiac arrest in an avalanche is extremely low.144,145 No survivor with traumatic cardiac arrest from an avalanche has ever been reported.
Recommendations
We suggest that if a critically buried victim is in cardiac arrest because of trauma, rescuers should withhold resuscitation. Weak recommendation, low quality evidence.
Duration of Burial, Core Temperature, and Airway
Critically buried victims are very likely to die within 60 min from asphyxia if the airway is not patent or if the air pocket is inadequate to support effective ventilation.21,32,35 Standard ALS can lead to ROSC in an asphyxiated victim, but with a high risk of permanent neurologic damage. Avalanche victims who are found pulseless and apneic or in asystole with core temperature ≥30°C at extrication have most likely died from asphyxia. 138
An avalanche victim with core temperature <30°C and a patent airway at extrication with ventricular fibrillation, pulseless electrical activity, pulseless ventricular tachycardia, or a perfusing rhythm after a witnessed cardiac arrest has a good chance of survival.38,138,174
Recommendations
We recommend that in a pulseless and apneic victim, regardless of cardiac rhythm, with duration of burial of ≤60 min and core temperature ≥30°C, rescuers should consider terminating resuscitation if ROSC does not occur within 30 min, depending on local protocols. Strong recommendation, moderate quality evidence.
Recommendation
We recommend that in a pulseless and apneic victim, regardless of cardiac rhythm, with an obstructed airway and duration of burial of >60 min, rescuers should consider terminating resuscitation if ROSC does not occur within 30 min, depending on local protocols. Strong recommendation, moderate quality evidence.
Prediction of Survival with ECLS Using the HOPE Score
The HOPE score is a multivariate algorithm to predict survival of hypothermic victims in cardiac arrest resuscitated with ECLS rewarming. It can be accessed freely at https://www.hypothermiascore.org. 143 Discrimination between survivors and non-survivors is better with the HOPE score than with serum potassium alone.59,143 The HOPE score has been externally validated. 137 If the HOPE score cannot be used, serum potassium alone can be used for triage. 59 Avalanche victims with possible asphyxia, should be scored “without asphyxia” and “in cardiac arrest at extrication.” The HOPE score was not developed to predict survival with ECLS of avalanche victims in cardiac arrest survival but is currently the best tool for this purpose.175,176
Traditionally serum potassium has been used for outcome prediction. The highest recorded potassium in a successfully resuscitated avalanche victim was 6.4 mmol L−1. 19 One avalanche victim with serum potassium 8.0 mmol L−1 had ROSC but did not survive. 177 It may be reasonable to transport an avalanche victim with unwitnessed cardiac arrest and other factors that might lead to termination of resuscitation to the nearest medical facility to determine the HOPE score, including serum potassium, and to assess eligibility for invasive rewarming techniques. If the HOPE score cannot be calculated, ECLS rewarming should not be initiated unless core temperature is <30°C and serum potassium is <7 mmol L−1. 59
Recommendations
We recommend using the HOPE score for outcome prediction in hypothermic avalanche victims in cardiac arrest being considered for ECLS rewarming. If the circumstances are not clear, choose asphyxia as the reason for cardiac arrest. Strong recommendation, moderate quality evidence.
Recommendation
We recommend in an avalanche victim with a serum potassium of >7 mmol L−1, rescuers should withhold resuscitation, and ECLS rewarming should not be initiated. Strong recommendation, high quality evidence.
Risk to the Rescuers
After an avalanche, ongoing hazards may include additional avalanches, austere weather, and health risks to the rescuers, such as exhaustion, hypothermia, or frostbite. Rescuers should exercise caution when approaching an avalanche accident to avoid putting themselves in danger. Personal safety should be the first priority of each rescuer. Safety of the rescue team is the second priority. Only after these are assured should rescuers extricate and treat any victims.
Recommendations
We suggest that if the risks to the rescuers are unacceptably high, rescue attempts should be delayed until conditions improve, or the risks can be mitigated sufficiently. Ungraded: Expert consensus.
Transfer to Definitive Care
A severely hypothermic victim in cardiac arrest should be resuscitated with ECLS, if possible.178-181 Transport to a facility with ECLS may be beneficial for a victim with core temperature <30°C and hemodynamic instability, including systolic blood pressure <90 mm Hg or ventricular arrhythmias. 28 Victims with trauma should be transferred to a trauma center, if feasible. ECLS rewarming is possible in trauma victims. A hypothermic victim in cardiac arrest who cannot be transported to a facility with ECLS capability within 6 h should be taken to a closer hospital for non-ECLS rewarming.182-184
Recommendations
We recommend that a hypothermic avalanche victim in cardiac arrest or with hemodynamic instability should be transferred as rapidly as possible to a facility with ECLS capability if possible within 6 h. Strong recommendation, high quality evidence.
Recommendation
We recommend that if a hypothermic avalanche victim in cardiac arrest or with hemodynamic instability cannot be transported to an ECLS center within 6 h, the victim should be taken to a closer hospital for non-ECLS rewarming. Strong recommendation, low quality evidence.
Avalanche Victim Resuscitation Checklist
Adherence to avalanche resuscitation guidelines is often suboptimal. 185 The International Commission for Mountain Emergency Medicine (ICAR MedCom) published an avalanche victim resuscitation checklist in 2015 186 and an updated checklist in 2017. 187 The checklist is meant to improve adherence to guidelines and to help collect medical data for refining the guidelines (Figure 8). 187 The checklist is designed to be completed at the site of the accident and remains with the victim until hospital admission.

The Avalanche Resuscitation Checklist from the International Commission for Alpine Rescue. Adapted from Kottmann et al. 186 BLS, Basic Life Support.
Recommendations
We recommend that an avalanche resuscitation algorithm be used whenever possible. We recommend that a checklist be used to improve adherence to the ICAR MedCom resuscitation algorithm. Strong recommendation, low quality evidence.
Multiple Burials
Rescuing multiple burial victims can overwhelm locally available resources.134,136 A Monte Carlo simulation of avalanche accidents with multiple victims and a limited number of rescuers 133 was used to determine the greatest good for the greatest number of victims by limiting the duration of CPR of victims in cardiac arrest when other victims are still buried, and additional personnel are not available. The guidelines were published as AvaLife. 135 AvaLife limits CPR to 6 min in mass casualty incidents for victims who are normothermic and buried ≥150 cm deep.
Recommendations
We suggest rescuers should be prepared to triage in multiple burial situations. Ungraded: Expert consensus.
Post-Traumatic Stress Disorder After Avalanche Burial
Avalanche burial is a traumatic event. Preventive measures and early diagnosis of post-traumatic stress disorder may reduce the psychological burden.64,188 Avalanche rescuers are also at risk for long-lasting psychological effects. Formal psychological support may be beneficial. 189
Recommendations
We recommend providing psychological assistance to avalanche victims and rescuers. Strong recommendation, low quality evidence.
Research
The ICAR MedCom has determined quality indicators for the management of avalanche victims128,190 that should be used in reporting avalanche accidents. Registries might be useful to improve protocols for the management of avalanche victims. 191
Recommendations
We recommend that avalanche accident registries should be used to improve the management of victims. Strong recommendation, moderate quality evidence.
Nonavalanche Snow Burial
Nonavalanche snow burial (NASB), also called “nonavalanche-related snow immersion” or “snow submersion suffocation,” is different from avalanche burial. NASB has been reported in skiers, snowboarders, snowshoers, and snowmobilers who fell headfirst into tree wells or deep powder snow. Victims who are unable to extricate themselves die from asphyxia when snow compacts around the head.
The only published references are case reports, a review article, and a small simulation study.8,192 Self-extrication can be difficult or impossible. Buried victims who remove their skis sink deeper. Position likely affects the chance of successful self-extrication. Victims who were able to extricate themselves were often flexed at the waist. Case reports suggest that asphyxiation can occur rapidly, but there is no good evidence regarding the time it takes for death to occur or the exact mechanism of asphyxia.193-197
The best way to prevent NASB is to recognize and avoid tree wells and to avoid burial in soft snow by staying within the limits of one's skills and not falling. Other possibly effective measures to prevent fatal burial include maintaining voice and visual contact with a partner, alerting a partner when falling by yelling, and grabbing tree branches while falling in an attempt to stay upright.
Buried victims can use gentle rocking motions to try to pack the snow and get a purchase in attempting to self-extricate. 192 However, a simulated burial study found that victims sank deeper when struggling and when skis or snowboards were jettisoned. Parkas collected more snow when the victims were upside down. 192 Whether skis and snowboards should remain attached or be jettisoned is unclear. In 2 cases, victims were spotted because skis or a snowboard was still attached.193-195,197
There are no data on the use of avalanche transceivers, radios, or mobile phones in NASB. One body was recovered using an avalanche beacon and another victim was found alive after using a voice-activated 2-way radio. 197 One manufacturer has speculated that deploying an airbag might create an air pocket.196,197 An airbag that deflates after deployment might create an air pocket. 89 A small study suggested an airbag that deflates after burial might be useful to prevent nonavalache snow burial asphyxia. 93
Recommendations
Avoiding falling into tree wells or deep powder snow is the only known means of preventing NASB. We suggest that a victim of NASB should keep skis or snowboard attached to avoid sinking deeper and to provide visual clues to rescuers. Weak recommendation, low quality evidence.
Recommendation
We suggest that in areas with deep snow or tree wells, travelers should stay in voice and visual contact with a partner. If falling, we suggest that a person should yell to alert a partner, attempt to grab a tree branch, and attempt to land upright. Ungraded: Expert consensus.
Recommendation
We suggest that a transceiver may be useful to locate a person buried in deep snow or a tree well. We also suggest that an airbag that deflates after deploying may create an air pocket that might help prevent or delay asphyxia. Ungraded: Expert consensus.
Discussion
These guidelines are evidence-based recommendations for prevention, rescue, and resuscitation in avalanche and NASB accidents. The foundation of avalanche safety for professional personnel and recreational enthusiasts is avoidance of high-hazard, avalanche-prone areas. Avalanche safety should be learned through education about avalanche mechanics, safe route finding, traveling in appropriate snow and weather conditions, knowledge of local avalanche forecasts, routine practice with equipment, gaining experience from skilled partners and guides, taking courses, and using good judgment. Good judgment is the single most important factor in avalanche safety.
Data regarding avalanche safety techniques and management of avalanche injuries are limited, as with all of wilderness medicine. It is difficult to conduct randomized, controlled trials or simulate avalanche accidents. Future research should evaluate the efficacy of helmets and avalanche airbag configurations in trauma prevention, the causes of airbag nondeployment, and the use of new transceiver technology. Advances in ALS, ECLS, dog search, and aeromedical evacuation may lead to improved methods for managing avalanche victims.
Supplemental Material
sj-pdf-2-wem-10.1016_j.wem.2023.05.014 - Supplemental material for Wilderness Medical Society Clinical Practice Guidelines for Prevention and Management of Avalanche and Nonavalanche Snow Burial Accidents: 2024 Update
Supplemental material, sj-pdf-2-wem-10.1016_j.wem.2023.05.014 for Wilderness Medical Society Clinical Practice Guidelines for Prevention and Management of Avalanche and Nonavalanche Snow Burial Accidents: 2024 Update by Christopher Van Tilburg, MD, Peter Paal, MD, Giacomo Strapazzon, MD, PhD, Colin K. Grissom, MD, Pascal Haegeli, PhD, Natalie Hölzl, MD, Scott McIntosh, MD, MPH, Martin Radwin, MD, William “Will” R. Smith, MD, Stephanie Thomas, MS, Bruce Tremper, MS, David Weber, FP-C, Albert R. Wheeler, MD, Ken Zafren, MD, and Hermann Brugger, MD in Wilderness & Environmental Medicine
Footnotes
Acknowledgments
The authors thank Dale Atkins and Jürg Schweizer for their assistance with statistics.
Author Contribution(s)
For 2017 and 2024 update, all authors contributed to acquisition of data, analysis of data, drafting the manuscripts, critical revision of the manuscripts, and approval of one or both of the final manuscripts.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Correction (March 2024):
This article has been updated to correct the error on page 34S. The corrected statement now reads: Avalanche victims with possible asphyxia, should be scored “without asphyxia.”
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.