
Abstract
Objective
The objective of this study was to examine the patterns of severe injury documented at a northern British Columbia regional trauma center based on age, sex, month of year, activity type, injury type, and injury severity as they relate to participation in outdoor recreational activities.
Methods
A retrospective analysis of data abstracted from the British Columbia Trauma Registry for patients sustaining injuries between April 1, 2004, and March 31, 2007, while engaged in outdoor recreational activities in the Northern Health Authority. The British Columbia Trauma Registry inclusion criteria are as follows: 1) admitted for treatment of injuries sustained from the transfer of external energy or force; 2) admitted to the facility within 7 days of injury; and 3) length of stay more than 2 days or in-hospital mortality.
Results
In all, 159 patients met study criteria. August and September were peak injury months (mean 7.3 and 7.0 per month, respectively). The highest injury patterns involved cycling (n = 31), all-terrain vehicle operation (n = 30), horseback riding (n = 22), and snowmobiling (n = 22). Of the 159 patients, 76.1% were male, with a peak age distribution between 10 years and 19 years (22%). Males were more commonly injured than females among cycling (83.9%), all-terrain vehicle (86.7%), and snowmobile (100%) traumas. Females were more commonly injured from horseback riding events (42.1%).
Conclusions
This study emphasizes the need for rapid translation of research findings into injury prevention awareness and programming in northern British Columbia, particularly relating to cycling, horseback riding, snowmobiling, and all-terrain vehicle operation. Further investigation is required to analyze long-term outcomes for this common injury population.
Introduction
Every year, millions of dollars are spent on outdoor recreational pursuits across the province of British Columbia (BC), and participation in these activities is steadily increasing. 1 In 2011 and 2012 alone, there were 19.3 million visits to BC Parks. 1 Along with any outdoor recreational activity (ORA), there comes an inherent risk of injury. To date, no studies have established injury patterns related solely to ORA in northern Canada. Understanding injury patterns related to the subset of injuries sustained during ORA will help guide future research and prevention programs in northern BC.
The Northern Health Authority (NHA) is the largest of 5 geographically determined health authorities providing health services in BC. Within the mountainous geography of northern BC, the NHA encompasses more than 500,000 square kilometres. 2 The NHA is subdivided into 3 operational Health Service Delivery Areas (HSDA): the northeast, northwest, and northern interior. The University Hospital of Northern British Columbia (UHNBC) is located in Prince George and is within the northern interior HSDA. The UHNBC is the level III trauma referral center for a population of approximately 300,000 persons from all 3 HSDA. 3
This study aims to examine the patterns of severe injury (ie, injuries resulting in a hospital stay >2 days or death) related to participation in ORA in northern BC. Categories of ORA were adapted from the National Electronic Injury Surveillance System–All Injury Program in coordination with the BC Trauma Registry (BCTR) criteria for injuries sustained while participating in sport and recreation. 4
Methods
This project was approved by the University of British Columbia Research Ethics Board and the NHA Research Review Committee. The BCTR is a standardized, hospital-based trauma registry that draws its data from designated level I to III trauma centers in BC. All data were drawn from the BCTR for patients who were assessed at UHNBC, had a discharge date between April 1, 2004, and March 31, 2007, and sustained injuries occurring while engaged in an ORA in the NHA. This timeline was chosen as BCTR data entry for UHNBC commenced in April 2004 and overall inclusion/exclusion criteria were changed in April 2007.
Patients met the following criteria for inclusion in the BCTR: 1) admitted for treatment of injuries sustained from the transfer of external energy or force; 2) admitted to the facility within 7 days of injury; and 3) had a length of stay more than two days or died. This study identified 159 cases admitted to UHNBC and included cases requiring subsequent transfer to higher level trauma centers. The collected data were analyzed for age, sex, month of year, activity type, and injury type and severity. All personal patient identifiers including health insurance and medical record numbers were excluded from the data for confidentiality purposes.
Data analysis was performed using SPSS software (Version 19.0, IBM SPSS, Armonk, NY). Statistical significance was set at α = 0.05. Analysis of categorical data (ie, sex, age, injury type, activity type) was assessed using nonparametric χ2 test of proportions and linear-by-linear association. The continuous variable of Injury Severity Score (ISS) was examined using nonparametric methods (Mann-Whitney U test for 2 groups and Kruskal-Wallis test for more than 2 groups) as the equality of variance necessary for parametric comparison between groups could not consistently be assumed.
Results
A total of 159 patients (ranging in age from 7 to 96 years) meeting inclusion criteria were injured during the 3-year study period. Overall patient demographics and a synopsis of injury frequency by age and sex category are outlined in Tables 1 and 2. Using the Maximum Abbreviated Injury Scale for anatomic categories, Figure 1 demonstrates the frequencies of body regions injured. 5 “External” refers to injuries to the skin such as abrasions, contusions, lacerations, avulsions, penetrating or degloving injury, and burns.5,6 Sixty of the 159 subjects (37.7%) had injury to more than 1 region of the body.
Patient demographics
Injury frequency by age and sex category
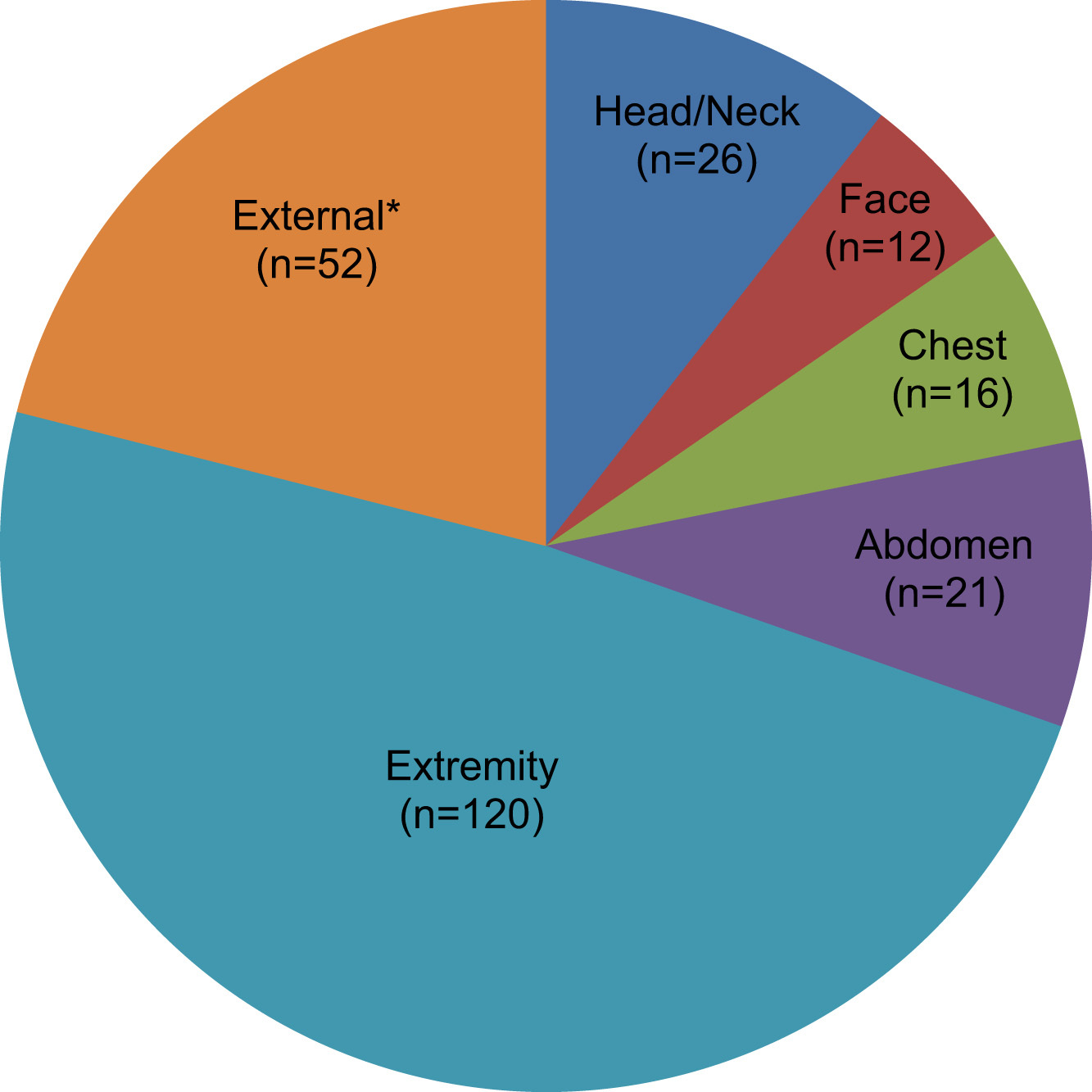
Number of individuals injured by body region. *External denotes injuries to skin including abrasions, contusions, lacerations, avulsions, penetrating or degloving injury, and burns.
There was a predominance of male patients (76.1% vs 23.9%). Overall, there was no statistically significant difference between the 4 age groups (≤19 years, 20–39 years, 40–49 years, and ≥50 years). When stratified by sex, however, age did differ (P = .004). There was an increasing proportion of female traumas within the study cohort with increasing age (P = .001). There was no significant variation of sex and age proportions with year, season, or day of week (weekday/weekend). The most common months for injuries were August and September, with a mean number of injuries per month of 7.3 and 7.0, respectively. The overall mean number of injuries per month is demonstrated in Figure 2.
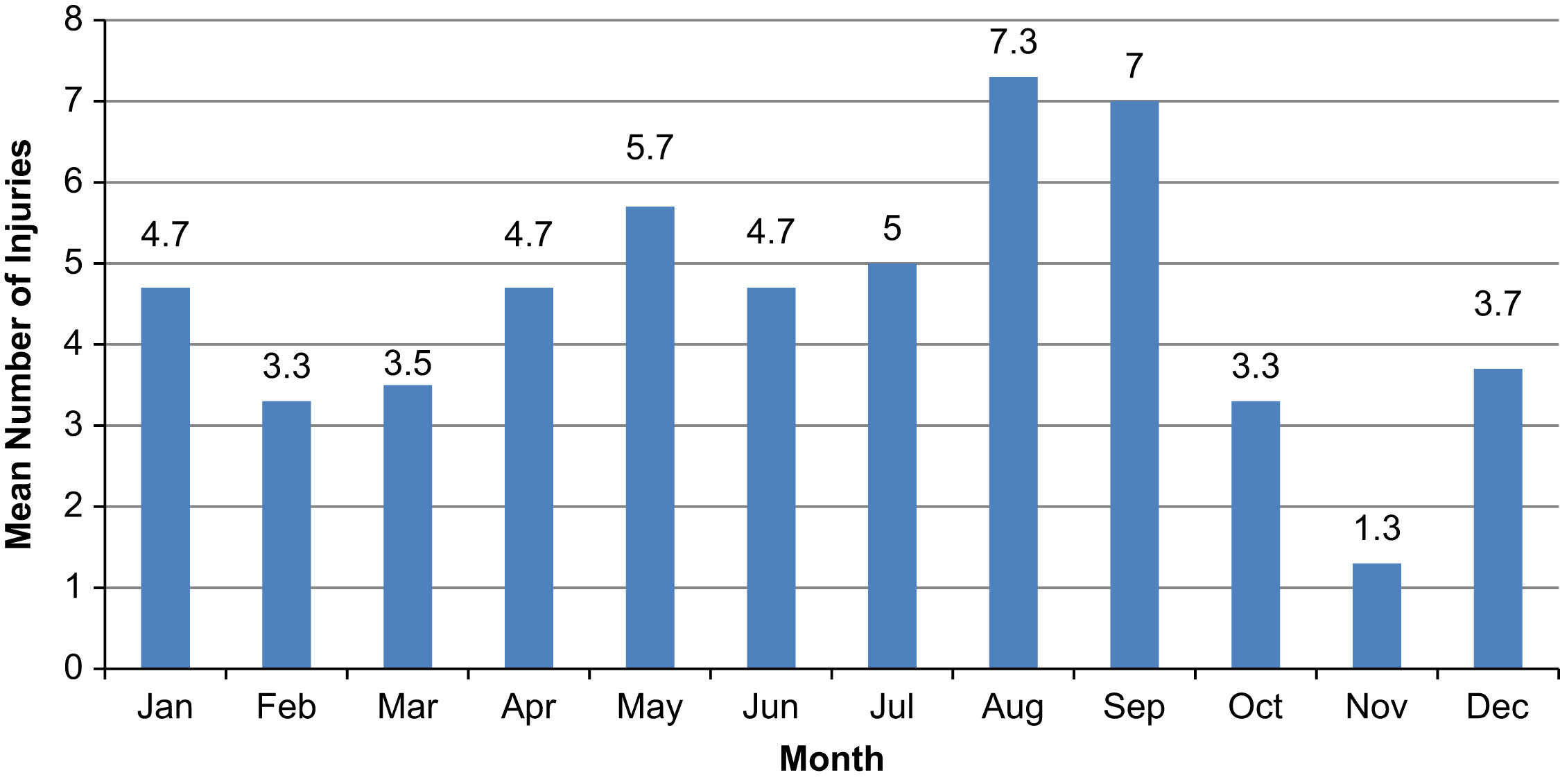
Mean number of injuries incurred per month from April 2004 to March 2007.
Injury By Activity Type
The 2 most common mechanisms of injury were transport related (81.8%) and falls of less than 1 m (10.1%). Among the transport-related events, 32.7% were related to off-road motor vehicle use such as snowmobile and all-terrain vehicle (ATV), 19.5% to bicycle use, and 13.8% to horseback riding. A subgroup of activities with the most frequent injury occurrence coupled with highest severity of injury was noted. This subset included cycling, ATV use, horseback riding, snowmobile use, and motorized biking. The injuries associated with these ORA differed by sex; trauma among males was more commonly associated with snowmobile use (18.2% vs 0%, P = .005) whereas trauma among females more often involved horseback riding (42.1% vs 5.0%, P < .001). By age group, persons 19 years and under were most commonly injured while cycling (37.5%), persons 20 to 39 years old while using ATV (25.0%) or snowmobile (22.9%), and persons 50 years and older while horseback riding and walking (23.3% and 22.0%). Cycling had a statistically significant relationship with age overall, demonstrating a declining proportion of injuries as age increased (P = .001). There were no other statistically significant associations between activity, sex, or age but that is limited by small cell sizes for several activities. The total number of injuries per activity type is outlined in Figure 3.
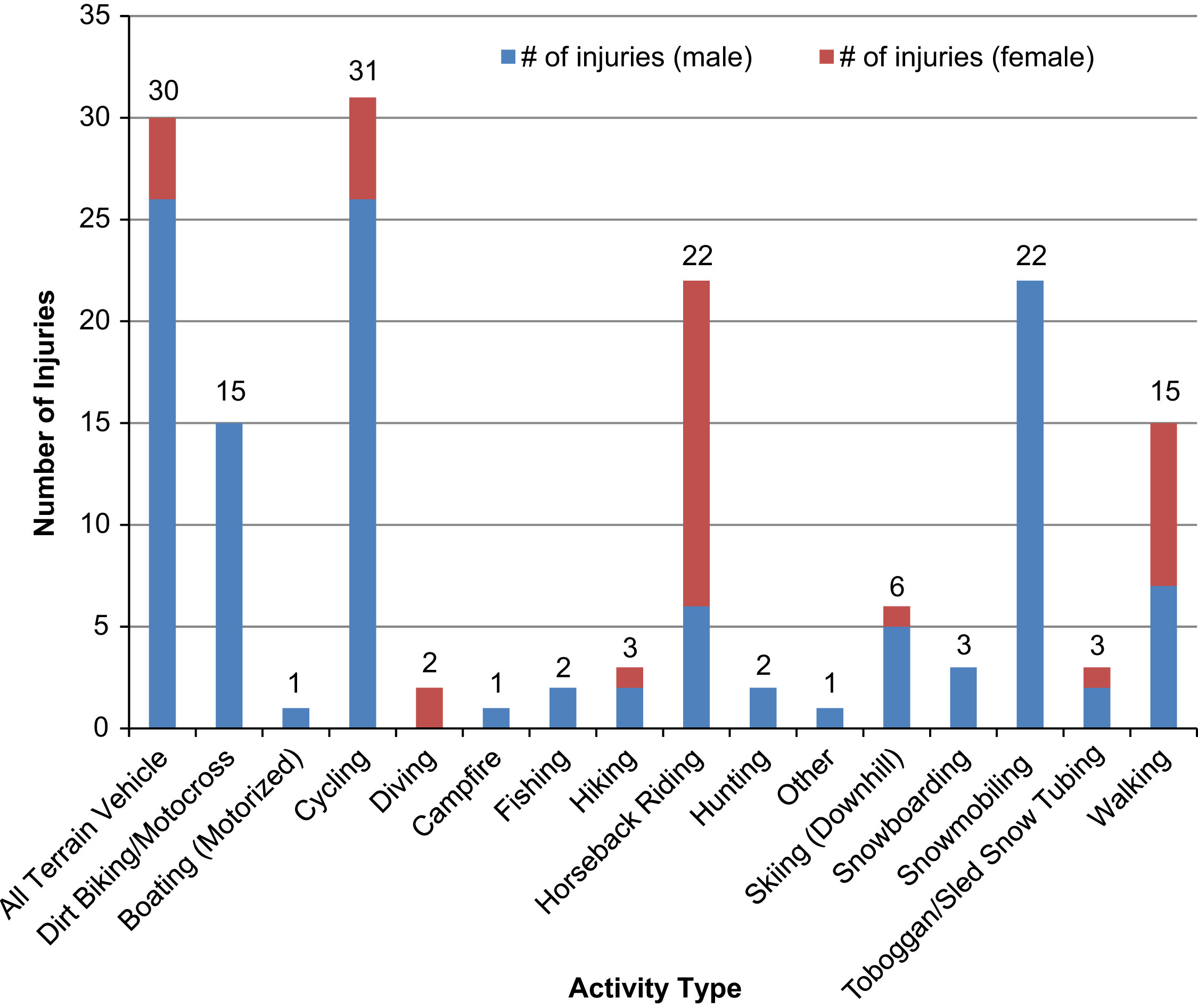
Number of injuries incurred per activity type between April 2004 and March 2007.
Injury By Severity
The ISS is a scaled score of trauma to single or multiple body regions based on the measurement of anatomic injury. 6 Given that Canadian trauma centers commonly use ISS greater than 12 as the cutpoint at which injury is of recordable severity, the score was dichotomized for clinical relevance. 7 Of the 159 subjects, 31 (19.5%) had an ISS result above 12. Among these seriously injured persons, nearly all were male (n = 27, 87.1%) and a disproportionate number experienced their trauma in summer or winter (n = 23, 74.2%). This is well outside of an equal distribution of injuries between summer/winter (50%) and spring/fall (50%; P < .001).
Discussion
Outdoor recreation encompasses a broad category of activities and is a rapidly expanding industry in North America. 8 –11 The objective of this study was to examine patterns of severe injury documented at a northern BC regional trauma center based on age, sex, month of year, activity type, injury type, and injury severity as they relate to participation in ORA.
Males (76.1%) demonstrated a higher percentage of injury than females (23.9%). It may be that more men participate in ORA and therefore appear more often in the injury data, with comparative risk between sexes unknown. Without knowing the number participating in ORA to provide context for the number injured, risk should be evaluated cautiously. Numerous studies have demonstrated similar results with higher percentage of injury in males but were unable to conclude a definitive sex linkage to ORA injury patterns without data indicating overall exposure. 8 –11 In spite of this, it is notable that the mean ISS was highest in the male-predominant (91.4%) age group of 19 years and under. The high variance of these scores indicates serious trauma among certain persons, and given the potential for a lifetime of disability in this particular age group, it would seem important that ORA injury prevention strategies include a focus on the younger male population.
The most common mechanisms of injury were related to forms of transportation (81.8%). Although the majority of transport-related trauma events occurred during participation in snowmobiling, ATV use, cycling, and horseback riding, there are sex differences of note as demonstrated in Figure 3. In comparison with other high-risk etiologies that are linked with the male demographic such as snowmobiling (18.2% male vs 0% female), this study identified that trauma within the female group more often involved horseback riding than their male counterparts (42.1% female vs 5.0% male). In addition, the older age groups (40–49 years and ≥50 years) were also more frequently involved with horseback riding injuries (23.3% and 26.7%, respectively). There are many unknown variables to be examined with regard to horseback riding and snowmobiling in northern BC such as location (eg, backcountry vs domestic), rider experience and riding type (eg, recreational vs competitive). Further evaluation of the demographics of regional horseback riding and snowmobiling participants may assist with future prevention strategies and target audiences.
Age-related analysis revealed that persons 19 years of age and under were most commonly injured while involved in cycling (37.5%). Access to bikes as compared to snowmobiles and ATVs in this population may be partly explained by cost factors and legislation limits on user age, but we cannot be certain without further investigation. There was no specific delineation made for type of cycling (eg, mountain vs road) within the BCTR. Kim et al 12 demonstrated a threefold increase in trauma center admissions due to mountain biking over a 10-year period. Mountain biking trails and facilities in northern BC centers have grown immensely over the past 10 years. Dedicated research into injury patterns related to these activities and coordination with local schools and organizations regarding specific preventative educational programming will benefit all stakeholders.
Our study did not examine the association of helmet use, alcohol consumption, and mandatory training or registration with any of the activity types. These will be important issues to identify for future investigations to help provide information on adherence to legislation and correlate this with the impact of prevention programs.
For those seriously injured (ISS >12), a larger proportion experienced their trauma during the summer or winter months. This pattern has not been previously examined in the literature for populations in northern BC or Canada. It may be assumed that a larger proportion of the population participate in ORA during these seasons as part of vacations or holidays, yet hours of daylight for ORA are significantly limited in the northern winter months. A future comparison of severe injury patterns related to seasonal variation amongst provincial health authorities may help delineate trends specific to the north.
Study Limitations
Various limitations exist within this study. The number of injuries reported during the study period was relatively small, which limited significant statistical analyses due to small cell size. As discussed previously, the data include persons who experienced a trauma; it can raise suspicion about who is at risk for serious injury but with no information about the number of people exposed, incidence and prevalence rates per ORA, which require such a denominator, cannot be accurately determined. Even with a respected and high-quality database such as the BCTR, certain reporting discrepancies and missing data must be taken into account. This study was designed to examine the overall incidence and patterns of injury related to ORA in this population. The subgroup analysis for injuries with an ISS greater than 12 identifies persons at high risk for prolonged complications, permanent sequelae, and impact on health care services, but no outcome criteria related to mortality or morbidity were included, and that is significant when evaluating the long-term effects of these injuries. We must respect that patients presenting with minor injuries who were treated and discharged without hospitalization and persons who died on scene were not evaluated, preventing a comprehensive evaluation of the true incidence of injuries related to ORA.
Conclusions
This project has provided the foundation and direction for future research into the epidemiological spectrum of ORA in northern BC. Our findings emphasize the need for rapid translation of research into injury prevention awareness and programming with a focus on cycling, ATV and snowmobile operation, and horseback riding for populations at highest risk. Further investigation is required to analyze adherence to safety legislation and long-term outcomes for groups who appear at higher risk for injury. Comprehensive prospective data collection will optimize our ability to evaluate injury patterns outside the realm of major trauma and assist our understanding of the overall impact of ORA in northern BC, including social and economic impacts on our stressed health services system.
Footnotes
Acknowledgments
The authors would like to thank the following for their expertise and ongoing support: Ms Dori Williams, Data Analyst with the BC Trauma Registry; Ms Jordan Oliver, Regional Manager for the Northern Trauma Program at the University Hospital of Northern British Columbia; Dr Rhonda Bryce, Research Assistant for the University of Saskatchewan College of Medicine Clinical Research Support Unit; and Dr Hyun J. Lim, Director of the University of Saskatchewan College of Medicine Clinical Research Support Unit.
Presented at the Trauma Association of Canada Scientific Conference, April 12–13, 2012, Toronto, Ontario, Canada.