
Abstract
Introduction
Tree stand falls are a common injury among hunters. This study was designed to identify specific injury patterns and local and regional factors affecting access to and care for this unique trauma cohort in Iowa.
Methods
The University of Iowa trauma registry was retrospectively queried from 2004 to 2014 for patients with a mechanism of injury of fall from tree stands. Data are presented as mean±SD, median, and range, or raw number and percentages as appropriate. Correlation analyses were performed using the Spearman coefficient.
Results
Fifty-three patients were identified. Age was 44±14 (17–78) y. Median fall height was 4.6 m (15 ft), ranging from 1.5 to 12 m (5 to 40 ft). Transport times varied from <1 h to >7 h. Hypothermia was observed in 6 patients (11%). Two patients (4%) tested positive for alcohol. Three patients (6%) tested positive for drugs. Soft tissue injuries (32 [60%]; ie, lacerations and abrasions) were the most common, followed by 30 spine fractures (57%, including 11 lumbar and 10 thoracic fractures), 16 other bone fractures (30%), and 11 rib fractures (21%). Twenty-two patients underwent surgery. Median hospital length of stay was 4 d, ranging from 0 to 20 d.
Conclusions
Tree stand falls lead to significant injuries. Hypothermia represents a significant risk for these patients, and remote location resulted in long transportation time. Improper use or poor condition of safety equipment contributed to falls and injuries in a few of our patients.
Introduction
In geographic regions where whitetail deer hunting is prevalent, falls from tree stands represent the leading cause of hunting-related injuries in the United States. 1 Hunters who fall from tree stands vary widely in age and demographic characteristics. 2 Fall and winter hunting seasons increase the risk of hypothermia, which can complicate traumatic injuries.3,4
From a public health perspective, falls from tree stands are of concern in rural areas where deer hunting is a popular activity in the fall and winter. In Iowa, approximately 171,000 people obtained deer hunting licenses for the 2016 to 2017 season. 5
Deer hunting is most frequently performed from an elevated position in rural areas. Despite the availability of manufactured deer/tree stands, most are often homemade. 6 Their height, stability, and safety equipment vary greatly. The rural setting results in distinct challenges to the patient, the healthcare team members, and the healthcare system.
This retrospective study was designed to identify specific injury patterns associated with falls from elevated tree stands used in hunting as well as other associated injuries or cofactors related to this activity. By predicting common injury patterns, this study may help minimize missed injuries and facilitate appropriate early care for both medical field personnel and receiving facilities. This study may also lead to public safety and prevention announcements to better educate the population of potential risks of injury associated with falls from tree stands.
Methods
Study Design
This retrospective study was approved by the University of Iowa institutional review board. The University of Iowa trauma registry was queried to identify patients who were evaluated by the trauma service for injuries sustained from a tree stand fall during a 10-y period from 2004 to 2014. To effectively identify those patients, the following terms were used for our search: fall, fall from height, fall unspecified, and/or fall from tree stands. The list of patients was reviewed, and only patients who sustained an injury from falling from a tree stand were included. The following variables were collected from the trauma registry: age, race, sex, body mass index (BMI), date/time of injury, date/time arrival to University of Iowa trauma center, body temperature at arrival, height of the fall, list of injuries, injury severity score (ISS), transfer from referring hospital information, and hospital length of stay in days. Medical records were reviewed to collect the following information: the presence of comorbidities, specifically hypertension, smoking, chronic back or joint pain, and the results of the admission toxicology screens. Urine toxicology screening and blood alcohol screening are routinely performed on all trauma patients in our center to detect drug use and intoxication. Blood alcohol level >0.08 g·dL-1, the threshold in Iowa for driving under the influence, was considered indicative of intoxication.
Trauma patients with core body temperatures <36.0°C are considered hypothermic at our trauma center. We used this threshold in this study because it followed existing hospital protocols.
BMI was stratified according to the following scale: normal if BMI was <25.0 kg·m-2, overweight if 25.0 < BMI < 29.9, and obese if ≥30.0. We grouped the patients according to BMI because we speculated that overweight or obese patients might suffer more falls or more severe injuries.
We examined the transfer status of the patients because two-thirds of the patients admitted to our trauma center are transferred from other hospitals. We calculated time from injury to arrival to identify any inordinate delays and whether delays were associated with morbidity.
Data Analysis
Normality was assessed using the Kolmogorov-Smirnov normality test. For continuous variables, normally distributed data are presented as mean±SD and range; non-normally distributed data are presented as median and range. Categorical variable data are presented as number of patients in each category and percentage. Independent t-test, Mann-Whitney U test, correlation, and multivariate logistic regression were performed as appropriate using SPSS 25.0 (IBM SPSS, Chicago, IL), and figures were prepared using the GraphPrism software package (GraphPrism, San Diego, CA). P<0.05 was considered significant.
Results
Patient Demographics
The medical records of 53 patients admitted for a tree stand fall at the University of Iowa trauma center between January 2004 and December 2014 were reviewed for this study. All patients were Caucasian males, except for one. The median age of our population was 44 y and ranged from 17 to 78 y. BMI ranged from 19.0 to 60.2 kg·m−2 with a median of 28.2 kg·m−2; 23 patients (48%) were classified as overweight and 17 (35%) as obese. Thirty-two patients (60%) presented with comorbidities, including hypertension, back/joint pain, cancer, hypothyroidism, and depression. Three patients (6%) were on aspirin and 1 patient was on anticoagulation therapy before the injury. Two patients (4%) were intoxicated at admission (blood alcohol concentration of 0.24 and 0.09 g·dL-1), 7 (13%) were not tested for alcohol use, 1 had a blood alcohol level of 0.07 g·dL-1, and the other 43 cases (81%) tested negative with blood alcohol levels below the 0.01 g·dL-1 limit of detection of the clinical blood test. Similarly, 3 patients (6%) tested positive for drugs, 13 (24%) were not tested, and 37 (70%) tested negative for drugs. One patient tested positive for both alcohol and amphetamine/benzodiazepine. Two patients tested positive for tetrahydrocannabinol.
Injury Characteristics
The median tree stand height was 4.6 m (15 ft), ranging from 1.5 to 12 m (5 to 40 ft). Nineteen patients (36%) fell more than 6 m (20 ft) The median ISS was 9, ranging from 1 to 36. Eleven patients (21%) presented with an ISS of ≥16.
Twenty-nine patients (55%) were transferred from referring hospitals. The time from injury to admission to our center was 2.2±2.9 h, ranging from 21 min to 14 h 28 min for patients who were admitted directly from the scene of the injury. One patient waited more than 14 h before presenting to the emergency department. For transfer patients, the time from injury to presentation to our center was 5.8±2.1 h, ranging from 3 to more than 11 h.
As shown in Figure 1, most patients presented with soft tissue injuries, followed by spine fractures. Of the 30 who sustained spine injuries, 2 had cervical spine injuries, 9 had thoracic spine injuries, 12 had lumbar spine injuries, and 7 had multiple spine injuries. Two thoracic spine injuries were associated with paraplegia and 1 lumbar spine injury featured an incomplete spinal cord injury with a conus medullaris contusion. One patient who had multiple spine injuries developed quadriplegia due to a cervical level spine and spinal cord injury. Only 3 patients had traumatic brain injury because of the fall, and 2 patients had visceral or vascular injuries. Overall, 13 patients (25%) sustained only 1 injury, 19 (36%) had 2 to 3 injuries, and 21 (40%) had 4 or more injuries.
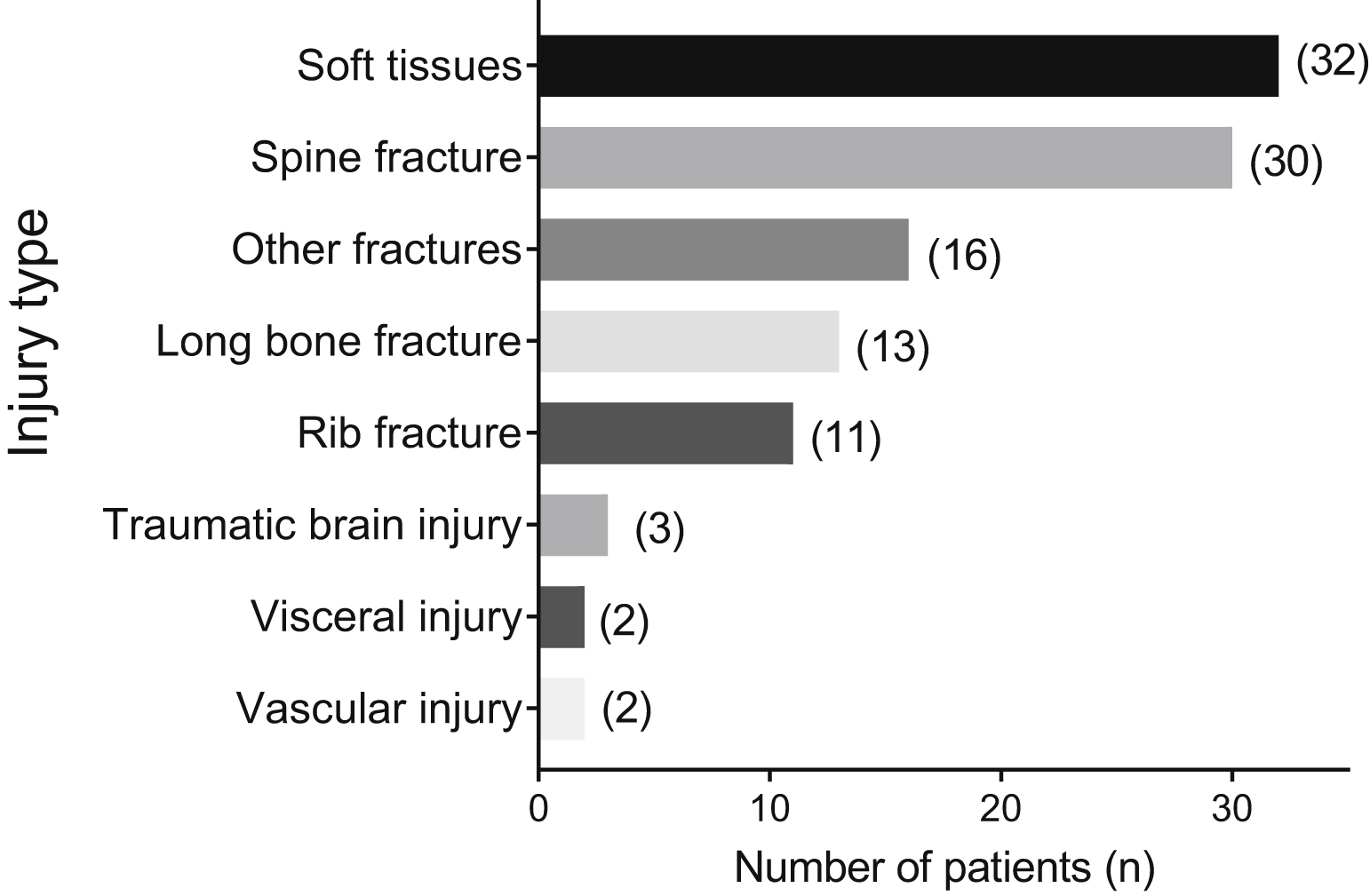
Injury patterns observed in patients admitted for a fall from a tree stand.
Six patients (11%) presented with hypothermia; their body temperature ranged from 34.8 to 36.0°C. Twenty-two (42%) required surgery; 14 (26%) required only 1 surgery, 4 (8%) required 2 surgeries, and the last 4 (8%) required 3 surgeries. Fifteen (68%) patients underwent orthopedic operations, 6 (27%) underwent neurosurgical operations, and 1 was treated by trauma surgery for splenectomy and left chest tube placement as the first surgical intervention. The median hospital length of stay was 4 d, ranging from zero to 20 d, with 35 patients (64%) being hospitalized for 1 to 7 d; 10 patients (19%) did not require admission. No correlation was observed between age, BMI, or fall height and ISS.
In terms of discharge disposition, 41 patients were discharged to home (77%), 8 (15%) were admitted to a rehabilitation facility, 3 (6%) to a skilled nursing facility, and 1 (2%) to an acute care hospital.
Safety Equipment
Information regarding the use of safety equipment was known for only 6 of 53 patients (11%). One patient did not use any safety equipment. Of the 5 patients who reported using safety equipment, 1 used a safety harness, another used a cable, another was hooked to a safety line that broke, and the 2 others used safety restraint equipment that was either rotten or broken.
Discussion
Deer hunting is a popular sport around the United States, especially in rural areas. This unique cohort of patients presents many specific characteristics that are a challenge for the healthcare community. The purpose of this study was to identify common injury patterns among this population and modifiable risk factors that increase injury severity and morbidity. Our data show that most of the patients were male, which reflects the deer hunter demographic in Iowa. In this state, most deer hunting licenses were sold to men (93%) with an average age of 41 y. 7 Most patients (75%) admitted at the University of Iowa after a fall from a tree stand fell from a height of 3 m (11 ft) and higher; about one-third (36%) were admitted for injuries due to a fall from a height of 6 m (20 ft). In addition, the time from injury to admission to our center varied greatly, with some patients presenting more than 5 h after injury. These data reflect the rural nature of this sport, which is practiced in remote areas, making access to tertiary healthcare difficult. Additionally, 55% of the patients were transferred from referring hospitals, increasing the time between injury and admission at the definitive care facility.
Although alcohol is a known risk factor for injuries from accidental falls, 8 only 6% of our population tested positive for alcohol at admission. The rate of intoxication in our population is similar to rates of 2 to 7% reported previously. 9 –11 This low percentage may be explained by the fact that alcohol blood levels may have decreased during the time between injury and admission; this period was highly variable owing to transportation time and/or transfer from a referring hospital. It might also be low because all Iowa hunters receive injury prevention education as part of the class required before getting a hunter’s license. The injury prevention education includes the risks associated with the consumption of drugs and alcohol while hunting.
Common injury patterns were different from those previously reported.12,13 In our cohort, soft tissue injuries were the most common injuries reported, followed by spine fractures. Long bone fractures and closed head injuries were less common in our study than in previous studies.12,13
Length of hospital stay in this study was similar to that described previously12,13 and correlated with the ISS. In our series, however, there was no correlation between fall height and ISS. A prior study from another institution reported a positive correlation between those variables. 13
Because deer hunting is an outdoor sport practiced during the fall and winter, deer hunters are likely to face extreme cold and harsh weather conditions, especially in the Midwest. Such conditions may affect the patient’s body temperature. Our data indicated that 12% of the patients admitted had mild hypothermia. 14 Hypothermia is a risk for trauma patients and may lead to complications that can be lethal.14,15
Finally, the use of safety equipment was only reported for 6 patients (11%). We do not know how many patients in the unreported group used proper safety equipment. Furthermore, we did not collect any information about the tree stand manufacture or installation factors that might contribute to stand failure and resulting falls. Manufactured deer/tree stands are available in many designs by many producers. They are rigorously tested and provided with safety equipment. Some hunters, however, build their own stands. 6 We do not know if homemade stands fail more often than manufactured stands. Stand height, stability, and safety equipment vary greatly. 6 In our population, the use of safety equipment was poorly documented. Although tree stand fall-related injuries have been shown to be partly attributed to failure to appropriately use safety harnesses, 16 the infrequent use of safety equipment among deer hunters has been previously described.9,11,17,18 Taken together, these data suggest a need for improvement in capturing information regarding the use of safety equipment. Although the Iowa Department of Natural Resources has information on tree stand safety, 19 education on the use of safety harnesses to prevent falls from tree stands should be provided to all hunters. 20
Our study has several limitations, including its small sample size. First, the data were acquired through retrospective chart review, which introduces a risk of bias stemming from poor documentation or missing data. Second, only a few patients reported using safety or protective devices. As indicated, we do not know how many patients did, in fact, use proper safety equipment, making it difficult to draw any definitive conclusions. In addition, most of our patients were tested for alcohol use on admission, and a large proportion tested negative with blood alcohol levels below the detection limit. However, regardless of transfer from referring hospitals, the median time from injury to admission was 3.5 h, making it difficult to draw any conclusions regarding whether patients were under the influence at the time of the fall. Furthermore, tree stand height was self-reported and is most likely an approximation. Moreover, the type of surface onto which the patients fell, which may also have affected injury severity, was unknown. Finally, we believe that only the most severely injured patients presented to the hospital. Many individuals who fall from tree stands probably do not seek medical attention or remain at local hospitals because of minor injuries. Despite those limitations, our study provides useful information on the type of injuries incurred from tree stand falls.
Conclusions
Our study highlights that falls from tree stands lead to significant injuries in Iowa. Deer hunting in remote locations resulted in long transportation times to definitive care. Failure of safety harnesses when assessed was a contributing factor to falls and injuries in a few patients, but not all. Finally, there was low incidence of alcohol and drug intoxication, which may reflect injury prevention aspects of the required hunter education classes.
Footnotes
Acknowledgements
Author Contributions: Study conception and design (TSG, MG, DAS); acquisition of data (MG, CG, ML); analysis and interpretation of data (CG, TSG, MG, ML, DAS); drafting of manuscript (CG, MG, DAS, TSG); critical revision (TSG, CG, ML, DAS); final approval of manuscript (MG, CG, MAL, DAS, TSG).
Financial/Material Support: None.
Disclosures: None.