
Abstract
Wild boar attacks have rarely been reported in the medical literature. This is the case of an 83-year-old male farmer who was assaulted from behind by an injured adult wild boar. He presented with hemorrhagic shock after sustaining injuries to the right profunda femoris artery and right sciatic nerve as well as significant soft-tissue injuries, bilateral iliac wing fractures, an open pneumothorax, and an anorectal injury. The anorectal injury was treated with fecal diversion but was complicated by soft-tissue infection in the surrounding dead space. The patient needed multiple operations, including removal of the distal rectum and creation of a permanent colostomy. In this report, we highlighted the characteristics of anorectal trauma caused by a wild boar attack. We conclude that penetrating anorectal injuries caused by this type of attack can be associated with extensive soft-tissue damage despite externally appearing to be simple puncture wounds. Anorectal combat injuries have demonstrated similar extensive surrounding soft-tissue injuries and propensity for infection; therefore, this case supports adopting a similar treatment strategy, that of serial and radical debridement, to treat certain wild boar injuries.
Introduction
The wild boar (Sus scrofa) is a species with an abundant population in most parts of Eurasia. It has been introduced into areas such as North America and Australia. A wild boar has higher motor performance than one might realize, as well as potentially dangerous features. Adult boars usually weigh up to 90 kg, but individual boars weighing over 100 kg have been reported. Boars can run as fast as 40 km·h-1, can jump over a 1 m fence, can lift an object of over 30 kg using their nose, and have sharp tusks over 10 cm long.1,2 Mayer reported that wild boar attacks, as described primarily in the popular literature, have been increasing in developed areas since the mid-1990s. 3
In Japan, according to the Ministry of the Environment, wild boar habitat increased by 70% between 1978 and 2014. The report also mentioned that wild boar hunters have been aging and their numbers have been decreasing over the years in Japan, thus leading to lower pressure from hunting on the wild boar population. 4 This situation has been even worse in the Fukushima prefecture following the earthquake/tsunami-induced meltdown of the Fukushima Dai-ichi nuclear plant in 2011. Commercial trade and consumption of local boar meat has been banned because of high radiodensity in the wild boar caught in the area. 5 –7 This discourages hunting and, consequently, makes it more difficult to control overgrowth of the wild boar population in the area. 8
These changes have affected the incidence of human−wild boar conflict. The local government of Kobe city, which is located in the western part of Japan, has reported wild boar–induced injuries annually, with a drastic increase in these injuries after 2010 (1.7 per year for 2007–2010; 41.6 per year for 2011–2014). 9 Some fatalities and severe injuries have been reported in Japanese mass media after 2000. 10 Responding to the increase in public interest, the Ministry of the Environment commenced maintaining nationwide statistics about wild boar attacks beginning in 2016.
Despite these facts, cases of wild boar injuries have rarely been published in the medical literature, and only a few fatal and nonfatal cases have been reported. 10 –17 In this report, we describe the case of a nearly fatal wild boar assault with multiple traumas, including anorectal injury, that occurred in Fukushima prefecture. Our case appears to be one of only a few reported cases of survival after a severe wild boar injury—defined as any internal organ injuries or life-threatening external bleeding 10 —and the first case of anorectal injury caused by a wild boar attack.
Case presentation
An 83-year-old male farmer was attacked from behind by a male adult wild boar while working on his farmland located in the southeastern part of Fukushima prefecture, approximately 150 km north of Tokyo. The boar had been injured by a hunting trap. Emergency medical personnel noticed multiple penetrating wounds and active external bleeding in the right posterior thigh, but the exact bleeding vessels could not be identified in the prehospital setting. The patient underwent volume resuscitation with crystalloids started during transportation to the hospital. He was brought to our emergency department by air ambulance. His initial vital signs were as follows: systolic blood pressure of 65 mm Hg, a heart rate of 68 beats·min-1, and a respiratory rate of 28 breaths·min-1. It was impossible to obtain a blood oxygen saturation level with a pulse oximeter because of poor peripheral perfusion. The patient also appeared confused and agitated. Physical examination showed multiple penetrating wounds to his legs; a 3 cm long wound located at the sixth intercostal space in the right anterior chest wall, which reached the intrathoracic space; a degloving injury of his buttock and right posterior thighs; active bleeding from a deep laceration in the right posterior thigh; and a deep perineal wound passing into the anal canal and distal rectum (Figure 1). He was unable to dorsiflex his right ankle and toes, indicating partial sciatic nerve palsy. Initial imaging studies showed a right open pneumothorax, bilateral undisplaced iliac wing fractures, and multiple air bubbles around the rectum as seen by a computed tomography scan, which indicated anorectal injury. Computed tomography also showed a high-density foreign body in his right buttock (Figure 2).

Photograph of the patient upon arrival. Note the multiple wounds in the buttock and the bleeding from the perineum.
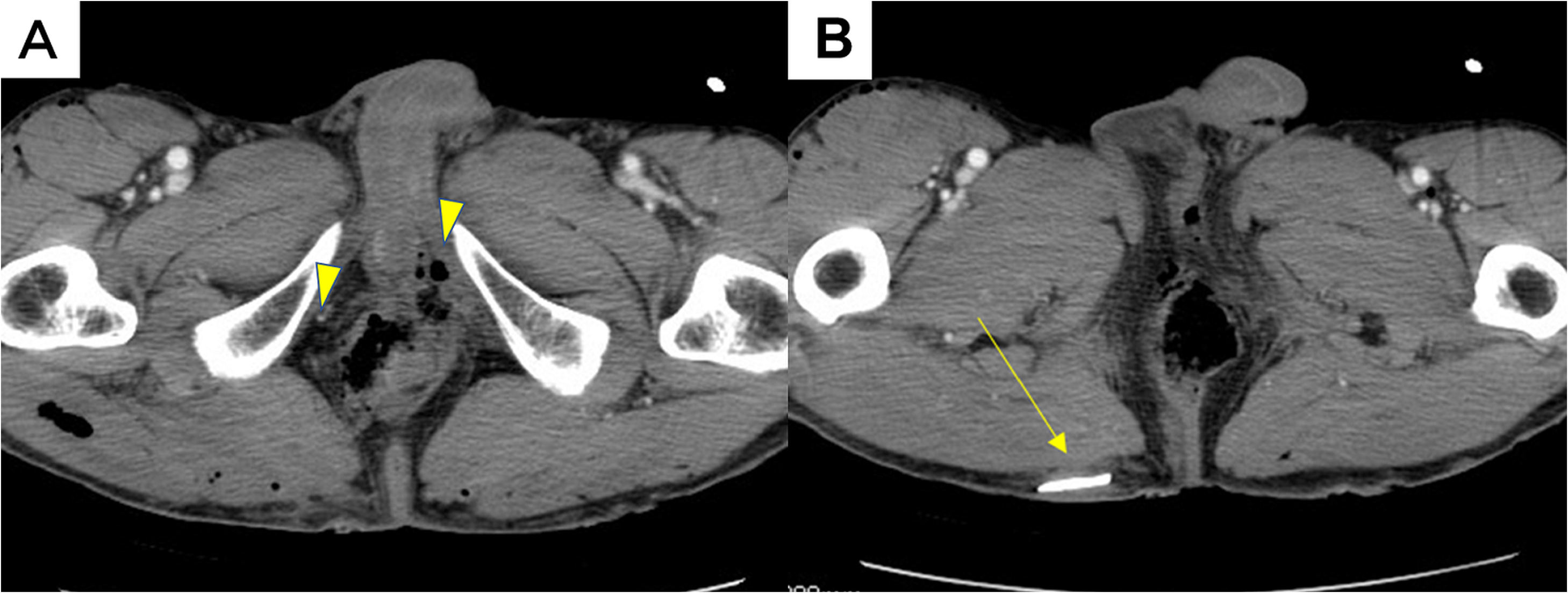
A, Computed tomography scan at the level of the rectum showing free air bubbles around the rectum (arrowheads). B, Another image, which shows a tusk remaining in the subcutaneous layer of the right buttock (arrow).
Because of its uncontrollable aggressiveness, the attacking animal was caught and killed by local hunters 3 h after the incident and was identified through the observation of a broken tusk.
The patient showed no significant change in hemodynamic variables after 2000 mL of crystalloids were administered, and he was diagnosed with hemorrhagic shock. Blood product infusion was initiated as soon as the patient was determined to be unresponsive. During the primary survey, the patient was intubated in the emergency department due to prolonged poor oxygenation, and pneumothorax was treated with thoracostomy tube insertion through a newly created incision and simple wound closure. His iliac fractures were considered stable and treated conservatively. An emergency operation was performed. Active bleeding from his transected right profunda femoris artery was observed, which was controlled with a ligation. His right sciatic nerve was partially lacerated and directly repaired with sutures (see online Supplemental Material 1). The degloving wound in his buttock and thigh was debrided and closed with suction drainage. A piece of the wild boar’s tusk was found in one of the wounds and removed (see online Supplemental Material 2). Complex full-thickness lacerations in his anal canal and distal extraperitoneal rectum were confirmed: One laceration was located in the left lateral wall, and another was located from the mid-posterior to the right lateral wall (see online Supplemental Material 3). The distal rectal and anal canal walls appeared impossible to repair directly. Fecal diversion with a temporary proximal colostomy was performed, and the patient was stabilized and admitted to the intensive care unit. Intravenous ampicillin/sulbactam (ampicillin 2000 mg and sulbactam 1000 mg every 6 h) was started prophylactically, targeting the animal’s oral flora as well as human enterobacteria. Tetanus toxoid and human tetanus immunoglobulin (250 IU) were also administered.
On the fifth day, the patient was extubated and discharged from the intensive care unit. The degloving wound around his perineal area became infected because of uncontrolled contamination with mucus secretion from the distal blind stump of his rectum. The patient underwent removal of the distal rectal remnant and creation of a permanent colostomy on the 13th day. A rotation skin flap was created on the 32nd day to cover the debrided wound. After rehabilitation, he was discharged on the 114th day with residual partial sciatic nerve palsy and a permanent colostomy.
Discussion
Wildlife attacks are not common in developed countries. Although commonly reported attackers are carnivores, such as bears or wolves, several reports highlight injuries caused by noncarnivorous animals.18,19 Regarding carnivore attack cases, Penteriani et al 20 reported that high-risk human behavior, including leaving children unattended, the presence of a dog, and approaching wounded animals while hunting, triggered the attacks in over 50% of cases. In our case, the boar had been injured by a hunting trap. Some reported cases of wild boar attacks had triggers similar to those of carnivore attacks.3,16 Most people do not realize which situations are highly likely to trigger an attack. Therefore, public health actions to increase public awareness about the potential dangers of wildlife encounters and knowledge about injury prevention should be implemented in high-risk areas.
Reports of wild boar attacks in the medical literature have been surprisingly sparse despite increasing reports in mass media. In fact, we found only 8 reports on 14 patients in the English literature. 10 –17 According to these reports, wild boars have a typical attack pattern that leads to unique localization of the injuries. In typical cases, boars first charge, then bite their victims and gouge them with their tusks. 16 Victims commonly sustain multiple wounds to the posterior thighs: An adult boar’s head can be located as high as 70–80 cm, at approximately the level of the thighs of an adult human. Moreover, victims are often attacked from behind while trying to run away from an attacking boar. 3 ,14,15 This was the case with our patient. Tumram et al reported a patient who had a fatal arterial injury caused by a wild boar’s tusk impaling his thigh. 14 Nagasawa et al summarized wild boar attacks previously reported in Japanese mass media and reported that thigh or leg wounds were the main wound site in 3 of the 4 fatal cases. 10 We suppose that these causalities were likely to have included vascular injuries. Our patient had a transection of the profunda femoris artery, which led to his near-fatal hemorrhage. We believe that leg injuries caused by wild boars can be fatal even if the lacerations are located only in the posterior thigh with the major organs remaining intact, especially when the penetration is deep enough to reach major vasculature. Considering that wildlife attacks most commonly occur in rural areas and that vascular injuries need prompt intervention, we believe air transportation has significant advantages over ground transportation in cases of patients severely injured by wild boar attacks.
In our case, intravenous ampicillin/sulbactam was given prophylactically to cover both human enterobacteria and the animal’s oral flora. For elective colon procedures, second-generation cephalosporins with both aerobic and anaerobic activities (cefoxitin or cefotetan) or cefazolin plus metronidazole is usually recommended to cover pathogenic enterobacteria inhabiting the human lower gastrointestinal tract. Alternative regimens include ceftriaxone plus metronidazole and ampicillin/sulbactam. 21 Although data about a wild boar’s normal oral flora are lacking, Barnham studied wound infection after domestic pig bites. 22 The isolated organisms included Streptococcus agalactiae, Streptococcus dysgalactiae, Streptococcus suis, Pasteurella aerogenes, Proteus species, Escherichia coli, Bacteroides species, Pasteurella multocida, and coagulase-negative Staphylococcus. In previous case reports of wild boar bite wounds, amoxicillin/clavulanic acid was administered in 4 cases 10 ,13,15,16; other regimens included intramuscular penicillin plus metronidazole, ciprofloxacin plus clindamycin, and cefuroxime plus metronidazole. 16 Each regimen was used in just a single case. Of these 8 cases, only 1, with amoxicillin/clavulanic acid administration, was complicated by wound infection. 10 Our patient experienced deep wound infection even with prophylactic antibiotic use; however, we believe this infection was caused primarily by poor control of contamination and the fact that antibiotic use never outweighs proper wound management.
Historically, the management of penetrating anorectal trauma has been described using the “4 Ds”: diversion of feces, distal rectal washout, drainage of the presacral area, and direct repair of the injury. 23 However, due to the rarity and variety of these injuries, the indications for use of each technique remain controversial, and many authors have recommended a case-by-case approach to their management. 24 –27 Anorectal injury rarely occurs as a result of animal attacks. To date, there have only been 2 reports of bull-horn anorectal penetrating trauma.28,29 One patient was treated only with primary suturing, whereas the other required a temporary colostomy; perineal wounds healed uneventfully in both cases. No report can be found about anorectal injuries caused by other animals.
Our patient had a degloving injury close to the perianal area, and there might have been a direct communication between the degloving wound and the anorectal laceration. Therefore, controlling contamination of the large dead space was difficult, and the patient eventually underwent removal of the distal rectal remnant and creation of a permanent colostomy. Wounds from wild boar attacks are not simple stabbing lacerations because boars do not just bite but also pull and tear tissue during the attack. Thus, the wounds can be deep, contaminated crush wounds associated with large dead spaces and devitalized tissues, which are common characteristics of combat soft tissue injuries. 30 Glasgow et al analyzed 46 combat anal traumas, in which 76% of casualties occurred from blast injury and 6 patients required complete rectal and anal sphincter resections, as did our patient. 26 The reasons for these procedures were unrepairable massive wounds in 4 patients and uncontrolled infection in 2 patients. Moreover, it is noteworthy that reconstruction of the anal sphincter and complete wound closure, which might have led to inadequate debridement, were attempted in those 2 infection cases. 26 The authors have recommended serial radical debridement of nonviable tissue for complex perineal wounds to treat battlefield anorectal injuries. In situations similar to our case, as with combat trauma, we also believe that planned second-look surgery should be considered as well as radical debridement, and early consultation with reconstruction surgeons who have expertise in flap surgery should be mandatory to minimize the risk of subsequent infection.
Finally, this wildlife population can be indirectly attributed to the recent nuclear disaster, which significantly decreased human pressure in the affected area. Thus, it should be remembered that mass disasters, which can alter human activity in an area for a long time, may also affect the incidence of wildlife-related health issues.
Conclusions
We have reported the case of a patient with multiple traumas, including anorectal injury, caused by a wild boar. The lesson learned from our case is that wild boar–induced penetrating anorectal injury can be associated with more extensive soft-tissue damage than simple stabbing or impalement. Physicians should, therefore, evaluate soft-tissue damage carefully and consider serial and radical debridement because of the substantially high infection risk.
Author Contributions: Conceptualized, collected data, and prepared the article (IO); collected data and prepared the article (MY, NK); critically revised the article (YW, TSu, TM, NM); critically revised the article and gave the final approval (KS, TS, KI).
Financial/Material Support: None.
Disclosures: None.
Footnotes
Supplemental Material
Supplemental material associated with this article can be found in the online version at
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.