
Abstract
Objective
Bouldering is a type of rock climbing in which the climber ascends small boulders with pads and spotters in lieu of ropes, with an emphasis on ascending the most difficult surface possible. We sought to investigate the prevalence and incidence of injuries, and we hypothesized boulderers who enlisted preventative measures and those who bouldered indoors would have fewer injuries.
Methods
This cross-sectional cohort study assessed incidence and pattern of injury among indoor and outdoor boulderers over 1 year.
Results
Spotting other boulderers resulted in few injuries, but both climbing and falling were associated with diffuse injuries. Finger and ankle injuries were common. Traditional preventative measures were ineffective, and there were few differences between indoor and outdoor boulderers.
Conclusions
Bouldering outdoors has an increased risk of injury to the fingers. Preventative measures appear largely ineffective in reducing the number of injuries in both cohorts.
Keywords
Introduction
Bouldering is a sport intimately related to rock climbing. Climbing sports can be conceptualized as having 2 different athletic goals: 1) successful ascent to a summit or 2) the gymnastic act of climbing itself. Athletes involved in bouldering focus completely on the latter to move over the most difficult section of rock possible. This is accomplished on boulders near to the ground, obviating the need for ropes and harnesses to catch a falling climber. Instead, the boulderer climbs above a specialized portable pad and is spotted very similarly to a gymnast (Figure 1). Therefore, a boulderer repeatedly attempts a short difficult section of rock, which is generally 8 to 15 feet high. It can take the boulderer anywhere from hours to years to successfully solve this mini-climb or “boulder problem.” The boulderer repetitively attempts the sequence of climbing moves to create muscle memory, build strength, and improve efficiency of movement required for successful ascent. Although bouldering had modest beginnings circa the 1950s, the sport has exploded in popularity with specialized equipment, companies devoted to bouldering gear, boulder route guidebooks, professional bouldering guides, and restrictions to bouldering areas because of excessive demand.
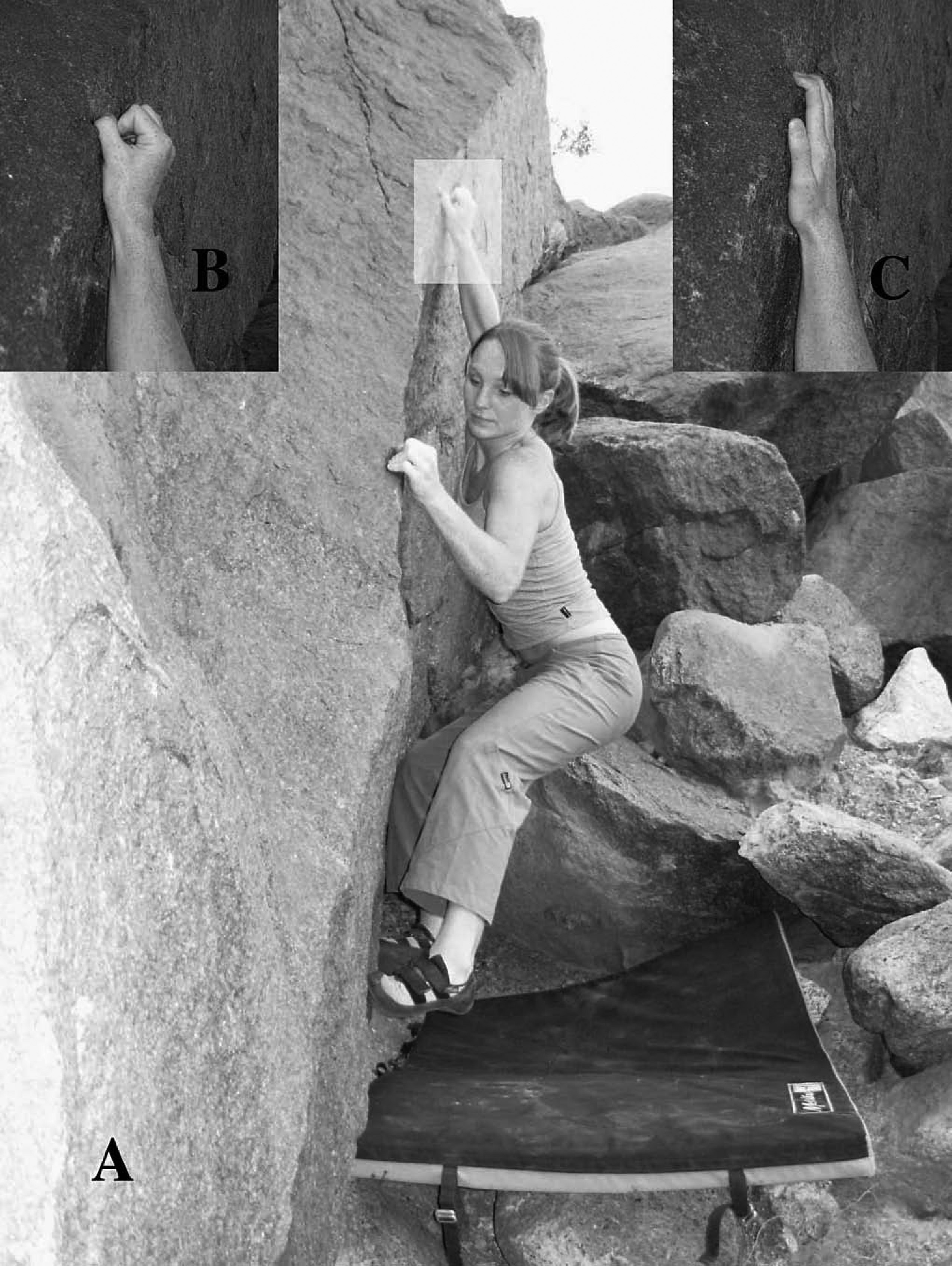
A. Typical bouldering layout with subject attempting problem above pad, spotter outside of photo; B. typical crimp grip; C. typical slope grip.
As the number of people climbing recreationally has increased from 7.3 million to 9.2 million over the last decade, 1 investigators have begun to study the inherent danger of the sport, common injury patterns, and the use and efficacy of safety equipment. Despite this nascent attention to the epidemiological aspects of climbing, bouldering has been neglected. Unfortunately, there is reason to doubt that findings related to rock climbing are generalizable to bouldering. First, bouldering involves serial repetitive movements, which are typically more strenuous and powerful than traditional rock climbing. This “vertical sprinting” could exact a greater toll on connective tissue. If this is true, athletes could be at increased risk of overuse syndromes previously described in rock climbing. 2 Second, bouldering involves 3 different activities during which the boulderer can sustain injury: 1) climbing the boulder, 2) falling, or 3) spotting others bouldering.
Despite its popularity and differentiation from rock climbing, there is little evidence to support an understanding of bouldering injuries. Although some injuries might overlap with other climbing forms, previous studies have either not directly addressed bouldering or excluded bouldering altogether.
2
–8 Several artificial models Schematic of crimp grip with flexor tendon (arrow), tendon pulleys depicted by solid black ovals and labeled A1–5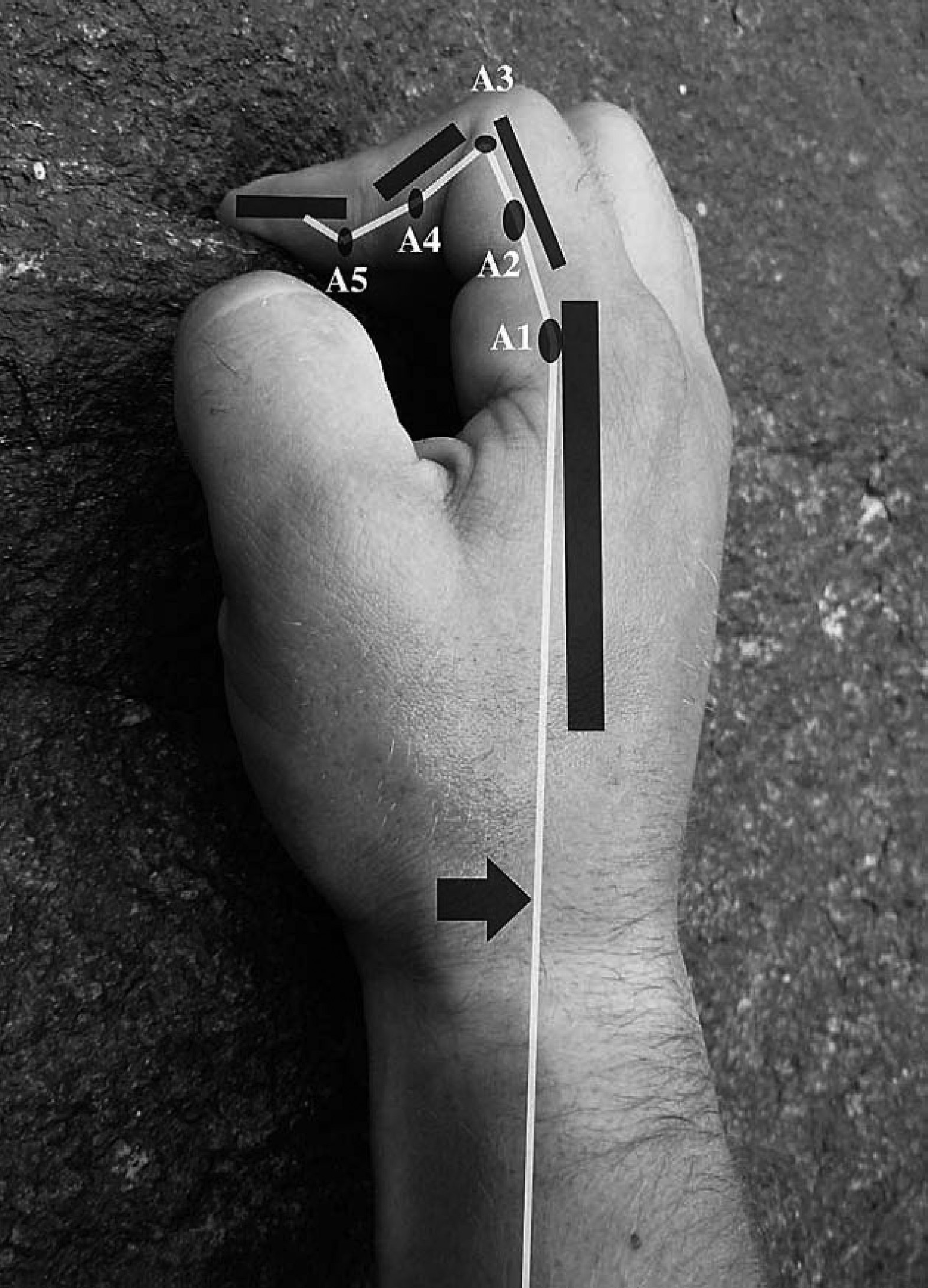
The purposes of this inquiry were 1) to determine the incidence and prevalence of bouldering injuries sustained during the 3 activities involved in the sport (climbing boulders, falling, and spotting other climbers), 2) to describe patterns of injury, 3) to analyze injury prevention strategies and their frequency of use, and 4) to compare injuries and prevention strategies between indoor and outdoor boulderers.
Methods
Study Design
This prospective study consisted of 2 phases. The first involved a survey to evaluate characteristics of a cross section of athletes participating in the sport of bouldering indoors and outdoors (Appendix 1, initial survey, available at wemjournal.org). The second phase followed 2 cohorts of boulderers (those recruited indoors and outdoors) to assess their experience and injuries over a period of 12 months. A follow-up internet survey (encrypted to protect subject personal and health information) assessed new injuries and use of injury prevention techniques during the 12-month study period.
Study Setting and Population
The authors recruited consecutive volunteers who were actively bouldering in 12 popular bouldering areas throughout North America. These areas included: Moab, UT; Joe's Valley, UT, Triassic, UT; Red Rocks, NV; Joshua Tree, CA; Corona Del Mar, CA; Yosemite Valley, CA; Tuolomne Meadows, CA; Happy Boulders, CA; Sad Boulders, CA; Buttermilks, CA; and Squamish, British Columbia, Canada. These areas involved a large range of rock type, boulder size, and difficulty. Surveys were conducted from October 1 to November 30, 2004. During the same period of time, subjects were enrolled from another population in an identical manner from the bouldering area of a rock climbing gym in Saint Paul, MN. This group came from an area with limited nearby outdoor bouldering where the sport is practiced almost exclusively in indoor facilities with artificial rock. Bouldering areas in the gym had gymnastic-type padded floors and supplied additional mobile bouldering pads.
Questionnaire Development and Validation
The initial questionnaire was developed from the existing literature on rock climbing. 2 –8 The instrument was refined by consensus from 5 experienced boulderers. The instrument was further refined for validity via consultation with 3 experienced clinical researchers. This proposed survey instrument was piloted among active boulderers who were then interviewed in person and asked to comment on the questionnaire items. The instrument was refined on the basis of their suggestions and retested until changes were no longer being suggested (a total of 14 cognitive interviews each with different athletes). 1
Measurements
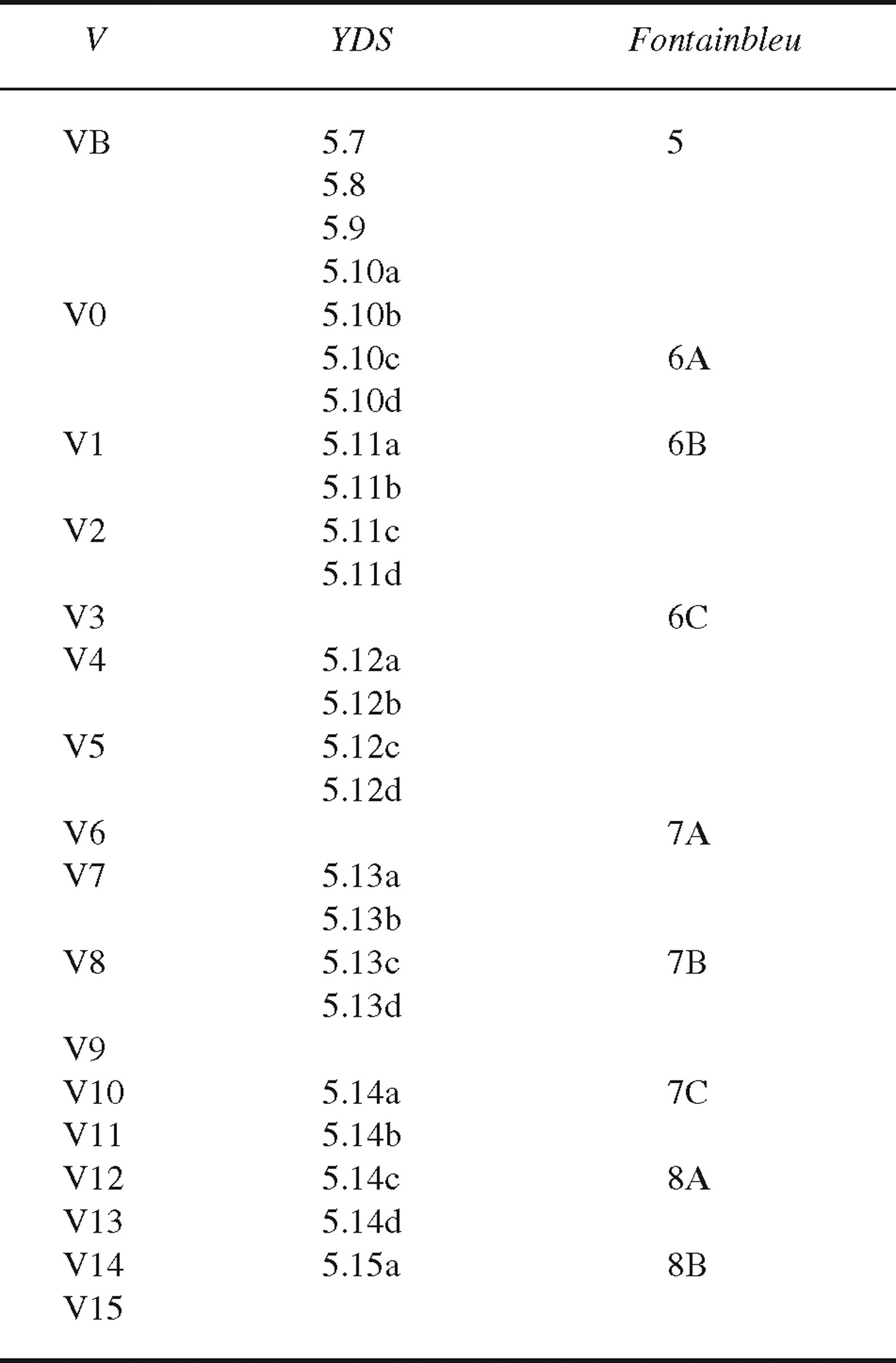
The questionnaire addressed injury by body part [yes/ no] and the activity during which each injury occurred— specifically, climbing, falling, or spotting others. Potential risk factors that were hypothesized to contribute to injury risk were also investigated. These risk factors included gender, height, weight, body mass index (BMI), age, years of bouldering experience, use of preventative measures, presence of previous injuries, and ability level. Ability level was determined on the basis of the nationally recognized bouldering difficulty scale grading boulder problems from V1 to V15 (Table 1).
Comparison of 3 systems for rating difficulty of rock climbing and bouldering: the Bouldering V scale (V), the Yo semite Decimal System (YDS), and the French Fountainbleu System (adapted from
Outcome Measures
Injuries during the 12 months of study were the primary outcome measures. These injuries were divided by anatomical location and by the activity during which they occurred—specifically, while climbing the boulder, while falling and striking the ground or pad, or while spotting another bouldering athlete.
Study Protocol
Athletes bouldering indoors and outdoors were approached consecutively, informed about the study, and offered enrollment. No compensation was offered to subjects. In addition to the written survey, subjects were questioned further about any injury they indicated on the questionnaire. In recruiting potential subjects, informed consent occurred with an explanation of the study's purpose, confidentiality, and voluntary participation. Subjects who completed a survey were asked for an e-mail address for follow-up survey participation (Appendix 2 Appendix 2 Cont., follow-up survey, available at wemjournal.org). This follow-up survey was administered via the internet and evaluated the incidence of injuries, the pattern of bouldering injuries, and the use of preventative measures during the year of study. Institutional Review Board approval was obtained.
Statistical Analysis
The descriptive statistics of patterns of injuries are presented. Relationship of preventative measures, habits, and baseline characteristics of the study population to injuries was measured with Fisher exact test to account for small cell size, with alpha <.05 considered statistically significant. Results in the tables are based on analyses of the proportions so that approximate confidence intervals can be displayed. All analyses were performed by Stata 9.2/SE (Stat Corp., College Station, TX).
Results
Enrollment and Population Characteristics
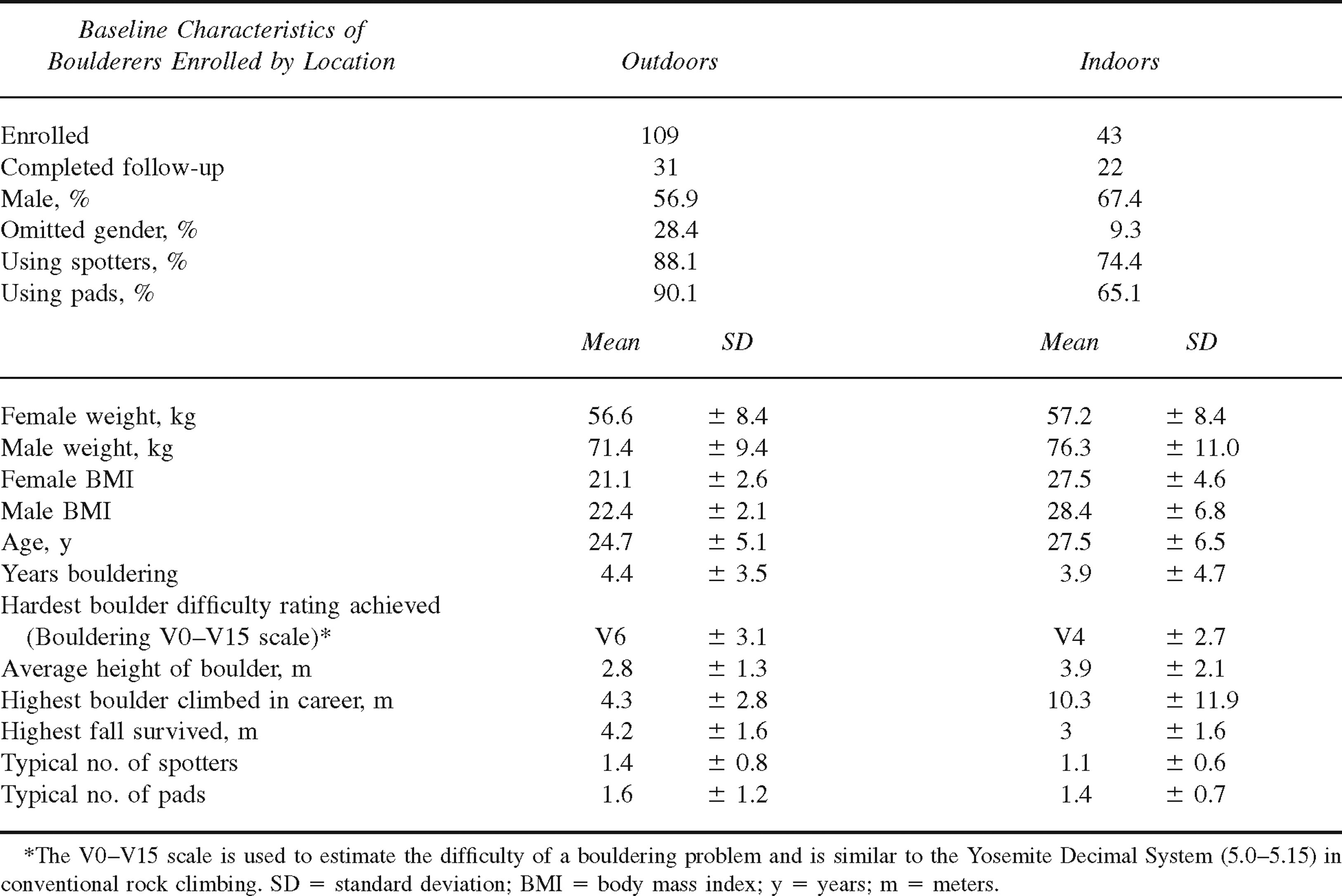
Outdoors, a total of 113 individuals were approached for the study, with 109 (96%) persons enrolling in the study, of whom 100 (92% of participants) supplied an e-mail address for follow-up and 31 completed the 1-year follow-up study for a 1-year participation rate of 28%. Indoors, 48 individuals were approached, 43 (90%) elected to be enrolled, 40 (93% of participants) provided e-mail addresses, and 22 (51%) completed the 1-year follow-up study. The population was generally young with an average age of 25 ± 5 years and an average experience level of 4 ± 4 years (Table 2). The population enrolled outdoors averaged a higher level of self-assessed ability (V6 vs V4 indoor).
Baseline characteristics of boulderers on the basis of outdoor compared with indoor bouldering locations
Incidence
The incidence of climbing injuries is depicted in Table 3. Of note, climbers in the outdoor cohort injured their fingers more often than those in the indoor cohort (19 [61%] vs 6 [27%]; 95% CI for risk difference −10 to −3). This was the most common injury, and, during the study, injuries were associated with a history of previous finger injury (odds ratio 4.0; 95% CI 1.2–13.6; p = .03) but were unrelated to other variables measured, including gender, years of climbing experience, BMI, or weight. Other common injuries sustained during the study included injuries to the shoulder (8 [26%] outside vs 8 [36%] inside, 95% CI −20 to −41) and to the elbow (8 [26%] outside vs 6 [27%] inside; 95% CI −27 to 30).
Incidence of injury by activity to bouldering athletes enrolled indoors and outdoors
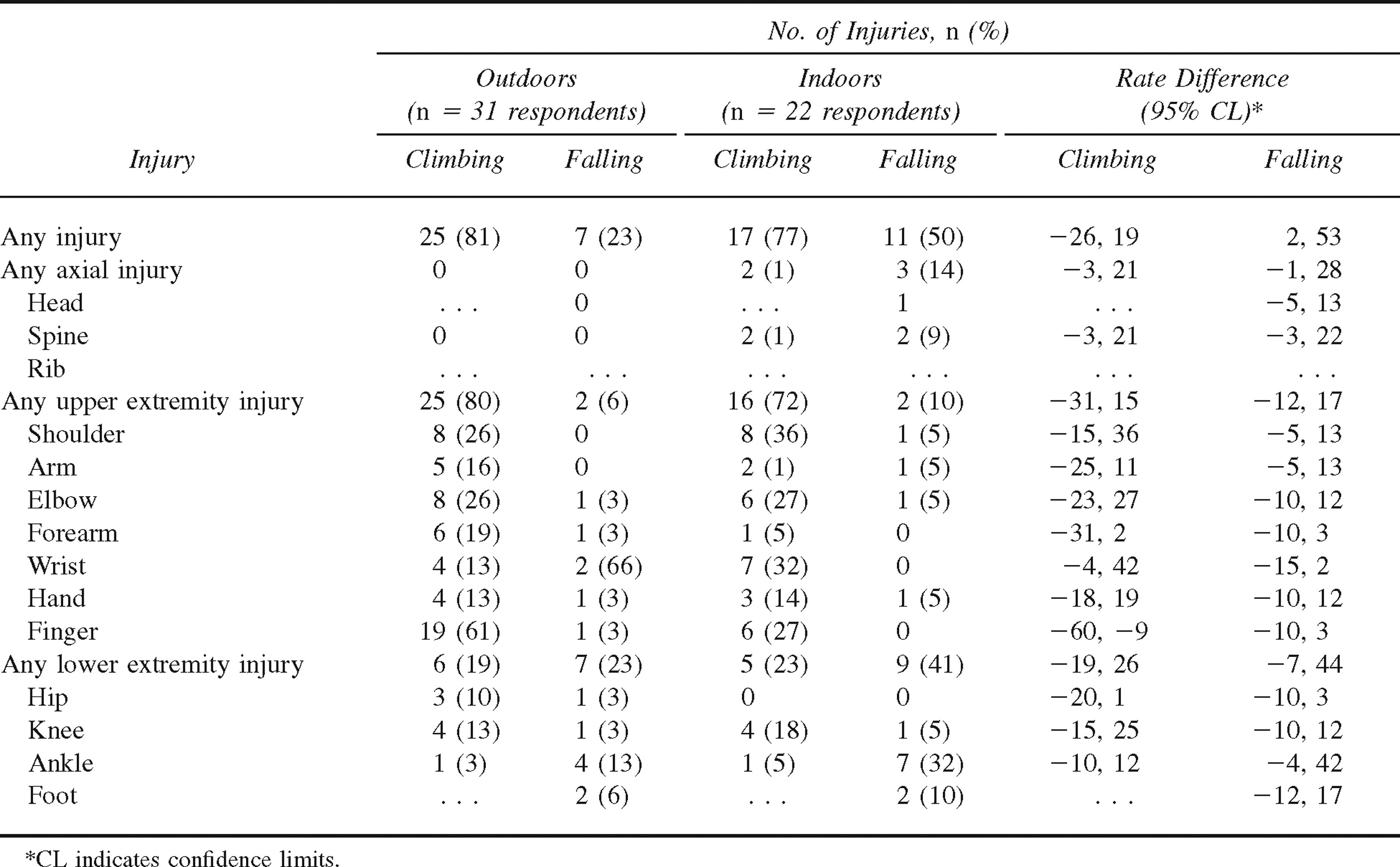
We considered that one possible explanation for the differences in finger injuries was the higher self-assessed ability level in the outside cohort. To explore this possibility, we used a logistic regression. Specifically, we used finger injury regressed on location of climbing and ability, with all location and ability interaction effects included. Additionally, we examined the association of finger injury with ability. The results indicated that the differences in injury rates were independent of other factors. Neither ability nor the interaction effects of ability with location were statistically or clinically significant.
During the 12 months of the study, injuries sustained while falling were less common in the outdoors cohort vs indoors (7 [23%] vs 11 [50%]; 95% CI 2 to −53). However, the incidence of specific injuries did not differ among cohorts. The most common locations included the ankle (4 [13%] outside vs 7 [32%] indoor; 95% CI −8 to 46), and the foot (2 [6%] vs 2 [10%]; 95% CI −13 to 18). The incidence of these injuries was unrelated to use of spotters, number of spotters, height of average boulder, height of tallest boulder climbed, use of pads, number of pads, gender, years climbing, BMI, weight, or ability level. Spotting injury incidence was very low both indoors (2 [6%] and outdoors 1 [5%]).
Prevalence
The career prevalence of injuries sustained while climbing is depicted in Table 4. The finger was the most commonly injured area, with 73 injuries outdoors (67% of cohort) vs 25 (58%) indoors (95% CI −3 to 1). Other areas commonly injured were the elbow (42 [39%] outside vs 18 [42%] inside; 95% CI −14 to 21) and the shoulder (44 [40%] vs 16 [37%]; 95% CI −20 to 14]. The prevalence of these injuries was unrelated to gender, years climbing, BMI, weight, or ability level, and none of these differences were statistically significant. The ratio of career finger injuries to all other injuries was 1: 3.2 (n = 73:235) outside for the 109 participants and 1: 3.7 (n = 25:93) inside for 43 participants.
Prevalence of career injuries sustained by activity by location of bouldering
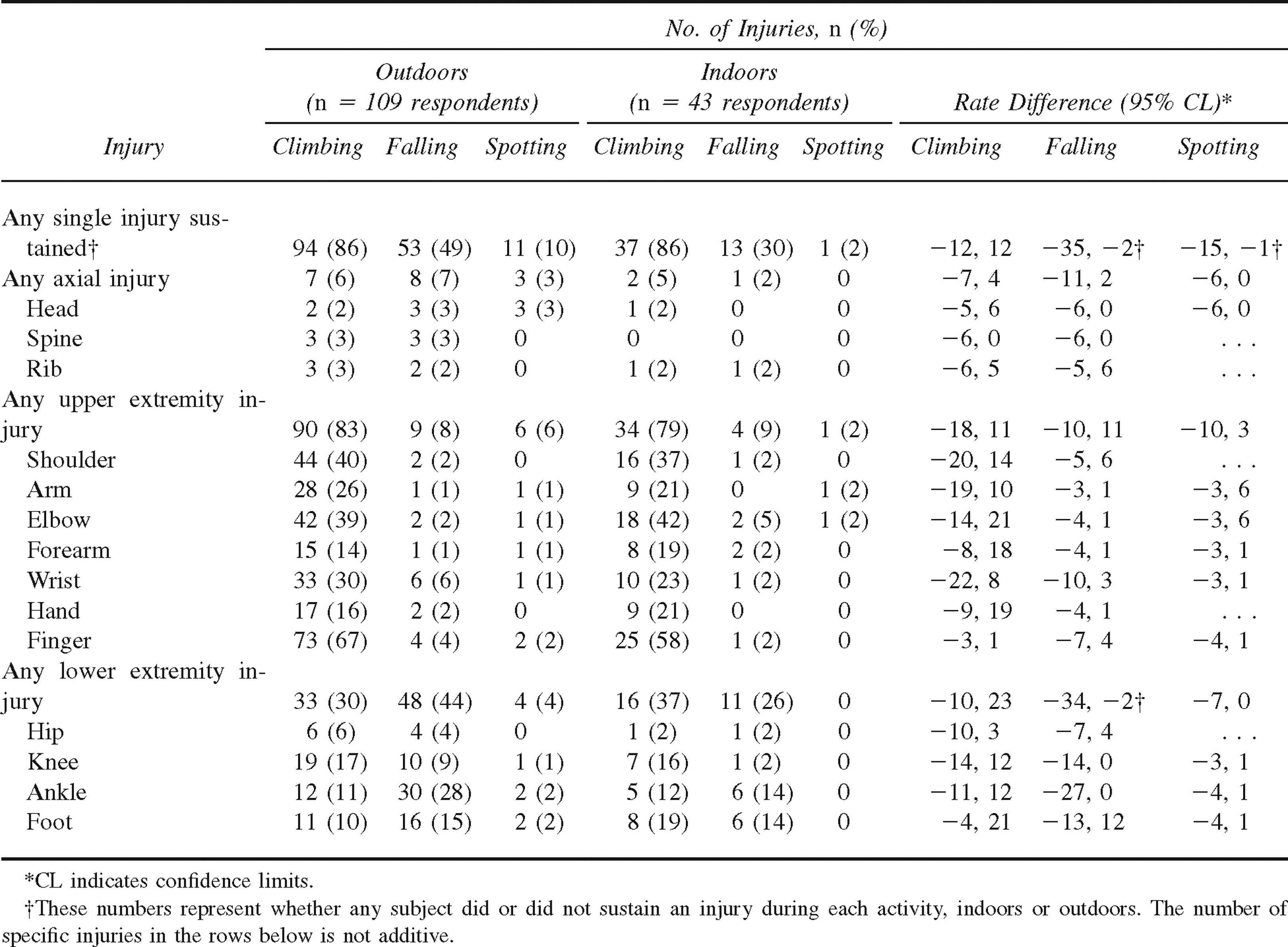
Prevalence of injuries sustained while falling differed between the cohorts, such that for all injuries, those climbing outdoors (49%) were more likely to be injured than those climbing indoors (30%; 95% CI −35 to −2). This was largely because of lower extremity injuries: 44% outside vs 26% inside (95% CI −34 to −2). The most common injuries in this category involved the knee (10 [9%] outside vs 1 [2%] inside; 95% CI −14 to 0), the ankle (30 [28%] vs 6 [14%]; 95% CI −27 to 0), and the foot (16 [15%] vs 6 [14%]; 95% CI −13 to 12). The prevalence of these injuries was unrelated to use of spotters, number of spotters, height of average boulder, height of tallest boulder climbed, use of pads, number of pads, gender, years climbing, BMI, weight, or ability level.
Spotting injuries were relatively less common. Climbers in the outdoor cohort sustained more injuries: 10% outside vs 2% inside (95% CI for difference −15 to −1). Injuries were generally limited to the upper extremity.
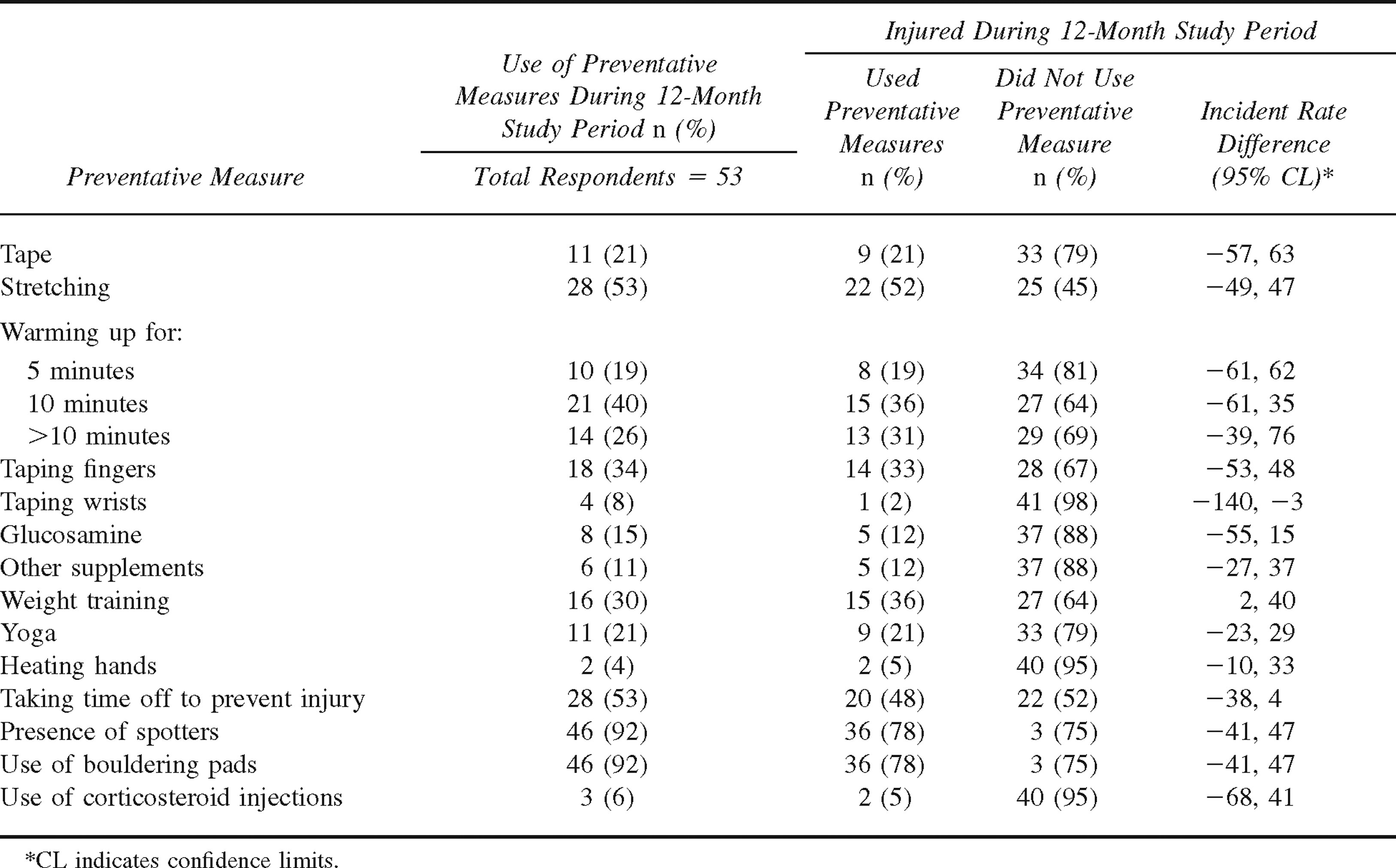
Preventative Measures
Of the preventative measures analyzed, only 2 offered a protective effect (Table 5). They were taping the wrist and weight training. The most commonly used measures included the use of bouldering pads, 46 subjects (92%); presence of spotters, 46 (92%); taking time off of bouldering to prevent injury, 28 (53%); stretching, 28 (53%); warming up for approximately 10 minutes, 21 (40%); and taping fingers, 18 (34%). Use of preventative measures was not significantly different between cohorts.
Preventative measures and relationship to injury during study
Discussion
An overwhelming majority of boulderers reported an injury while climbing. Half were injured while falling, and few were injured while spotting. Most injuries were to the upper extremity, with substantially less boulderers reporting lower extremity injuries. The finger was most frequently injured, and more frequently in the outdoor cohort during the study. Unfortunately, it appears that the majority of the preventative measures used did not reduce the number of injuries.
Our study demonstrated a high proportion of injured participants, with a similar pattern to that of rock climbing.2,4,11–16 For example, Paige et al. 4 found career injury incidence to be 49% (46/94) for traditional style climbers and 51% (48/94) for sport climbers. In that investigation, 48% (120/251) were injured on natural rock, similar to our outside group. They also reported 52% (131/251) of climbers injured on artificial rock, similar to our indoor population. 4 Wright et al. 3 found a 44% (131/295) rate of career injuries, 32% (94/295) of which involved the fingers. Schoffl et al. 17 reported injuries by location in injured climbers presenting to a sports medicine clinic. By location, these injuries involved a finger in 41% (247/604), an elbow in 13% (81/204), a shoulder in 5% (30/604), and a knee in 4% (22/604) of cases. 17 Gerdes et al. 18 reported 2,472 injuries in 1,887 injured climbers who completed a web survey similar to our own. The distribution was finger 27.5%, ankle 12.6%, elbow 9.2%, shoulder 9.2%, and knee 5.1%. 18 Most boulderers had suffered from an injury while climbing, with the majority of those injuries being to the upper extremity. Consistent with previous studies of rock climbing, finger injury was the most common site and appeared to be recurrent. 2 –4,6,14 These results suggest that boulderers and their healthcare providers should be attentive to overuse and high-force injuries to the upper extremities from the demands of this sport.
Although most boulderers experienced an injury while climbing, approximately half experienced an injury while falling. It should be emphasized that the purpose of climbing small boulders is to have the luxury of a safe fall from any height attained during an attempt, but many climbers reported a highest boulder climbed to heights of up to 15.24 meters. It is therefore possible that the line between bouldering and sport climbing is being blurred. Our results failed to find a relationship between falling injury and variables such as climbing higher boulders or the use of more pads or spotters. The low rate of injury found while spotting suggests that it is relatively safe.
Few of the injury prevention strategies employed by boulderers were associated with reductions in the number of injuries. Prevention of finger injuries is of particular concern given their high incidence and prevalence. Many authors have made the observation that certain aspects of rock climbing and bouldering make finger pulley injuries extremely likely over time, specifically the A2 finger flexor tendon sheath pulley.6,9,12,15,19–21 Although, there are many hold techniques in bouldering, 2 main positions are under investigation: the crimp grip positions (where the proximal interphalangeal [PIP] joints are flexed 90° and the distal interphalangeal [DIP] joints are hyperextended) and slope grip positions (where PIP joints are extended, figure 1). Biomechanical models have suggested 2 theories with respect to these injuries that might be useful among boulderers. First, after extensive warm-up, 100 climbing moves, or 50 cyclic crimp grip holds, there is an increased distance of bowstringing over the distal edge of the A2 pulley in the crimp position by 30%. 9 However, our data showed no relationship of warming up for greater than 10 minutes to rate of any injury. This could relate to the heterogeneous nature of an individual's warm-up. Second, another finger-specific problem, known as the Quadriga effect, concerns holds involving a single digit. 9 Specifically, when the force on a hold sharing the load is transferred from multiple digits to a single digit, the force on that digit's tendon sheath is greater than that of each finger in the multifinger hold. This could account for a larger number of pulley injuries in single-digit loading. This Quadriga effect is present in both crimp grip and slope grip positions. Maximum force of an isolated slope grip (i.e., using the hand on holds with PIP joints extended and flexion at the DIP joints) was 20% higher than isolated crimp grip, indicating a more efficient use of flexor digitorum profundus. 9 This finding suggests that a higher load could be applied to a single digit loaded in the slope position rather than the crimp position with potentially lower risk of pulley injury. Similar to previous studies, we found taping fingers to be ineffective at reducing finger injury. 22 –24
Limitations
This investigation has several limitations. First, although the initial survey yielded a fair sample size to determine the prevalence of injuries, the calculation of a 1-year incidence rate of bouldering injuries is dramatically limited by the large proportion lost to follow-up. This limitation could create a reporting bias that those injured might have been more likely to complete follow-up surveys. The majority of our very young bouldering population comprises a highly mobile group. E-mail was thought to be the best means for follow-up; however, despite this assumption, a large proportion was lost to follow-up, limiting our ability to calculate representative incidence rates for injuries. Nonetheless, the pattern and rate of injury in this study is similar to previous studies of rock climbing. Furthermore, baseline comparisons between those included and those lost to follow-up did not reveal significant systematic biases at baseline. Second, the study did not provide a strict definition for injury, nor did we investigate reductions in the severity of injuries. No detailed physical examination was performed by a medical professional. Subjects were permitted to determine whether any injuries constituted a significant injury. The individual's perception of significant injury, however, is likely to both guide healthcare seeking and motivate the use of preventative measures, so the subjective definition was chosen for this study. Third, this study did not take into account other orthopedic problems or comorbid conditions of subjects that might have confounded the results. It is possible that subjects omitted injuries they attributed to other conditions. It is possible that our results would be dramatically different within a subgroup having a specific comorbid condition. Because these subgroup analyses were not part of our a priori hypotheses, we did not explore this possibility. Fourth, the use of dichotomized “yes” or “no” style of questions could have obscured more subtle differences in injury severity. This could have resulted in an inability to detect difference in injury severity by preventative measures, where one did not exist in simple injury occurrence. Fifth, we were unable to account for exposure through time spent bouldering, time spent on various degrees of bouldering difficulty, repetitive attempts in single sessions, time between sessions, or participation in other recreational activities. During instrument development, we determined that such detailed bouldering logs would result in a dramatic reduction in response rate and a shortened instrument was preferable and thus adopted. Thus, we believe our results are applicable to the average boulderer but do not permit a calculation of injury per time unit bouldering nor a difficulty adjusted measure of bouldering activity. Sixth, we were unable to determine whether those who reported using preventive measures were actually using such measures when injured or the frequency with which they used such measures. It is possible that no one was injured while using preventative measures and that all injuries occurred when no such measures were in use. Our results indicate, however, that those using preventative measures receive no reduction in the number of injuries sustained. Seventh, the small sample size precludes us from stating that the 2 groups were equivalent—We can only assert that we failed to detect a difference. We assumed that approximately half of respondents would use preventative measures. We expected to see injury prevalence of 60% among those not using preventative measures and 20% among those using preventative measures. With a target enrollment of 56, we would have 80% power to detect this difference at the alpha = .05 level. In retrospect, however, it is clear that these assumptions were not met, and future studies will need substantially larger samples to demonstrate equivalence to detect a small difference. Finally, we surveyed active boulderers, and those who have suffered injuries sufficient to terminate a bouldering career would not be represented in our initial prevalence sample and might have been more likely to follow up our incidence sample.
Conclusion
Bouldering is a sport comprising climbing boulders, falling, and spotting. Climbing injuries are very common, with little understanding of how to reduce or prevent them. Falling injuries are frequent among those who boulder outdoors and are more likely to suffer a falling injury to the knee. Spotting injuries are rare. The majority of the injuries sustained involved the fingers and occur while climbing boulders. Preventative measures commonly employed appeared ineffective in reducing the overall number of injuries. Future studies should focus on reducing finger and upper extremity injuries while climbing, with a focus on bouldering techniques and novel prevention strategies.
Footnotes
Acknowledgments
The authors extend thanks to all the subjects involved in this investigation.
1
The authors have no conflicts of interest.