
Abstract
A tool that can differentiate ischemic stroke from other neurological conditions (eg, hemorrhagic stroke, high-altitude cerebral edema) in the field could enable more rapid thrombolysis when appropriate. The resources (eg, an MRI or CT scanner) to investigate stroke at high altitude may be limited, and hence a portable tool would be of benefit. Such a tool may also be of benefit in emergency departments when CT scanning is not available. We report a case of a 49-year-old man who, while climbing at 5900 m, suffered a left middle cerebral infarct. The clinical diagnosis was supported using 2D Power Doppler. The patient received aspirin and continuous transcranial Doppler was used for its potential therapeutic effects for 12 hours. The patient was then evacuated to a hospital in Kathmandu over the next 48 hours. This case report suggests that portable ultrasound could be used in the prehospital arena to enable early diagnosis of thrombotic stroke.
While ascending to 5900 m on Cho Oyu in Tibet, a 49-year-old Canadian climber collapsed to the ground and was subsequently unable get up or walk. He was a fit climber (with no significant past medical history or medication requirements) who had previous altitude experience to 6959 m. On the day prior, however, he had a mild gastrointestinal disturbance. His team radioed for assistance believing he might have developed high-altitude cerebral edema (HACE). A retrieval team of 2 doctors and 6 Sherpas were sent to assist. The team was informed that he had collapsed while resting. Examination revealed a patent airway with possible decrease of protective mechanisms (he had no gag reflex). He was localizing to pain and his eyes opened to voice, but he had profound dysphasia. He also had a dense right hemiplegia and right-sided neglect. He was given oxygen, dexamethasone 4 mg intravenously, and then evacuated by stretcher on foot over rough glacial terrain from 5900 to 5600 m (Advanced Base Camp).
On arrival at 5600 m approximately 3 hours later, the patient was given aspirin (300 mg orally), intravenous fluids, and a urinary catheter was inserted. He was subsequently made nil by mouth. A nasopharyngeal airway was used to help maintain his airway and basic measures undertaken to maintain adequate tissue oxygenation (supplementary oxygen at 2l/min). Keeping the patient on a self-inflating mattress protected pressure areas, and he was kept warm using sleeping bags and a generator-powered heater. Hourly neurological observations, blood pressure, SpO2, and urine output were measured.
The team was part of a medical research expedition and had access to additional research equipment. A portable, handheld ultrasound machine (Sonosite MicroMaxx™ 2MHz Transducer, Bothell, WA) with transcranial Doppler (TCD) capabilities was used to assess his cerebral perfusion. While good flow was found in his right middle cerebral artery (MCA) (normal flow demonstrated in Figure 1), no flow was demonstrable in his left. Near-infrared spectroscopy measurements of cerebral oxygenation (Somanetics, Invos C, Troy, MI) demonstrated a regional saturation (rSO2) of approximately 55% on the left, while higher saturations in the region of 70% were recorded on the right (Figure 2 demonstrates the difference in right and left rSO2 values in the patient overnight).
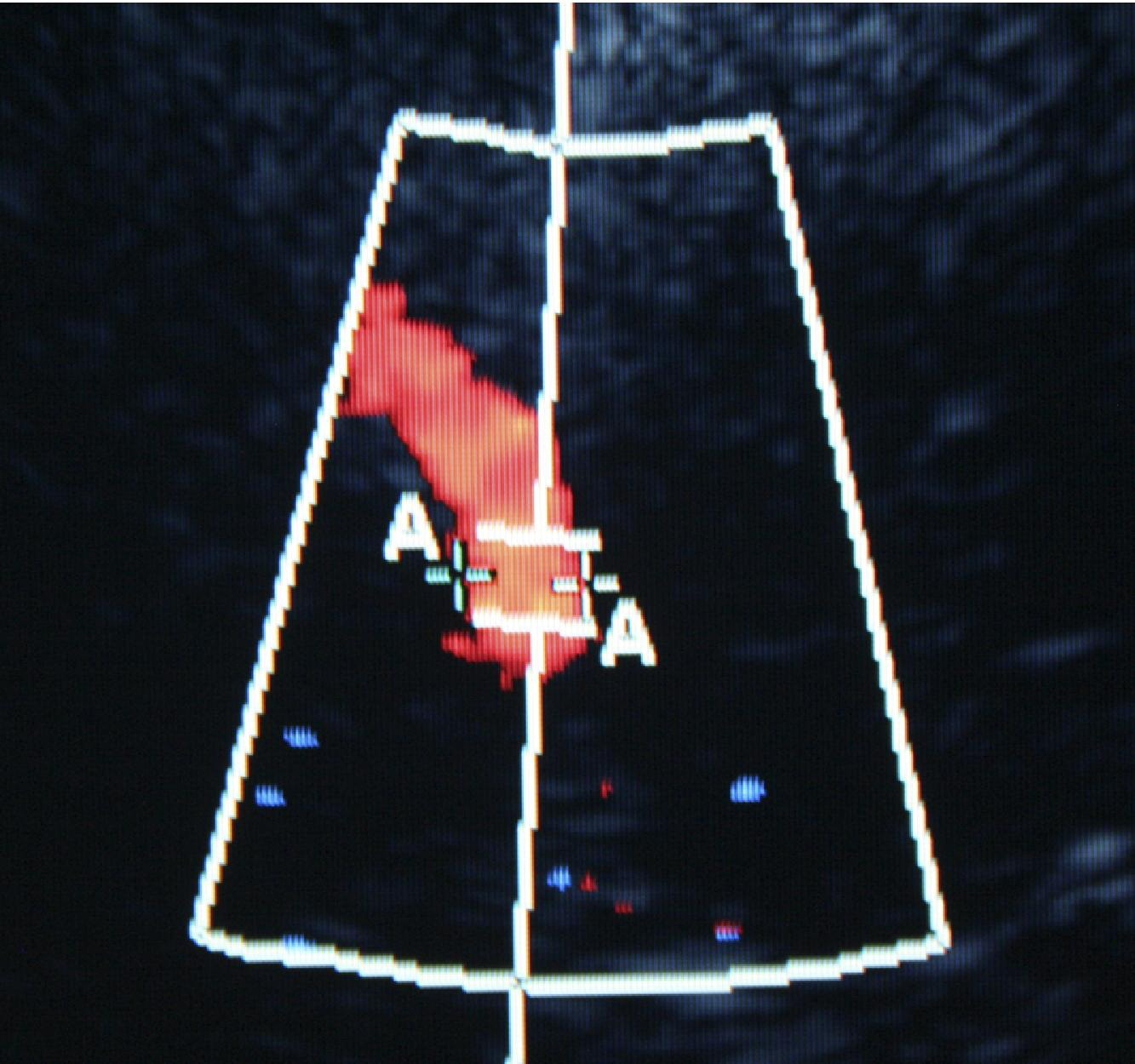
Normal Right Middle Cerebral Artery visualized through a temporal window at 5300 m using 2D ultrasound (Micromaxx™, Sonosite, Bothwell, WA).
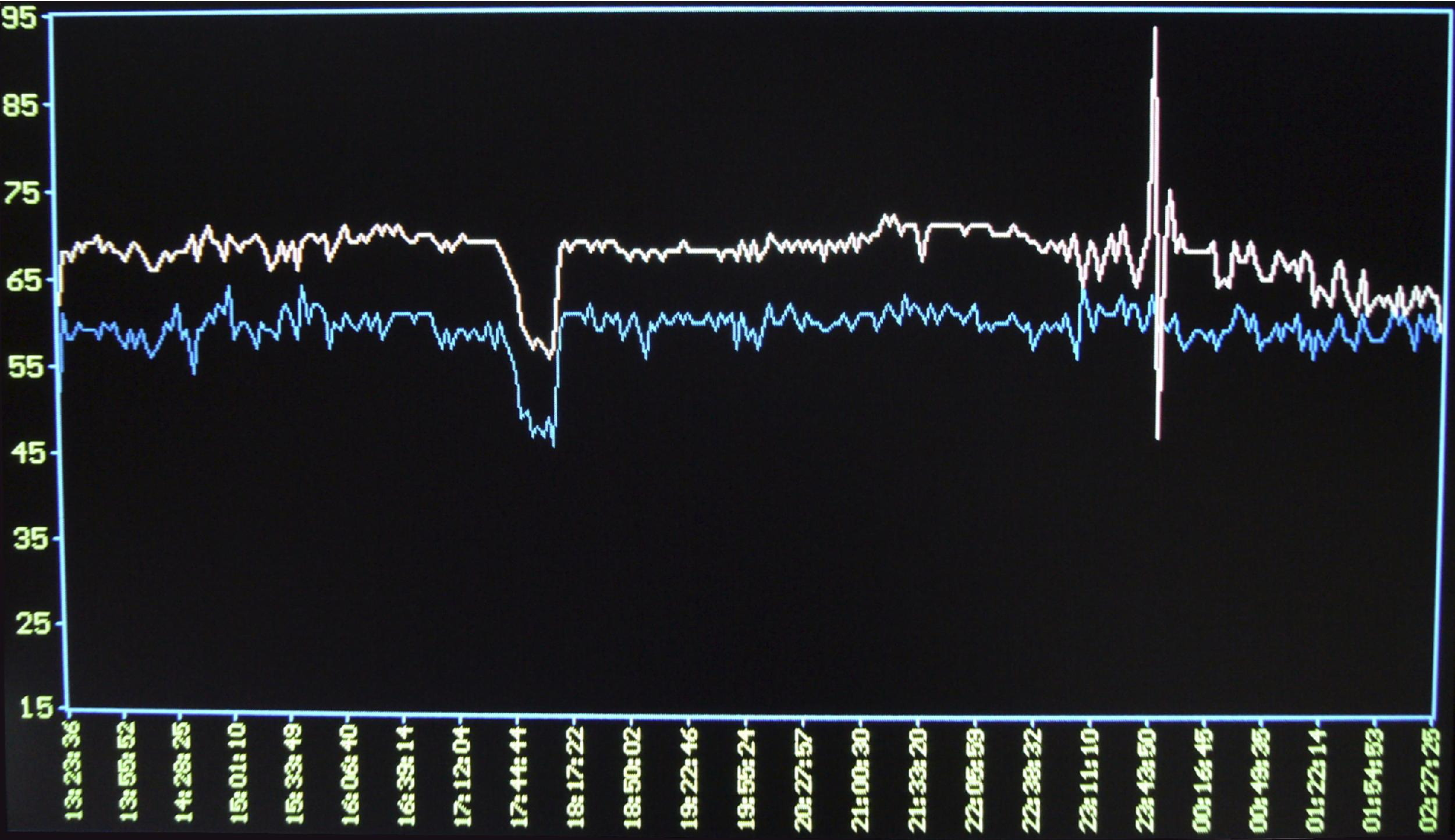
Near-infrared spectroscopy monitoring of cerebral saturations (rSO2) showing reduced left (blue) regional cerebral oxygenation compared to right (white).
The team did not have the capabilities to undertake intravenous tissue plasminogen activator (tPA) thrombolysis. Overnight, prior to evacuation the following morning, the TCD signal was maintained constantly as it has been suggested that ultrasound can improve thrombolysis.
After 12 hours, the patient's dysphasia had improved to the point where speech could be understood, and some power had returned to his right leg. Stretcher evacuation continued by foot to the road head at 4900 m. One night was spent at 2300 m before the patient was evacuated by helicopter to 1300 m. He was subsequently flown back to North America. Figure 3 is a single slice of the CT performed subsequently in North America, confirming an ischemic area within the left MCA lenticulostriate branches (deep perforator) territory. He has subsequently made a good recovery, regaining his speech, and he now walks with a cane. We are unable to assess whether or not continuous 2-MHz ultrasound was a significant factor in improving his symptoms.
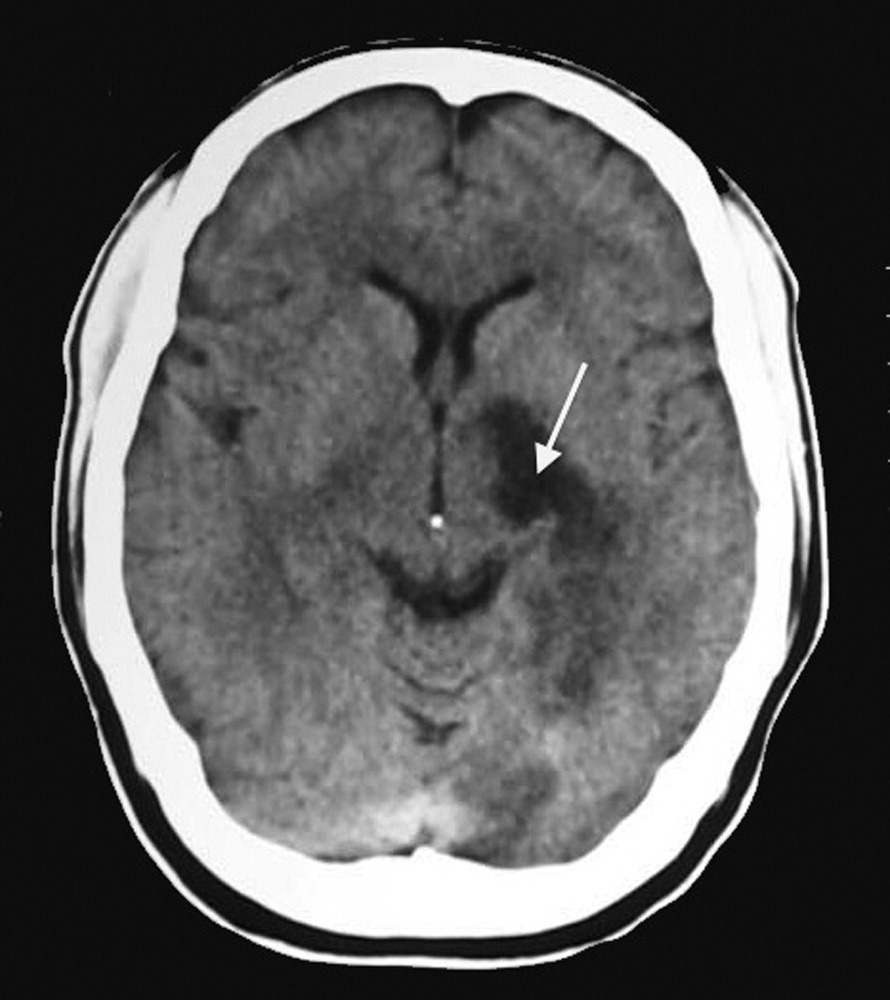
Subsequent CT scan demonstrating residual infarct in left MCA deep perforator territory.
Discussion
We believe this is the first case report demonstrating the value of Doppler ultrasound in the diagnosis of ischaemic stroke in remote environments.
The use of ultrasound to assess ischemic stroke in the clinical setting and to guide thrombolysis has previously been described. 1 -4 Its principal advantage, even when CT is available, is that, in experienced hands, ultrasound can demonstrate occluded vessels a number of hours prior to the development of ischemic parenchymal change on CT. Many conditions (eg, cerebritis, tumors, migraine) that can present with similar lateralizing signs to an ischemic stroke, do not demonstrate an obvious abnormality of CT. The additional weight of evidence pointing to a vascular cause when the MCA is not clearly visible helps to support the use of thrombolysis if not contraindicated.
A small study demonstrated that, with ultrasound, it was feasible to assess intracranial vessels rapidly in 20 of 25 patients in the prehospital arena and hence gain an earlier diagnosis enabling more rapid treatment. 5 Conversely, ultrasound does not demonstrate hemorrhagic stroke, which can be rapidly ruled out by CT, and this is why CT is the standard imaging tool in hospital. Any clinical suspicion that a patient may have a hemorrhagic stroke in the prehospital arena or prior to CT should be a contraindication to thrombolysis.
Allendoerfer et al 6 performed a multicenter prospective study correlating degree of ultrasound measured MCA occlusion and functional outcome with main stem occlusions having a particularly worse outcome. There is some evidence that continual TCD can augment lysis of thrombotic strokes in combination with tPA thrombolysis. 7 -9 There is limited evidence that ultrasound alone can improve thrombus lysis. 10 The CLOTBUST (Combined Lysis of Thrombus in Brain Ischemia using Transcranial Ultrasound and Systemic TPA) study demonstrated complete recanalization of the MCA within 2 hours after TPA bolus in 25% of patients treated with combined TCD (2 MHz) and tPA (n = 63) compared with 8% of those who received tPA alone (n = 63, p = 0.02).9,11 The mechanism of this effect is thought to be direct ultrasonic breaking of molecular linkages of fibrin polymers, which increase the surface area for the drug to work. 12 Others have had similar results and a recent meta-analysis has been published. 13 One small noncontrolled study (n = 6) demonstrated partial recanalization in 5 patients using 2-MHz TCD alone with complete recanalization in 1 after 24 hours. 10 Hence, for our patient, in the absence of the ability to provide tPA thrombolysis, continuous TCD was administered.
The principal limitations of ultrasound diagnosis and enhanced treatment of ischemic stroke are the technical skills required to perform it, and that in approximately one-fifth of patients, the temporal window is not adequate to enable good visualization of the middle cerebral artery. Its inability to demonstrate hemorrhagic stroke should also always be considered.
Summary
This case reports the first field use of Power Doppler to aid diagnosis (and possibly aid treatment) of ischemic stroke. It has demonstrated that this technique is practical in the remote environment. Further studies in emergency departments and in organized pre-hospital care groups are required to confirm the usefulness of this technique.
Footnotes
Acknowledgements and Funding
We are grateful to Sonosite for the loan of equipment and to Somanetics (now Covidien) for the loan if the Invos cerebral oximeter. Full details regarding the Caudwell Xtreme Everest expedition can be found on