
Abstract
This case report describes the presentation and management of a patient with an isolated right sixth nerve palsy while trekking in Nepal. Consideration is made of the anatomy of the sixth nerve and the differential diagnoses afforded to this isolated sign, including high altitude cerebral edema. The case stresses the need to exclude life-threatening pathologies for any symptoms associated with altitude and includes decision-making processes on whether to monitor the patient in the field or evacuate them to a definitive care facility.
Case Report
A 37-year-old white male with no previous altitude experience participated in a trek to Everest Base Camp (5350 m). Pre-expedition screening elicited that the young man had a history of sporadic, infrequent migraines that resolved with simple analgesia and were not associated with visual changes. He declared no other significant past medical history, drug history, or allergies.
After flying into Lukla (2600 m) from Kathmandu (1400 m), the young man trekked for 2 days to reach Namche Bazaar (3400 m). There he developed a high altitude headache (HAH) that resolved with a day of rest and simple analgesia. On continuing to an elevation of 3800 m, he once again began to develop HAH, with associated nausea and loss of appetite, symptoms suggestive of a progression to acute mountain sickness. On the fifth day, the young man continued to trek to higher elevation and reached Pheriche (4400 m) without any further issues.
While sleeping at 4400 m, the young man developed significant occipital headaches, periodically waking him through the night, and at sunrise he noticed that he had developed diplopia. At this point, advice was sought by the lead guide, via telemedicine, from the remotely located trek doctor. Subsequently, the young man’s headache resolved with rest, adequate fluid hydration, electrolyte supplementation, a treatment dose of acetazolamide 250 mg, and simple analgesia, but his visual impairment remained.
On sleeping a second night at 4400 m, the young man’s occipital headaches returned, resolving by morning, but his visual impairment deteriorated. He remained lucid throughout with no ataxic gait. Physical examination, performed by a member of the Himalayan Rescue Association team based at Pheriche, demonstrated nonfatiguing nystagmus on leftward gaze and debilitating diplopia on rightward gaze. The young man’s oxygen saturation, taken with a peripheral pulse oximeter, were 80% on air (expected normal 82–90%), 1 pulse 82 beats/min, respiratory rate 18 breaths/min, blood pressure 118/84 mm Hg, and temperature 36.8°C.
The young man was suspected to have HACE, was treated with a single dose of oral dexamethasone, and was evacuated by helicopter for urgent magnetic resonance imaging (MRI) in Kathmandu. On the same day, the MRI head report described “atypical high altitude cerebral edema–related white matter changes.” The patient was then examined by an ophthalmologist, who diagnosed an isolated right sixth nerve palsy with no other abnormalities on fundoscopy.
An ophthalmology review 2 months later determined that the patient’s symptoms had almost completely resolved.
Discussion
The sixth, abducens, cranial nerve follows a protracted course from its source in the brain stem, 2 subsequently making it vulnerable to pathologic processes at various locations. Originating in the pons, it emerges into the subarachnoid space, traveling superiorly along the clivus of the occipital bone before piercing the dura mater as it arches steeply over the petrous temporal bone. It then enters Dorello's canal and passes through the cavernous sinus, over the internal carotid artery, before exiting the cranial vault through the superior orbital fissure to innervate the ipsilateral lateral rectus muscle. 3 Its vascular supply derives from distal branches of the internal carotid artery. 4
Cases of sixth nerve palsy, albeit rarely, have been documented at altitude both in isolation and concurrently with other cranial nerve palsies.5-7 The suggested pathophysiologic mechanism in these cases has been of an increase in intracranial pressure secondary to HACE, with descent leading to resolution.8-10 The abducens nerve is particularly susceptible to compression and stretching at the point where it traverses the petrous temporal bone. 2
Pathologic processes associated with the abducens nerve, their potential anatomic location, and details relevant to the case report.
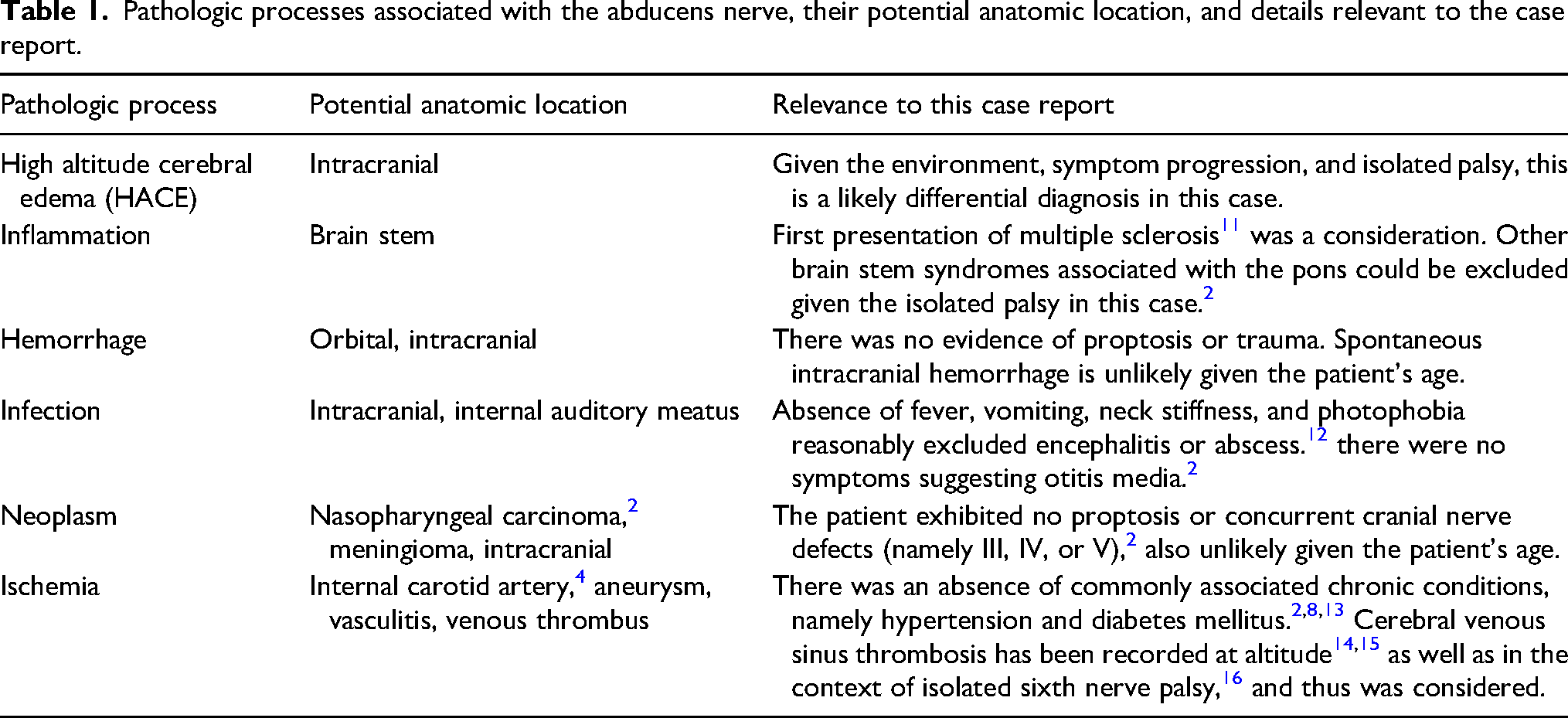
In this case, when symptoms of headache began at 3400 m, it was reasonable to assume that altitude, the patient’s migraine history, or any of the stresses of foreign travel and trekking, including, but not limited to, nutrition, dust, and dehydration 17 could be the cause. Simple management of the most common differential diagnoses, with HAH at the forefront, therefore was appropriate initially.
However, with ongoing ascent, the persistence of the symptoms, recognition of an isolated intractable neurologic finding, the absence of a relevant past medical history, and the age of the patient led to HACE and cerebral venous sinus thrombosis representing the most severe acute differential diagnoses that required management (Table 1).
If moderate acute mountain sickness18,19 had been recognized earlier and managed appropriately, with a pause in ascent, rest, and a review of the patient’s condition at 24 h, the patient may have avoided developing HACE altogether. This underlines the challenges of telemedicine in the wilderness setting, where the inability to physically assess the patient presents as the primary disadvantage, with limited access to quality communication between guide and medical support compounding this issue. Timely and decisive decision making therefore is essential in supporting patients as well as those caring for them in these environments.
In this case, physical assessment by a medical practitioner was required—hence the involvement of the Himalayan Rescue Association in Pheriche, whose personnel treated for HACE but naturally could not rule out an ischemic event. Thus, descent to facilitate specialist assessment and appropriate imaging presented as the most appropriate next step in management, descent being the most important consideration for patients with persistent neurologic conditions at altitude. 8
Given the patient's relatively low oxygen saturation of 80% on air at an altitude of 4400 m, 1 and with hypoxia being a recognized cause of diplopia, 20 the patient reasonably could have been started on low flow oxygen. However, it is well documented that the accuracy of pulse oximetry at altitude is inconsistent and should not complicate clinical decision-making processes. 1
With awareness of the likely transient nature of sixth nerve palsy at altitude in someone so young, 21 and given that the patient was not ataxic, evacuation could also have been reasonably achieved on foot rather than by helicopter.
Conclusion
While HACE was suspected clinically but only definitively diagnosed on MRI, there are several other causes of sixth nerve palsy that could have been responsible for the presentation described. Thus, when a neurologic sign is present in the austere environment, it is essential that steps are taken to evacuate the patient in a timely manner to enable further assessment. Subsequent follow-up is optimal in all cases to determine a definitive diagnosis and outcome. It should be noted that the available resources for evacuation and standard of local care will vary by region and may in some cases be entirely unavailable. This emphasizes the risks associated with travel to remote locations and highlights the need for adequate preparation and planning prior to any expedition.
Footnotes
Author Contribution(s)
Consent
Written informed consent was obtained directly from the patient at the center of the case for the purpose of the publishing of this case report.