
Abstract
High altitude cerebral edema (HACE) is a rare but potentially fatal condition previously understudied in pediatric populations. We present a case of HACE in a previously healthy 10-y-old boy who rapidly developed neurologic symptoms at 4000 m on Mount Kilimanjaro. The child experienced headache, nausea, impaired consciousness, and ataxia before requiring assisted evacuation. Immediate descent of 2295 m resulted in complete recovery within 24 h with no long-term sequelae. A literature review of HACE in children revealed only 1 prior case series of 2 patients aged 12 and 16 y. This case report and literature review illustrate the challenges of recognizing and managing pediatric HACE in field conditions without medical support. Treatment guidelines for HACE in children suggest descent, supplemental oxygen, and dexamethasone, although these recommendations are extrapolated from adult data. Early recognition and descent remain the cornerstones of pediatric HACE management.
Introduction
Altitude illness is typically divided into 3 main groups: acute mountain sickness (AMS), high altitude cerebral edema (HACE), and high altitude pulmonary edema (HAPE). AMS is a self-limiting but sometimes debilitating illness characterized by headache, gastrointestinal symptoms, fatigue, and vertigo. HACE is a life-threatening progression of AMS with symptoms of encephalopathy, including ataxia and altered mental status. HACE typically presents when one rapidly ascends above 3000 m, but it has been reported to occur at elevations as low as 2100 m. 1 HAPE is a separate manifestation with pulmonary edema and respiratory distress that can exist alone or in combination with HACE.
Mount Kilimanjaro (5895 m) is the highest mountain in Africa and a popular first peak for aspiring mountaineers. Not limited by technical difficulty, trekkers may be tempted to ascend rapidly, which results in insufficient acclimatization. The nontechnical nature of the climb also may contribute to the peak's popularity, with 20,000 climbers attempting the summit each year. 2
HACE has been described extensively in unacclimatized adults,1,3,4 whereas the pediatric presentation of this condition has received limited scientific attention, with very few cases ever published.5,6 We present a case of HACE in a 10-y-old male on an expedition to Mount Kilimanjaro. We also provide a literature review of HACE in children that highlights the clinical presentation, potential pitfalls, and knowledge gaps.
Case Report
Patient Information
The patient was a previously healthy 10-y-old male (152 cm, 44 kg) with no history of chronic illness or regular medications. There was no family history of altitude-related illness or neurologic conditions. The patient had no psychiatric history or developmental concerns. Prior to the expedition, he underwent a medical evaluation including spirometry at the parents’ initiative; the results were normal. The evaluating physician discussed altitude risks with the family but did not recommend against the climb. The patient spent 2 wk at 1000 to 1400 m immediately prior to the expedition and did not take any medications except antimalarial prophylaxis.
The expedition consisted of the child, parent, and guides. No medical personnel accompanied the climb. The expedition party carried a pulse oximeter but no emergency altitude medications. The guides had basic first aid training and access to supplemental oxygen.
Clinical Findings
During initial ascent, the child appeared well, with oxygen saturation by pulse oximetry (SpO2) ∼90% noted on Days 1 and 2. On Day 3, while crossing the Lava Tower (∼4600 m), the patient developed a headache, nausea, lethargy, and fatigue (Figure 1). These symptoms resolved after passing the Lava Tower, and the patient recovered fully by the same evening at Barranco Camp (∼3976 m). He rated his overall well-being as 9 out of 10 despite an SpO2 of 77%. Overnight, the patient slept well and replenished fluids orally without any complaints of nausea. The expedition party departed Barranco Camp for Karanga Camp (∼3995 m) on the morning of Day 4, at which point the patient appeared well with no complaints.
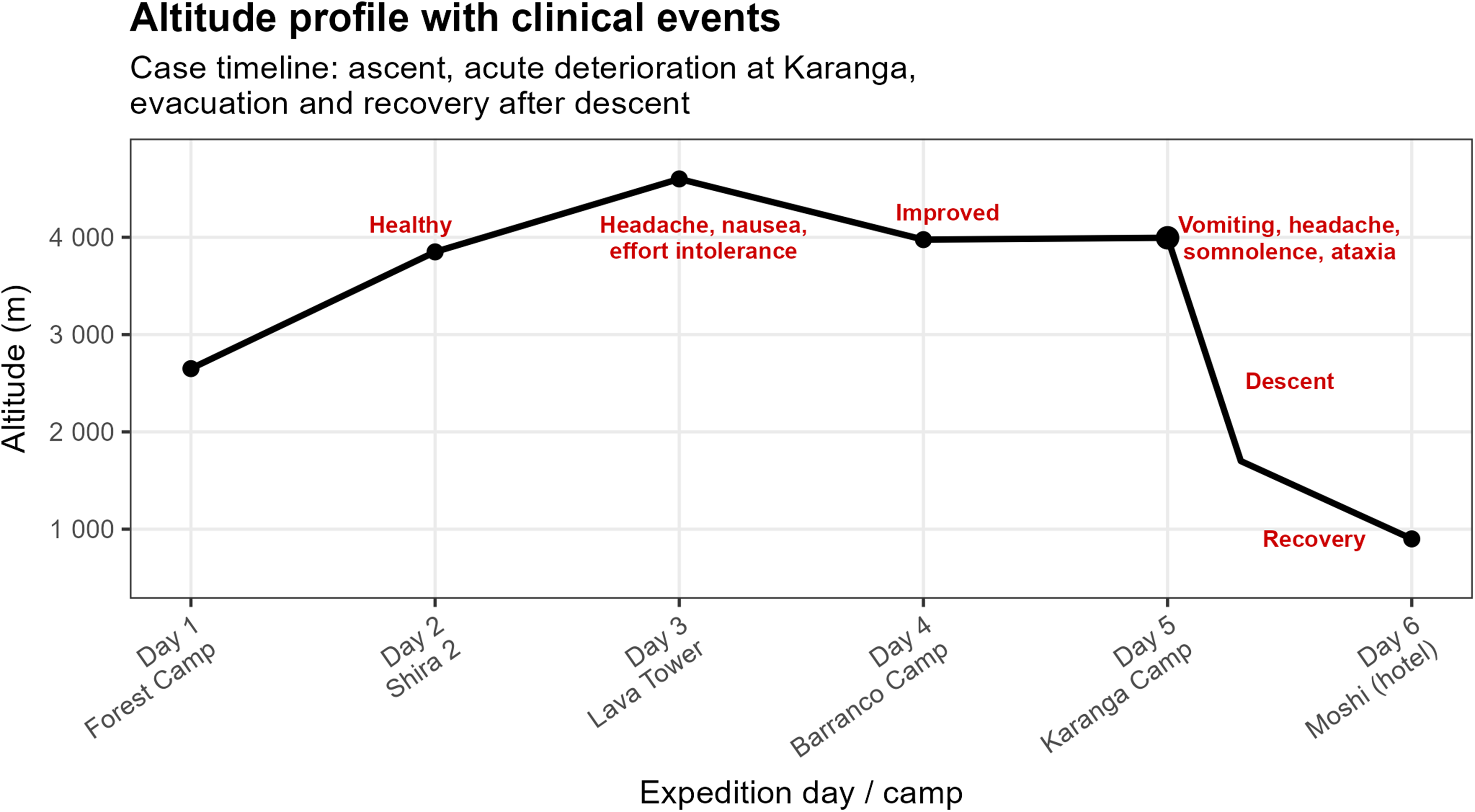
Altitude profile and clinical course during a Mount Kilimanjaro expedition. The patient remained well until Day 3, when transient headache and nausea occurred at 4600 m. On Day 5 at Karanga Camp (∼4000 m), sudden onset of vomiting, headache, somnolence, and ataxia prompted emergency evacuation. Symptoms improved rapidly during descent, with full recovery at low altitude the following day.
In the early morning of Day 5 at Karanga Camp, the patient reported nausea and headache 5 to 10 min following a bowel movement with diarrhea. Within minutes, he vomited and exhibited progressive fatigue and somnolence. After deterioration, an SpO₂ of 78% and a pulse rate of 140 to 150 beats/min were noted. The patient required assistance to dress, lost the ability to stand, and began responding minimally to verbal stimuli. The patient reports only limited, fragmented memories from this period.
Diagnostic Assessment
The working diagnosis of HACE was made by the corresponding author, who was consulted retrospectively. Diagnosis was based on the clinical presentation: acute onset of headache, nausea, ataxia (inability to stand), progressive decline in consciousness at 4000 m, and rapid improvement with descent. The parent's field assessment during the emergency was “severe altitude sickness requiring immediate descent.” No imaging or formal neurologic assessment was performed on site, and no remote medical consultation was available. Alternative diagnoses considered retrospectively included severe dehydration, gastroenteritis, hypoglycemia, stroke, and exhaustion. Diagnostic certainty is limited by the field conditions and lack of medical evaluation at the time. However, the constellation of symptoms, altitude, profound alteration in consciousness, ataxia, and rapid resolution with descent make HACE the most likely diagnosis.
Therapeutic Interventions
On recognizing the severity of the situation, the parent and guides immediately initiated rapid descent from Karanga Camp. Oxygen was available but not administered because the expedition guides advised against it. The parent, lacking medical training and deferring to the guides’ experience, accepted this recommendation. Once HACE was suspected, immediate descent was initiated. The evacuation did not follow the ascent route and instead used an alternative trail that included a brief initial uphill section before sustained descent. The child was carried down to an altitude of 1700 m, which took ∼5 h. The parent attempted to give additional fluids by mouth, but the patient was initially unable to drink on his own. His condition improved gradually during the descent with increased consciousness and ability to drink. No medications were administered.
Follow-Up and Outcome
The patient made a full recovery within 24 h of descent. On return home, the patient received medical care for slight exertional dyspnea that had not been present before the expedition. A general practitioner performed a medical evaluation including an electrocardiogram and spirometry, which were normal. The exertional dyspnea resolved completely within a few days, and no further investigations were performed. No neurocognitive concerns were noted by the parents or teachers in the subsequent months.
Literature Review
We reviewed the literature by searching PubMed using the MeSH terms “altitude sickness” (MeSH), “brain edema” (MeSH), and “child” (MeSH). Because no MeSH term exists for HACE, we performed an all-fields search for “high altitude cerebral edema AND child.” We also searched the Cochrane Library using the MeSH term “altitude sickness” and the Web of Science using the terms “high altitude cerebral edema child.” We included only English-language articles. We reviewed all abstracts to identify studies relevant to HACE in pediatric patients and examined the reference lists of the included publications.
The literature review identified only 1 case series of pediatric HACE in a 12-y-old male and a 16-y-old female. 5 The 12-y-old had a headache, vomiting, visual disturbance, and ataxia at 4500 m, and the 16-y-old displayed similar symptoms and hypoxia (SpO2 of 69%) at 3800 m. Both recovered with acetazolamide, oxygen, and descent. Three review articles containing pediatric treatment guidelines were identified, including consensus statements from the International Climbing and Mountaineering Federation (UIAA) and the International Society for Mountain Medicine (ISMM).6–8 The ISMM consensus statement mentioned unpublished observations of HACE in a 4-y-old and a 14-y-old at 3400 m. 6 Both the UIAA and ISMM recommended the same treatment for HACE in children: descent, oxygen, dexamethasone, and (if available) a portable hyperbaric chamber to facilitate descent. With regard to dexamethasone, the UIAA statement referenced the ISMM statement, which, in turn, referenced an editorial published 1998. 9 Both consensus statements specifically noted that these recommendations were based on adult treatment guidelines because there are no data on the use of drugs for HACE in children.
Discussion
The published cases of pediatric HACE suggest that HACE may develop in children at altitudes of 3800 to 4500 m, which are within reach of travelers to the Alps and Rocky Mountains. 5 Besides absolute altitude, the rate of ascent is also an important risk factor for altitude illness. In this case, the rate of ascent was rapid, with a night at >4000 m on the third day. The ease of climbing high and fast is a risk that makes Mount Kilimanjaro particularly dangerous.
In this case, symptoms began immediately after a bowel movement, raising the question of whether a Valsalva maneuver precipitated a surge in intracranial pressure (ICP) or bowel urgency reflected ICP that was already elevated. ICP at altitude can spike dramatically with minimal exertion. 10 The “tight fit” hypothesis further suggests that children may have less compensatory intracranial reserve, making them more vulnerable to small increases in cerebral edema.
In addition to physiologic differences, children may not perceive and communicate symptoms the same as adults. This is especially relevant in altitude illness because diagnostic tools such as the Lake Louise score (LLS) are based on self-assessment.11,12 A version of the LLS with age-appropriate language and visual aids for 4- to 11-y-olds has been suggested to mitigate these differences. 13 A survey-based study found that children reported 3 or more altitude-related symptoms (eg, headache, loss of appetite, vomiting, fatigue, insomnia, shortness of breath, or dizziness) almost as often when traveling at sea level as at altitude (21 vs 28% of children in the study). 14 This suggests that the disruption in daily routine associated with travel may elicit symptoms resembling altitude illness in children.
Neither the patient in this case nor those in previously published cases received corticosteroids, even though this is the only pharmacologic treatment recommended in available guidelines. Additionally, oxygen was not given in this case even though the SpO2 was low. Despite inconsistently applied adjunctive treatments, all patients in published cases recovered well with prompt descent.
The scarcity of reported HACE cases in children is likely influenced by the fact that relatively few children participate in high altitude expeditions combined with the overall rarity of HACE itself. As a result, our understanding of HACE in pediatric populations remains extremely limited. Early recognition and prompt descent remain the cornerstones of managing suspected HACE in children until more data become available.
Footnotes
Ethical Considerations
The case report is based exclusively on events that occurred without any involvement of the authors. According to the Swedish Ethical Review Authority, ethical approval is not required for this type of case report. We recognize that the unusual nature of this case makes true anonymity difficult but have made every effort to minimize identifiable information.
Author Contribution(s)
Consent for Publication
Written informed consent for publication was obtained from the patient and legal guardian.