Abstract

INTRODUCTION
Spectra Laboratories is a specialty laboratory with the majority of specimens originating from dialysis centers. In a previous article, “Automating a Dialysis Laboratory” (JALA, Nov. 1998), the unique nature of this patient population and the challenges of automating a dialysis laboratory were discussed. In that article, fibrin clotting was identified as one of the most significant challenges to automating front end automation. Because of the difficulty associated with automation of specimen handling when serum samples are frequently received clotted, we focused our efforts on management of result data and auto-edit of non-serum based testing. At the same time, we also reconsidered serum based sample handling which is a large proportion of our testing. What follows is our approach to the fibrin problem and automation, how these problems were addressed, and how “know thine enemy” resulted in potential solutions to the problem.
FIBRIN
As previously discussed, one of the most significant challenges to productivity in testing the blood of dialysis patients is the formation of fibrin in the serum. Dialysis patients are prone to a development of variety of coagulation defects 1,2 . The in vitro formation of fibrin clots in serum samples is due in part to the heparinization of dialysis patients which is part of their treatment, given to avoid dangerous clotting during the procedure 3 . Despite our clients' best efforts to allow time for the tubes to clot, and spinning them down adequately, 40% still contain visible clots in their serum upon arrival at the lab. The mechanism that allows heparin to keep the blood from clotting involves inhibition of calcium in the coagulation pathway. Over time, calcium is released and the heparin is no longer able to inhibit clotting. Consequently, although the serum may be clear at the time it is spun and separated from the red blood cells, by the time the sample arrives at the lab, clotting in the serum may reoccur.
These fibrin clots can accumulate on probes and tubing and make it difficult to automate processes that involve serum samples, such as pouring aliquots for testing. We rim and squeeze the serum out of the clot, re-spin the blood, and filter the serum, all in order to eliminate small clots and fibrin strands that are difficult to see. Even after these time consuming procedures, approximately 25% of the samples re-clot. Therefore, just before samples go on an instrument, the samples must be manually rechecked for clots.
TESTS PER ACCESSION - ANOTHER UNIQUE FEATURE OF THE DIALYSIS LAB
As was discussed in my previous article, Spectra receives more tests per accession than the typical reference laboratory. A typical reference lab receives an average of 1–3 tests per accession, while the dialysis laboratory receives an average of 8–12 tests per accession. This is due to the large number of patients who require monitoring of multiple disease states that commonly accompany renal disease, including anemia, diabetes, bone and heart disease and other co-morbid conditions. Increased tests per accession means an increased number of aliquots to be processed and analyzed on various instruments. This places added emphasis on the need to manage aliquoting and to limit the number of aliquots wherever possible.
THE GOAL OF THE PROJECT
We began with the goal of developing a specimen handling workflow that would, 1) eliminate mispours; 2) eliminate contamination; and 3) increase efficiency. As discussed in our previous article, the TLA companies were unable to meet our needs in accomplishing these goals, especially with the front-end aspect of processing, due to the pervasiveness of in vitro fibrin clotting in this patient population. Since we were unable to take advantage of TLA, we selected a different approach. We made the assumption that, in the long run, the fibrin issue would eventually be solved, either with tube additives that did not interfere with testing, or a mechanical approach to resolving clots. We began our search for an affordable solution that would utilize currently available technology.
THE TECAN
Nearly every laboratory has a Tecan aliquotor 4 . We have a number of them in our own lab. The basic operation of a Tecan is to pipette from a source tube to an aliquot tube or microtiter plate. We saw the potential for a more advanced utilization of the Tecan if it could be modified to function like our bidirectionally interfaced instrumentation. We wanted the Tecan to be
1) bi-directionally interfaced with the LIS to obtain orders and determine what aliquot tubes need to be pipetted, and, 2) have the ability to pipette from our source tubes to destination tubes with the filters that we use to eliminate fibrin and fibrin products. We met with Tecan representatives in mid 1997 to determine whether this application was possible. At the time, Tecan considered their instruments as batch aliquotors rather than front end primary aliquotors. As we explained our needs the company recognized how the concept could be realized. Development of this revised functionality took place as a joint effort of Tecan and Spectra over the course of the next year.
IDENTIFYING THE BARRIERS
Our main challenges were: 1) fibrin clots, 2) potential contamination from carryover or splashing, and 3) the height of the filters and their narrow lumen. At Spectra, Porex “Push-down” filters are used after the clot has been resolved, to eliminate any remaining small fibrin clots or strands [Fig.1] 5. These filters have allowed us to correct many of the fibrin problems in our manual system. The access height of the sample tubes with the filters inserted is two to three inches higher than typical test tubes. Additionally, the presence of the filters narrows the lumen of the tubes. These factors are the main impediments of front end specimen handling with TLA systems when dealing with dialysis patient samples. Although reclotting remained a problem, we felt that Tecan's clot detection system, if efficient, could identify any fibrin clots present, and the fibrin issue would be partially resolved.
Another of the goals in implementation of the Tecan was to assure that simple serum to serum contamination would not occur. The dialysis population includes 1 to 2% chronic hepatitis B antigen positive patients, over ten times that of the normal population 6. The antigen viral load in these chronically positive patients is usually in the order of one million circulating virons per milliliter of blood 7. The slightest contamination from these chronically positive patients could result in false positive results in otherwise antigen negative patients. When dialysis patients become hepatitis B positive, they must be physically isolated and their equipment restricted only for their use 8. This creates a tremendous psychological burden for the patient, and is very expensive for the dialysis unit.
Because of the excessive cost of disposable pipette tips, we initially experimented with the number of washes and a number of different wash solutions, including a saline-detergent mix. Unfortunately, if the Tecan was used to aliquot Chemistry and Immunochemistry, the saline caused chloride contamination in the chemistry aliquot. We were forced to change to disposable pipettes in order to eliminate any possibility of contamination.
DEALING WITH FILTERS
Next, we worked with Tecan to address issues with the filter. At the time, Tecan was using a single test tube holder that held any size tube with a spring mechanism from one side. This resulted in smaller tubes being pushed off center toward the side of the rack. The height of the filters, the narrowness of their lumans, and the off-center orientation resulted in pipette crashes on the sides of the master tubes. Eventually Tecan came out with size-specific racks which partially resolved the problem, but added a sort step to our workflow.
TOO MANY ALIQUOTS
One of the areas that frequently causes bottlenecks is front-end specimen handling. The more aliquots required, the larger the bottleneck and the greater delay between the time of receipt and testing time. At first we thought we could pipette from the source tube directly to the testing platform. However, some of the platforms, such as the Chiron ACS180 sample wheel 9, were too bulky. In the case of hepatitis testing, there were just too many different tests to be accommodated by a single platform. We decided to go to testing platforms that made sense, like the Hitachi 747, and later the Centaur 10, and remain with aliquot tubes for hepatitis. These could later be pipetted directly into various microtiter plates by the Tecan 150.
Our initial problem was that each department was pouring a separate aliquot for each test. The chemistry department required five aliquots, one each for the Hitachi 747, 717, HDL testing, Dade ACA Star 11, and ionized calcium. The Immunochemistry department wanted one aliquot for each HbsAg, HbsAb, Hbcore, HCV, HAV total, HAV IgM, ferritin, B12, folate, TSH, and PSA, a total of seventeen separate aliquots. Having had experience with many different processing systems, we realized that this was not a practical solution. The greater the number of aliquots, the greater the bottleneck and less efficient the system will be, choking the Processing department with the large volume of aliquots.
Over the period of time that we worked on this project, our workflow changed. We were able to program the LIS to consolidate aliquots and print test names on the test tubes. The number of aliquots in chemistry was decreased by one. However, the consolidation resulted in a dramatic decrease in testing volume for non-747 tests. This enabled us to aliquot the tubes after 747 testing was completed rather than bringing the system down with additional front end aliquots. The same consolidation was completed in Immunochemistry. Hepatitis was consolidated into a single aliquot, eliminating five aliquots. Consolidation of the Chiron ACS180 into a single aliquot resulted in elimination of an additional four aliquots. As a result, the Tecan only had to aliquot to three stations instead of 17, simplifying the programming needs as well as improving the front-end throughput.
TECAN CLOT DETECTION
Even though the Tecan has clot detection and can identify pipetting failures, manual intervention is required to handle clotted samples. The Tecan has two ways to process clotted samples. It can skip the sample and go on, or it can stop for manual intervention at the time the clot is detected. We chose to stop the aliquoting so that we avoided any chance of contamination as the pipette tips travel over the destination tubes.
BARCODES
With the need to process over 20,000 aliquots in a given night, barcoding all of these empty tubes and placing them in Tecan racks became the next problem to resolve. All laboratories battle repetitive motion injuries. As we progressed with automating the lab, we recognized that we might be left with simple, repetitive tasks that can be condusive to this type of problem. In response, we began a search for a barcode printer that would place the label on the cylindrical surface of a glass test tube.
VS250 AND THE PSD
In early 1998, we located sample handling instrumentation from another manufacturer that had many of the features that we required. Roche 8 had developed two sample handling instruments, the VS250 and the PSD 1200, which were being used in Germany. The VS250 aliquots from primary tubes directly into testing platforms and microtiter plates. The VS250 data manager queries the host LIS to determine the final aliquot destination. There are no barcoded tubes to identify. The PSD 1200 is a simple sorter that accepts tubes, queries the LIS, identifies the order, and sorts the tubes in manner predetermined by the lab. We saw potential for these two instruments, but with some reservations. The limitation of the VS 250 in this laboratory was that it would require to aliquoting into a primary testing platform. In the case of hepatitis, this would delay front end processing. Because of this disadvantage, we felt that the sorting capabilities of the PSD 1200 were not cost-effective with our workflow.
VSII
BMC's most recent entry into the front end automation field, the VSII, combines the aliquoting capability of the VS250 and the sorting capability of the PSD 1200. The instrument integrated a barcode printer, aliquoter and sorter. It applies the label to the aliquot tubes, aliquots sample to the aliquot tube, and sorts the master and the aliquot tubes in a manner predetermined by the lab. This seemed to be a suitable alternative to the Tecan. Fibrin clots and our filters remained unresolved problems.
SORTING FIBRIN CLOTS
The VS II was designed to handle direct tube aliquoting but the height of the pipette tip is not flexible and so a decision had to be made whether to eliminate use of our filters, or to abandon the idea of using the VS II. The VS II's ability to detect and sort clotted samples provided an alternative approach. The data manager of the VS II has the capability of recording and responding when a clot is detected. The barcoded aliquot tube is still made, but master and aliquot tube(s) are sorted in a separate placement area. This makes it easy to manually resolve the clot, filter and pour from the master to the aliquot tubes.
THE OCTOPUS OR THE UNICORN
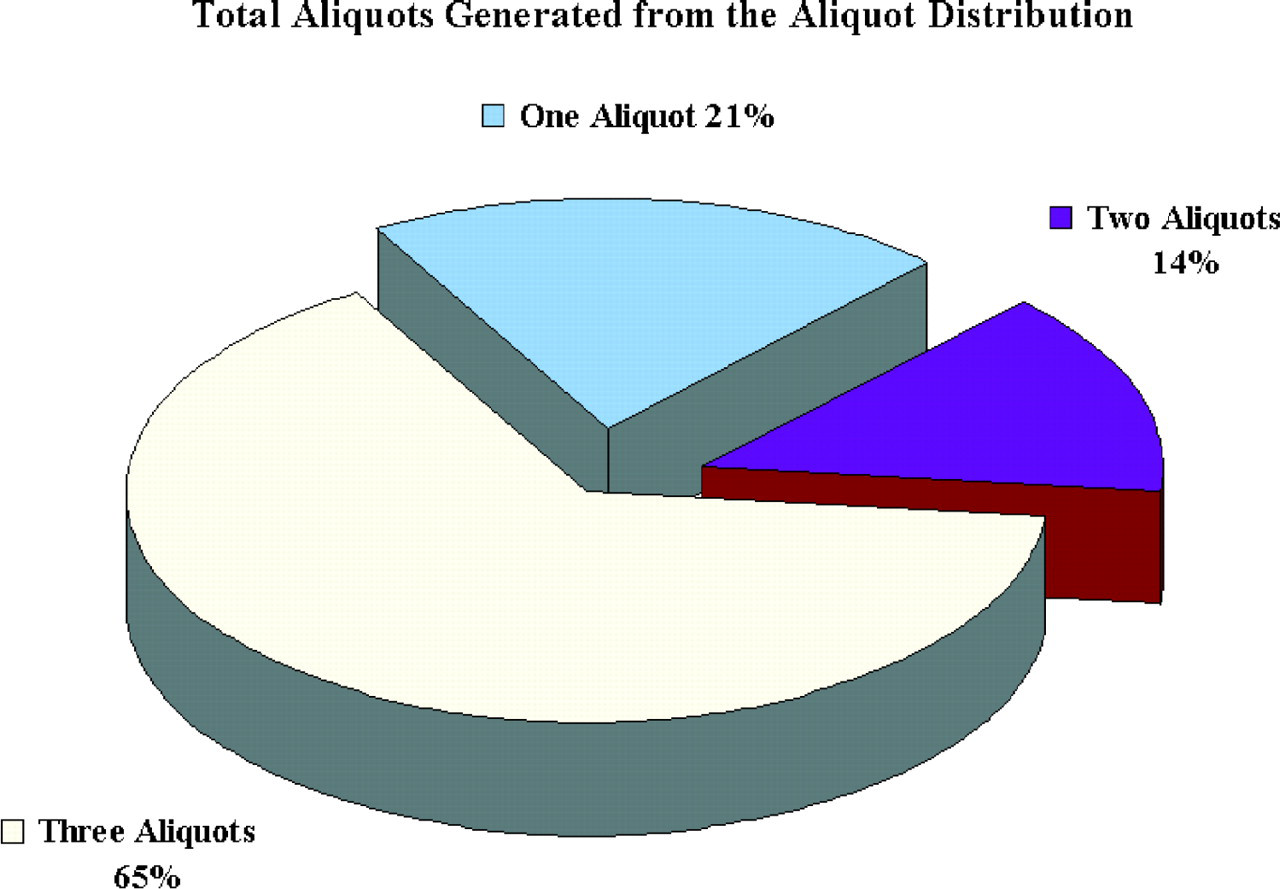
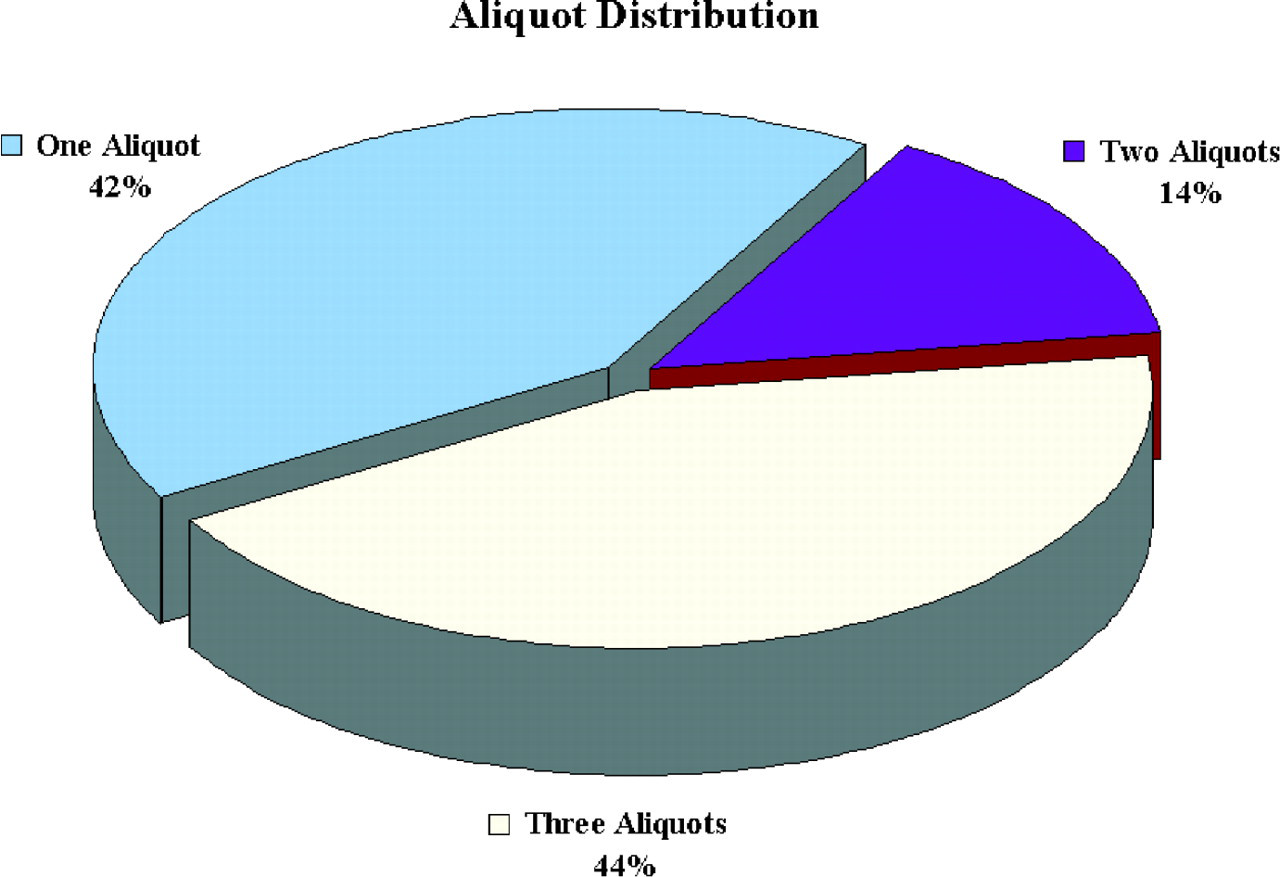
As previously noted, the high number of tests per accession in this specialty results in a large volume of aliquots overall. While our focus on this problem has resulted in a reduction in the number of aliquots, the volume remains high and will be a challenge to any automated aliquoting system. The Tecan Genesis 200 is a high throughput, eight-arm pipettor, while the VSII has a single arm that pipettes each aliquot separately. With either system the throughput decreases as the number of aliquots increases. Based on current volumes, we determined the number of aliquots that would be required on peak days [

Estimated Aliquots on Peak Days
Due to the differences in sample handling, we found that the estimated throughput for each instrument varies with the number of aliquots required [
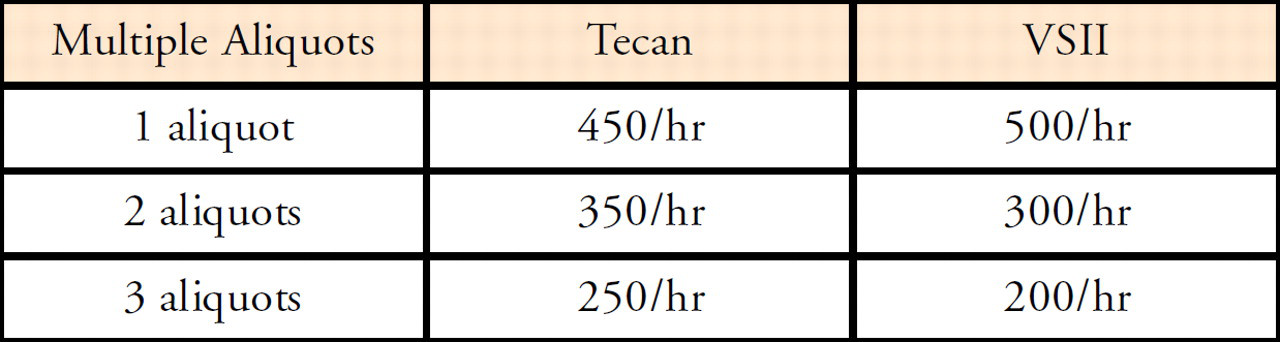
Estimated Throughput with Volume Change
Based on these figures, either five VSII instruments or four Tecan 200 instruments would be required to process this volume of specimens. In addition to requiring fewer instruments, the cost of a Tecan 200 is significantly lower than that of the VSII.
However, the increased cost must be weighed against the VSII's efficiency advantages, such as the ability to barcode and sort samples, especially clotted samples.
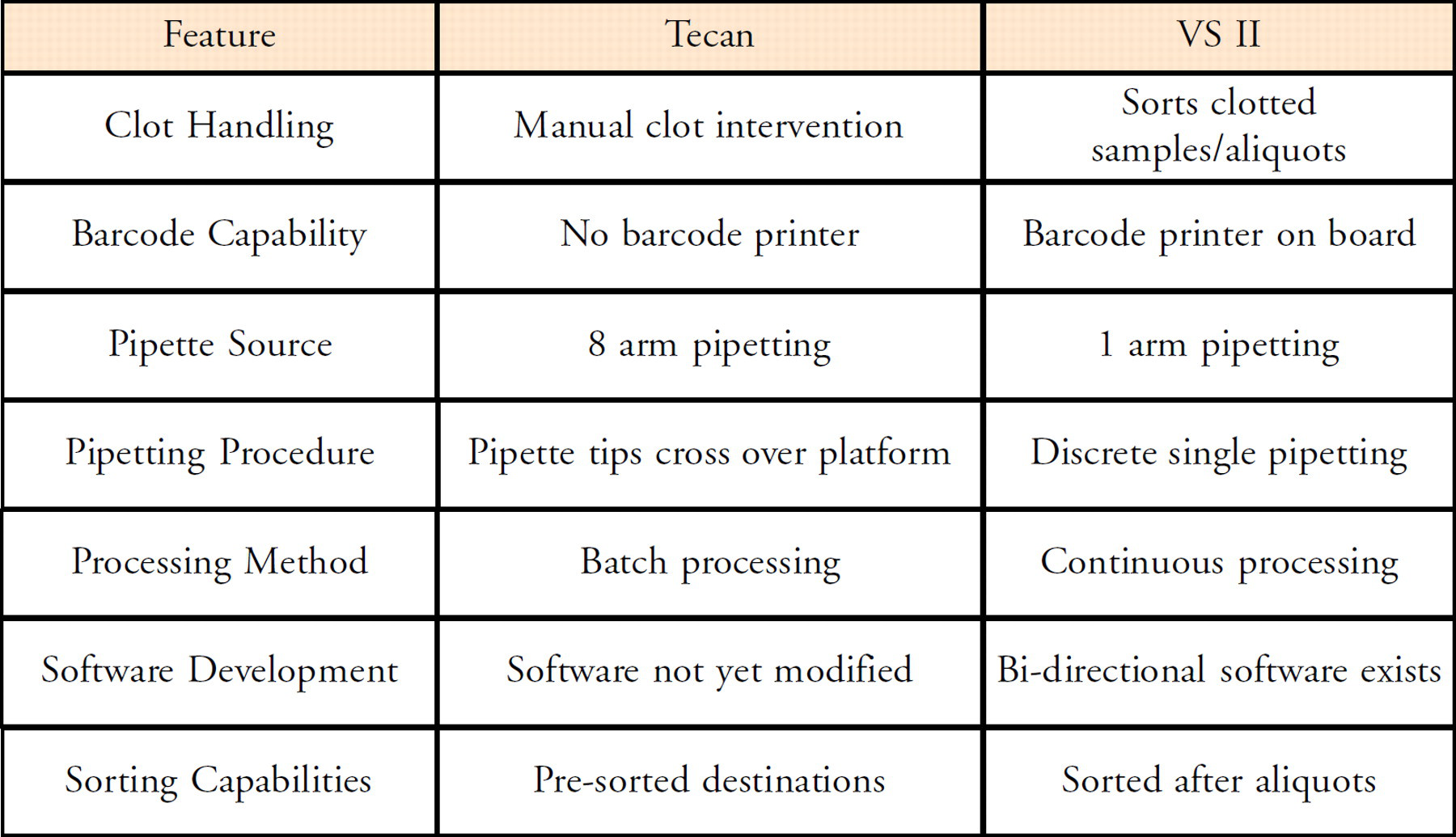
CONCLUSION
Both the Tecan 200 and the Roche VSII systems provide significant enhanced capabilities over our current manual procedures, and address our goals of eliminating mis-pours, minimizing contamination, and increasing efficiency. The Tecan has high throughput and a lower cost per unit. The VS2 has sorting and barcoding capabilities that significantly improve productivity. Both instruments offer viable and affordable alternatives to more expansive TLA systems, and address the unique problems associated with testing dialysis patients' samples.