
Abstract
Abstract
Introduction
The traditional treatment for congenital vertical talus, which involves serial casting and extensive soft-tissue releases, has been associated with severe stiffness and other complications in adolescents and adults. Our hypothesis is that favorable results will be obtained using the Dobbs method of serial manipulation, casting, and limited surgery for vertical talus correction, even in older children and syndromic cases. Therefore, the present study aimed at evaluating the Dobbs method in such cases.
Materials and methods
We treated 15 feet of 10 patients (aged from 1 month to 9 years) using manipulation and serial casting or the reverse Ponseti method followed by percutaneous Achilles tenotomy and limited open reduction of the talonavicular joint. All patients were evaluated both clinically and radiologically in a mean follow-up period of 2 years.
Results
After 2 years, all patients had plantigrade and flexible feet with good radiographic correction. The mean talocalcaneal angle before (70.5° ± 10.5) and after (31° ± 5.2) treatment and the talar axis metatarsal base angle before (60° ± 11.4) and after (15° ± 6.7) treatment were significantly improved (P < 0.001).
Discussion
Recent research has shown that manipulation and serial casting followed by limited surgery (Dobbs method) was successful in treating idiopathic congenital vertical talus. Our results also showed that this method resulted in an excellent outcome in both idiopathic and syndromic congenital vertical talus, even in older children.
Introduction
Congenital vertical talus is an uncommon foot deformity in pediatric patients. The clinical characteristics are convexity of the sole, hindfoot valgus, and abduction of the fore foot [1]. The incidence of this condition is 1 in 10,000 births [1]. The exact etiology of this pediatric deformity is unknown, but genetic factors play a significant role in congenital vertical talus, as approximately 50 % of patients have other neuromuscular abnormalities or known genetic syndromes. Nearly 50 % of the affected children have bilateral involvement, and there is no gender predication [2–4].
Children who are not treated suffer a significant long-term disability. Pediatrics ambulation is usually not affected and delayed, though abnormalities in gait pattern and balance exist [5, 6]. The untreated children have difficulty wearing shoes, due to the abnormal shape of the feet. Pain develops in the early stage of adolescence and later childhood [6, 7].
Historically, the treatment of these patients has been difficult, and they suffer complications in the long term. Experts disagree on the correct approach and the extent of release of soft tissue [8, 9], but most agree that, similar to the treatment of children with clubfoot, the handling of congenital vertical talus begins with serial manipulations and casts. While cast treatment has been viewed as important to stretch contracted dorsal soft tissues, it has not been used by many to achieve correction and avoid more extensive surgery [9–11]. Dobbs described a new method to treat vertical talus using casting and minimally invasive surgery that has been successful for both isolated vertical talus and syndromic vertical talus [12, 13]. This was a less invasive method in correcting the vertical talus, and it has been proved that the method produces more favorable results in the long term than extensive surgical methods [14]. Our hypothesis is that favorable results will be obtained using the Dobbs method followed by proper manipulation and serial casting and then limited surgery, even in older children and syndromic cases. The present study, therefore, aimed at evaluating the Dobbs method in such cases.
Materials and methods
This retrospective study considered five patients with idiopathic congenital vertical talus and five patients with congenital syndromes, such as arthrogryposis and Larsen syndrome, treated at Shohada Hospital of the Tabriz University of Medical Science during the period from 2006 to 2010. None of the patients had received previous treatment (surgical or non-surgical) during admission. The diagnosis of a congenital vertical talus confirmed by the following was the inclusion criteria of the study: (1) a lateral radiography with the foot in maximum plantar flexion demonstrating persistent dorsal translation of the forefoot on the hindfoot caused by fixed dorsal dislocation of the navicular on the head of the talus and (2) a lateral radiography with the foot in maximum dorsiflexion demonstrating a persistently decreased tibiocalcaneal angle, which indicates a fixed equinus contracture of the hindfoot.
In our study, fifteen feet of ten patients with congenital vertical talus using serial manipulation were treated using the Dobbs methods and casting. The deformity after the last casting was controlled relying on radiographic evaluations. The talar axis metatarsal base angle (TAMBA) <30° was appointed as our endpoint for further manipulation and casting. However, if TAMBA ≥30°, the manipulation will be continued and another cast will be applied. After 1 week, radiographic evaluation was repeated. If the angle was decreased in comparison with the previous week's X-ray, the weekly manipulation and casting were continued in order to reach an angle <30°. If there was no further decrease in the angle following further manipulation, our protocol calls for a more extensive, open reduction of the talonavicular joint. In our study, we did not have any such cases. In all cases with TAMBA <30°, therefore, we performed limited open reduction and pinning of the talonavicular joint, followed by a percutaneous Achilles tenotomy. After 6 weeks of casting, the pins were removed and an appropriate brace (according to Dobbs’ study, a pair of shoes with 15° plantar flexion and 15° adduction at the midtarsal joint connected by a metal bar) was prescribed for the patients. This brace was used on the basis of round-the-clock and only during night time for non-walking and walking children, respectively. The latter group used an ankle foot orthosis with the same characteristics as the shoes used by Dobbs while walking [15, 16]. All patients used the brace for 2 years. Finally, clinical and radiological evaluation was repeated for all patients at least 2 years after treatment.
In clinical examination, the foot skin was evaluated for callus formation, breakdown, or pressure areas. A single examiner measured passive plantar flexion and dorsiflexion of the ankle and subtalar motion, as well as varus–valgus heel alignment using a handheld goniometry. Written informed consent was obtained from all the patients’ parents. The Ethics Committee of the Tabriz University of Medical Sciences approved the study. We obtained anteroposterior and lateral radiographs of the feet at the time of presentation, immediately following surgery, and at the time of the final follow-up.
Statistical analysis
The data are shown as the mean ± standard deviation (SD). The Wilcoxon test was used to compare the angles in degrees before and after treatment. The SPSS software program (Statistical Package for the Social Sciences, version 17.0, SPSS Inc., Chicago, IL, USA) was applied for the statistical analyses. In the present study, P < 0.05 was regarded as being statistically meaningful.
Results
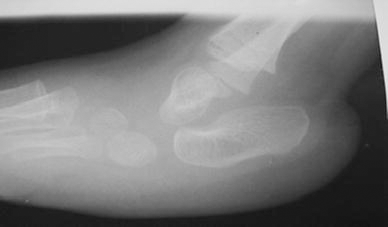
Patients with congenital vertical talus, including 5 (50 %) cases with arthrogryposis and Larsen syndrome and 5 (50 %) patients with idiopathic congenital vertical talus, were evaluated in the present study. The mean age of the subjects was 6.4 ± 2.1 years, varying from 1 month to 9 years. In all cases, the talonavicular joint was reduced following serial manipulation and casting (an average of six times). The minimally invasive approach including pin fixation of the talonavicular joint and heel cord tenotomy was used as well after casting, as described by Dobbs. The TAMBA was below 30°. In children older than 2 years (especially for those older than 6 years of age) and in syndromic patients, correction required further casting (on average, eight castings) and, frequently, general anesthesia was necessary at initial manipulations and castings. In younger children with idiopathic deformities or syndromic cases, there was no need for general anesthesia and casting was repeated, on average, five times. The pre- and post-treatment angle measurements can be found in Table 1, which refers to a significant difference (P < 0.001). Figure 1 shows a pre-treatment clinical picture of a <12-month-old patient's foot, and Fig. 2 shows the plantar flexion radiographic view of the same patient's foot. Figure 3 refers to the foot of an 18-month-old patient after treatment and casting.
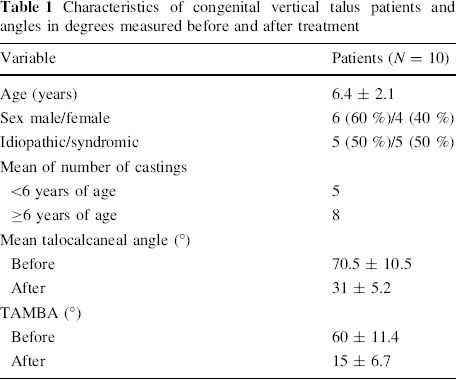
Characteristics of congenital vertical talus patients and angles in degrees measured before and after treatment

Clinical pre-treatment picture of a <12 months old patient

Plantar flexion radiographic view of the <12 months old patient

Clinical picture of an 18-month-old patient after treatment and casting
Figures 4 and 5 show the lateral radiographic images of a 6-year-old patient before treatment and after 6 months of manipulation and casting. A clinical picture of the same patient foot after the final treatment is presented in Figs. 6.
Lateral radiograph of a >6 years old patient before treatment

Six months after treatment and casting in the same patient

Clinical picture of the foot of the same patient
After 18–36 months, all patients were pain-free and had flexible legs and plantigrade feet. Patients wore ordinary shoes with no discomfort. All patients walked without problems, and their radiological evaluations showed no recurrence of deformity. The ankle range of motion was measured clinically, and the average ankle dorsiflexion was determined as 26° (14–28). The plantar flexion was, on average, 16° (12–18). There were no reported complications after casting or during the follow-up period. In our experience, general anesthesia was very useful in children more than 2 years old during the first three manipulations.
Discussion
The goal of the treatment of congenital vertical talus is to restore the normal anatomic relationship among talus, navicular, and calcaneus bones while maintaining a painless plantigrade foot [8].
Historically, manipulation and casting have not been fully effective in correcting congenital vertical talus. According to classical texts and many previous articles, modification of this deformity usually requires releasing a large soft tissue when the patient is 3–4 years old [14, 17]. Subtalar arthrodesis is often required in patients aged 3–8 years, but they experience post-operative stiffness and pain. According to Walker et al. [18], a soft tissue release operation had desirable outcomes in congenital vertical talus. Previous surgical methods have been associated with some complications, including wound necrosis, talar necrosis, under-correction of the deformity, joint stiffness, and pseudoarthrosis. Many of these patients need multiple operations following the primary surgical treatments, such as subtalar and triple arthrodesis, in their future life [18–23]. Also, there is significant controversy about the number and location of ideal incisions to surgically correct the vertical talus, as well as about correcting the deformities in one or two stages. The patients also experience severe limitations of their physical activity [14, 22].
Recent research has indicated excellent vertical talus correction with serial casting followed by a minimally invasive surgery. In the short follow-up time of patients with congenital vertical talus, treatment with serial casting and minimally surgery has excellent results in the correction of deformity [21–24]. Eberhardt et al. show that the Dobbs method is successful in vertical talus treatment [25]. In another new study, similar manipulation and casting before surgery for idiopathic congenital vertical talus has good results [17]. David believed that talipes equinovarus (clubfoot) and vertical talus were successfully corrected with manipulation therapy and minimally invasive Achilles tenotomy [11].
In their study, Dobbs et al. [15] evaluated a new method of treating idiopathic congenital vertical talus using serial manipulation and casting, followed by pinning the talonavicular joint and performing percutaneous tenotomy of the Achilles tendon in 19 feet. Their study showed excellent results in the clinical appearance of the foot, its function, and deformity correction, as measured by radiographic measurements over a period of 2 years [15].
In this study, we used the reverse Ponseti method to correct deformity in the talonavicular joint. Our results were comparable to those achieved from previous studies without opening the talonavicular joint. We reviewed studies in medical publications and found that 4 years was the highest age during which these methods were implemented for idiopathic congenital vertical talus [23–25], but we treated 5-, 6-, 7-, and 9-year-old patients with congenital syndromes like arthrogryposis and Larsen syndrome. This method was effective in all of the mentioned patients and can also be applied to vertical talus associated with genetic syndromes and neuromuscular conditions with a similar rate of success [26]. Researchers have recently been inspired by the Ponseti method of treating clubfoot, and they developed the reverse Ponseti procedure with manipulation and casting in the talonavicular joint, pinning, and percutaneous Achilles tenotomy (called the Dobbs method), which have shown very good results with favorable short-term follow-up periods [27]. Bhaskar treated four feet among 1-month-old patients suffering from congenital vertical talus using serial manipulation and casting, Achilles tenotomy, and percutaneous pinning of the talonavicular joint, and indicated the usefulness of following this procedure in preventing the need for extensive future surgery and producing desirable results [27].
Limitations
Due to the short follow-up time, there were some limitations in this study, such that the long-term outcomes are unknown. The small sample volume, heterogeneous cohort, and lack of a comparative cohort were other important limitations of the study. The mentioned limitations were inevitable because of the low incidence of vertical talus. Therefore, it is recommended to conduct a multicenter evaluation among syndromic cases with more patients using this method.
Conclusion
Using the reverse Ponseti method of closed manipulation and then limited open reduction and fixation with a pin in the talonavicular joint and percutaneous Achilles tenotomy, favorable results were obtained. It was an effective treatment method even in older children and those with non-idiopathic congenital vertical talus. There were also fewer complications compared to extensive operative treatments.