
Abstract
Early studies show hysterectomy is a main surgical choice for cervical agenesis with excellent outcomes. However, as time went on more literature showed successful uterovaginal anastomosis performed in cervical agenesis. This case report wishes to highlight the management of the patient with complete vaginal and cervical agenesis, which presented with acute abdominal pain due to severe extension of the uterus. We aim to explore options and dilemmas in preserving reproductive function in such cases. A 13-year-old child was presented with acute abdominal pain and primary amenorrhea due to suspected vaginal agenesis. Physical examination revealed fundal height equal to 20 weeks of pregnancy. The vagina has no introitus and the external urethral meatus was normal. Abdominal ultrasound revealed a hematometra with the size of 8.84 × 3.12 cm accompanied by hematosalpinx on both fallopian tubes. The patient then undergoes an emergency hysterectomy. During the operation, it was found the cervix was substituted with the muscular part of the uterus with a little part of connective tissue part with no cardinal ligaments. Earlier articles showed hysterectomy is the first line of treatment in cervical agenesis. However, with the advancement of surgical techniques conservative treatment was made possible and reported in several case reports. According to European Society of Human Reproduction and Embryology (ESHRE) classification, our patient is classified as U0-C4-V4 (complete vaginal and cervix agenesis). We opted for a hysterectomy in this patient due possibility of fertility being slim and acute abdominal pain relief. Performing such a difficult operation in our setting requires expert meetings, and tool preparation also an amniotic graft for neovagina which in our case we could not afford due to the acute abdominal pain the patient experienced, and the patient’s adamant wish for a hysterectomy. Hysterectomy remains a safer approach in low-resource settings with excellent postoperative outcomes. However, reconstructive surgery is an option that should be offered with its own risks and benefits.
Introduction
Mullerian abnormalities in females are a common benign condition with a prevalence of 4%–7%. 1 However this condition could cause many problems ranging from infertility, amenorrhea, or acute abdominal pain due to menstrual outflow tract disruption. From all mullerian anomalies, cervical agenesis is a rare congenital condition that occurs in 1 in 80,000 to 100,000 births. 2 Vaginal agenesis usually occurs in cases of cervical agenesis with a prevalence rate of 50%. 3 Early studies evaluating surgical approaches in cervical agenesis showed patients with hysterectomy had no complications and needed no further laparotomy compared to patients who underwent uterovaginal anastomosis procedures.4,5 However as time goes on more literature shows successful uterovaginal anastomosis performed in cervical agenesis.6,7 This case report wishes to highlight the management of the patient with complete vaginal agenesis and cervical agenesis which presented with acute abdominal pain due to severe extension of the uterus, discuss our choice to perform hysterectomy rather anastomoses, also available choices in low-resource settings. We aim to explore options and dilemmas in preserving reproductive function in such cases with available modalities.
Case report
A 13-year-old child was referred to Urogynecology Department with primary amenorrhea due to suspected vaginal agenesis. Patient had increasing abdominal pain since 6 months before admission which is cyclical however the pain has persisted since 2 months ago until now. Patient said the pain in the last 3 days has been unbearable and prevented the patient from doing daily activities. The patient was Tanner stage 3 for both her pubic hair and breasts. Physical examination revealed fundal height equal to 20 weeks of pregnancy. On external genitalia examination, it was revealed the vagina has no introitus and external urethral meatus were normal. At rectal toucher examination cervix couldn’t be identified and bulging from the uterus was present (Figure 1).
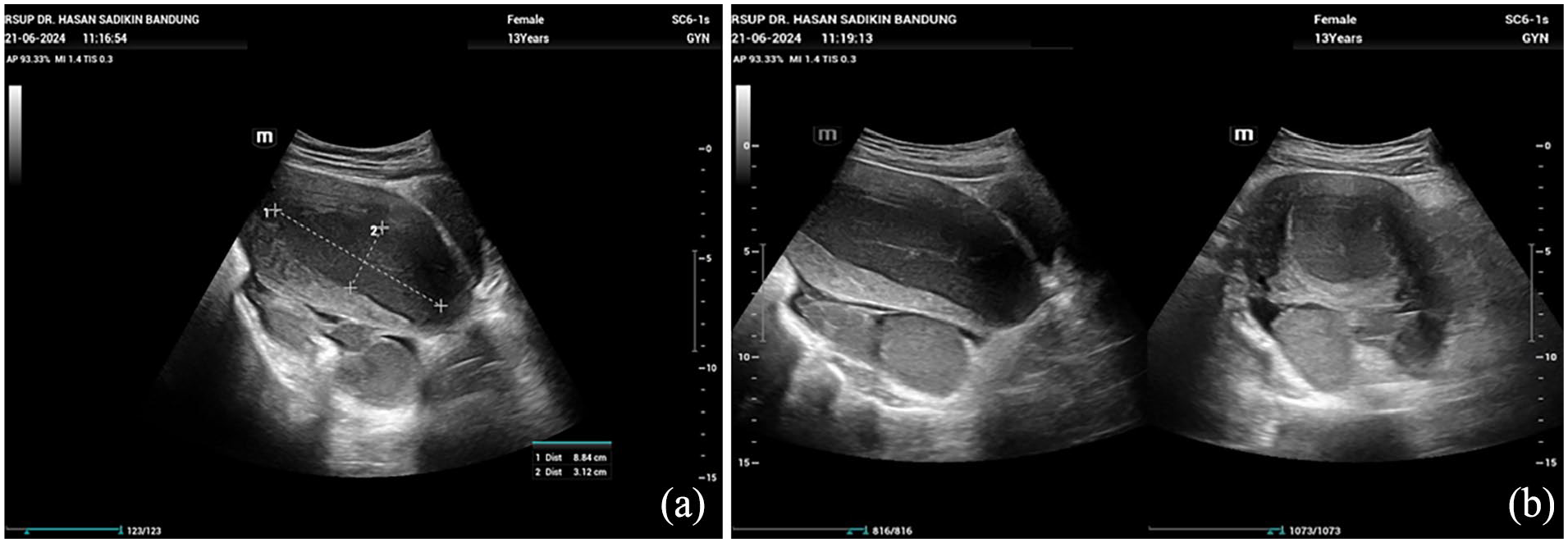
Patient abdominal ultrasonography. (a) Hematometra showing volume of 8.84 × 3.12; (b) sagittal view showing both fallopian tubes filled with blood.
Abdominal ultrasound revealed a hematometra with the size of 8.84 × 3.12 cm accompanied by hematosalpinx on both fallopian tubes. Cervical and vagina structures could not be identified. The patient was then diagnosed with acute abdomen due to hematometra and hematosalpinx resulting from cervical and vaginal agenesis. The patient and her family have been informed the possibility of anatomy restoration is slim and a hysterectomy would be performed. Patient also decided on future vaginoplasty when she decided to get married.
Emergency laparotomy was performed, and a hysterectomy was conducted after no cervix and vaginal structure was identified. Uterus was enlarged at 20 weeks of pregnancy and the bilateral fallopian tube was also enlarged. When approaching cardinal ligaments were not present (Figure 2).
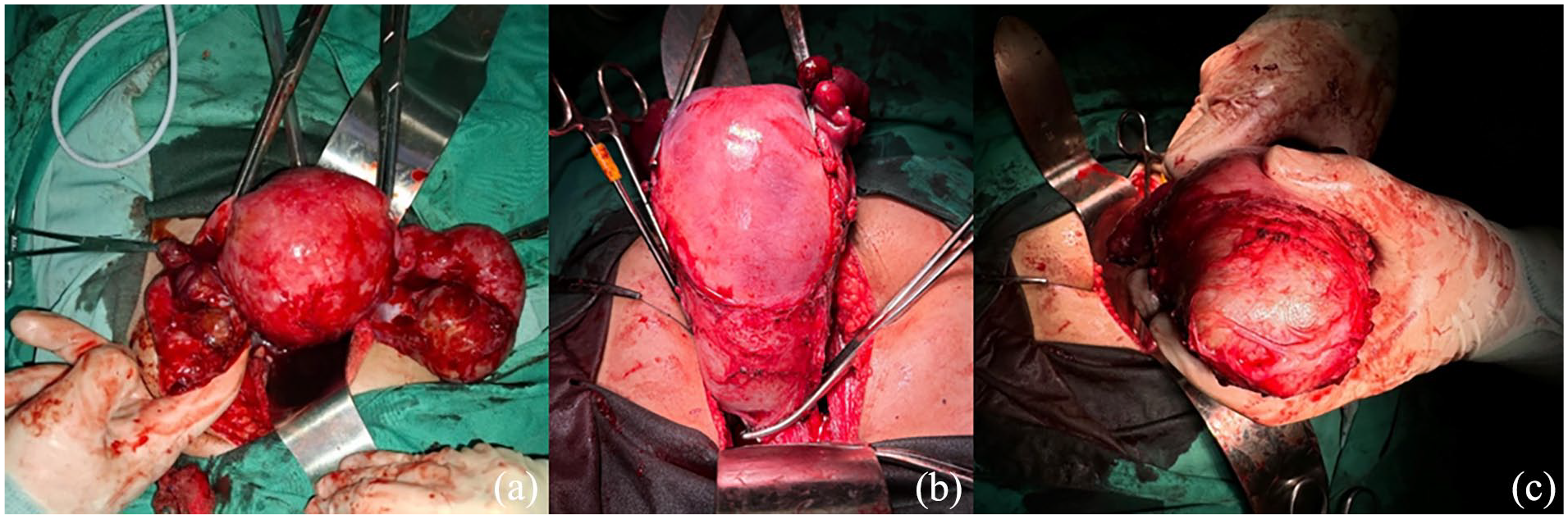
Intraoperative findings. (a) Hematometra alongside bilateral hematosapinx; (b, c) cervical structure was not present and uterus ended/closed with muscle part in the uterine outlet.
Specimen was identified outside and if was further identified the cervix was substituted with the muscular part of the uterus with a little part of connective tissue part (Figure 3). Brownish liquid which is menstrual blood estimated at 400 cc was evacuated from the uterine cavity.

Specimen after operation. (a) Enlarged uterus and bilateral salpinx due to retained menstrual products; (b) uterine after incised revealed no uterine ostium and retained menstrual blood.
Pathology anatomy analysis reveals bilateral hydrosalpinx and mullerian aplasia, as ½ lower uterine corpus shows no endometrium and is composed only of fibromuscular tissue. At the ward, after the operation was over, she felt relieved due to abdominal pain which occurred to her was not present anymore. On physical examination everything was normal. We also explained the surgical results to her parents and patient, and they understood the patient’s reproductive function could not be restored but she remains active hormonally and not in a menopausal state.
Patient came to Urogynecology Policlinic 2 weeks and a month after the operation, she has no additional symptoms and continues her daily activity. We contacted the patient 3 months after the operation to assess physiological changes that could occur after the operation. Patient said she has not experienced any changes in activity level and does not feel unhappy. She and her parents also felt satisfied with the outcome of the operation.
Discussion
Earlier articles showed hysterectomy is the first line of treatment in cervical agenesis. This step is considered based on the high recurrence level of risks and morbidity of reoperation for re-obstruction, re-stenosis, and infection.4,8 Possibility of fertility restoration remains slim due to the destruction of normal histologic features of the fallopian tube and uterus. Incidence of reoperation and subsequent hysterectomy in those undergoing uterovaginal reconstruction ranged up to 50%, with several deaths reported from sepsis. 9
However, with the advancement of surgical techniques conservative treatment was made possible and reported in several case reports.10,11 Deffarges et al. studies in 2001 show spontaneous pregnancy are possible after conservative management was performed, 10 of 18 patients had spontaneous pregnancy and cesarean section was performed later. 12 Newer case reports and follow-up study show laparoscopic-assisted uterovaginal anastomosis with concomitant vaginoplasty is possible and only one patient underwent hysterectomy, owing to restenosis and infection. 13
According to ESHRE classification, our patient was classified as U0-C4-V4. 1 This means the patient had complete vaginal and cervical agenesis. Even though laparoscopic uterovaginal anastomosis and concomitant neo-vaginoplasty were an option, the risk of reoperation is still there and should be considered and the surgery should only be performed by a specialized team with the required expertise in minimally invasive surgery. 6 For performing such a difficult operation in our setting requires an expert meeting, and tool preparation as well as an amniotic graft for neovagina which in our case we couldn’t afford due to the acute abdominal pain the patient experienced. We opted for a hysterectomy in this patient for several reasons, first the uterus is severely distended equal to 20 weeks of pregnancy, and hematosalpinx is also present, the possibility of fertility in this patient is rather slim. Second, the patient herself and her family adamantly opted for radical therapy due to her chronic abdominal pain which is exacerbated every month.
Padmawar in his publication showed steps of laparoscopic uterovaginal anastomosis for cervical agenesis, which involve uterine incision and drainage of hematometra continued by incision over the vaginal vault and placement of a Silastic Foley catheter as a stent between vagina and uterine cavity continued by uterovaginal anastomosis over the Foley catheter by placement of series of 2-0 Prolene sutures. 6 This alone already a complex procedure for cervical agenesis, however with vaginal agenesis (V4) it’s would be difficult to identify the cervical border as no vaginal vault present.
Management of cervical anomalies still remains controversial, as later result contradicts early studies. 9 When deciding on the appropriate procedure for the individual patient, the following questions should be considered: (1) Is the uterus large enough to sustain a pregnancy; (2) is there a cervical segment present (i.e., cervical dysgenesis vs. agenesis); (3) is the vagina developed; and (4) is the patient able to contribute to the decision-making process. 5 In our case, even though the uterus was deemed large enough to sustain a pregnancy, no cervical segment was present and she is adamant that she would rather have a hysterectomy rather than wait for laparoscopic uterovaginal anastomosis.
Conclusion
Hysterectomy remains a safer approach in low-resource settings with excellent postoperative outcomes. However, hysterectomy does not allow for the individual to preserve her uterus for cultural or emotional reasons or to carry a pregnancy. Due to this reason, reconstructive surgery is an option that should be offered with its own risks and benefits.
Take-home message
Hysterectomy remains a safer approach in low-resource settings; however, reconstructive surgery is an option and should be offered to patients and families.
If the patient presented with only amenorrhea without severe abdominal pain, laparoscopic uterovaginal anastomosis, and concomitant neo-vaginoplasty in such case with careful planning and expert operation team.
Early diagnosis in cervical and vaginal agenesis is adamant to prevent aggressive treatment such as adnexectomy or hysterectomy.
Footnotes
Acknowledgements
None.
Author contributions
M.R.A.S. was the attending consultant for the patient involved. M.R.A.S. was the examiner and M.W. was a trainee for the patient involved. M.W., A.Z.S., W.R., and M.R.A.S. conceived the design for this case report, collected the data, and interpreted the patient case notes. M.W., A.Z.S., and W.R. wrote the draft. M.R.A.S. directed and supervised the case report. M.W., A.Z.S., W.R., and M.R.A.S. agreed to the following version of the manuscript for publication.
Availability of data and materials
Not applicable
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study is exempted from an ethical approval as determined by the institutional and department review board.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Registration of research studies
Registration of research is not applicable in our case