
Abstract
Abstract
Purpose
This case report presents a new and unique surgical greater trochanter split procedure for reconstructing a hip joint after an infantile hip sepsis with consequent aplasia of the femoral head.
Methods
One patient underwent the new trochanter split osteotomy for postinfectious aplasia of the femoral head at the age of 4 years. A follow-up of 17 years is presented.
Surgical technique
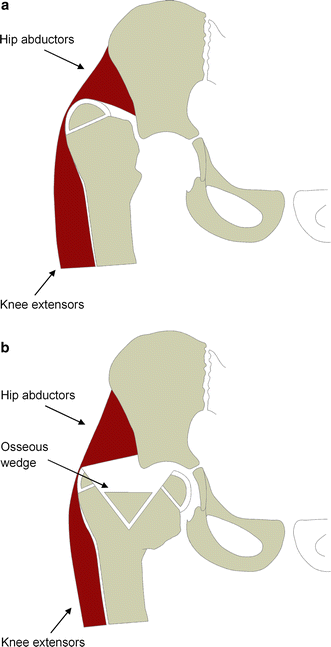
The remaining proximal femur is sagittally split and the medial part is shifted into the acetabulum, preserving the lateral part of the greater trochanter. The osteotomy is fixed by an osseous wedge and K-wires. In contrast to the techniques known so far, it does not harm the vastogluteal muscle sling, thus, significantly reducing abductor lurch. Furthermore, through placing juvenile growth cartilage from the greater trochanter area into the acetabulum, there is, by far, more potential for the regeneration of a femoral head than by the procedures known so far.
Conclusion
The presented surgical technique is able to improve the biomechanics of a hip joint with postinfectious aplasia of the femoral head. The growth of a new femoral head and the development of a well-shaped acetabulum is enabled. A clinical outcome with a stable joint and very good clinical function can be achieved.
Keywords
Introduction
As a result of an infantile hip sepsis or an osteomyelitis of the proximal femur, patients sometimes develop a postinfectious dislocation of the hip and a complete aplasia of the femoral head. This frequently leads to both a severe abductor lurch caused by the loss of femoral offset and tension of the gluteal abductor sling and shortening of the affected leg. Besides a conservative regime, several surgical procedures also exist. All of these aim to partially or totally reconstruct the hip joint to reacquire physiological function by reducing leg shortening and regaining an adequate offset to reduce abductor lurch. Furthermore, surgical treatments attempt to create anatomic conditions that allow a total hip replacement in the future [1–5]. In the literature, four surgical procedures are currently described: The subtrochanteric angulation osteotomy, in which the lesser trochanter is shifted into the acetabulum as a substitute for the femoral head. Shifting the greater trochanter into the acetabulum to achieve a varisation of the proximal femur. The hip abductors are reattached to the lateral femur periosteum in this procedure [6]. L'Episcopo's technique, in which the remaining part of the femoral head, which lacks a cartilage layer, is shifted into the acetabulum [7]. The modified Albee arthroplasty, in which the medial part of the sagittally split proximal femur is shifted into the acetabulum, the greater trochanter is resected and the hip abductors are reinserted at the lateral femoral periosteum [8].
In the literature, meaningful long-term results for the first three of these techniques are unavailable. Only the modified Albee arthroplasty is mentioned in an actual publication, in which long-term results over 10 years are presented [8].
In the following case report, an alternative surgical procedure addressing an infantile postinfectious aplasia of the femoral head (Choi type IVB) [5] and a well-documented follow-up of 17 years is presented. The method described here is distinctive because, as a result of the sagittal split of the cartilaginously preformed greater trochanter, a fully blood-supplied osteochondral fragment can be placed into the acetabulum.
Method
Through a ventral surgical approach, the acetabulum is exposed and debrided of postinfectious scar tissue. After that, the remaining stump of the proximal femur, with its apophysis of the greater trochanter, is split sagittally, placing the medial part, including half of the apophysis, into the acetabulum as a substitute for the femoral head. Distally, the medial cortical bone of the proximal femur is not completely separated but only bent, thus, producing a greenstick fracture. The lateral part of the greater trochanter including the preserved vastogluteal sling and the lateral part of the apophysis remains in situ. According to the anatomical pattern of attachment of the gluteal musculature at the femur, the attachment area of the gluteus medius muscle is preserved, while the gluteus minimus muscle is removed and reattached to the gluteus medius muscle [8]. The gap between both parts of the greater trochanter is filled with a bone wedge taken from the iliac crest. Osteosynthesis is performed using K-wires transfixing the medial and lateral part of the split greater trochanter, as well as the bone wedge and the medial half of the acetabulum.
Case report
A patient had suffered from a bacterial coxitis on the left side caused by an infantile sepsis. This resulted in complete destruction and aplasia of the femoral head and the femoral neck, while the greater trochanter remained (Figs. 1a and 2a). The patient was 4 years old at the first consultation in our hospital. The proximal femoral stump was found dislocated far proximal, which led to a leg shortening of 4 cm. Clinical examination showed a pronounced Duchenne limp with additional adduction and shortening components.
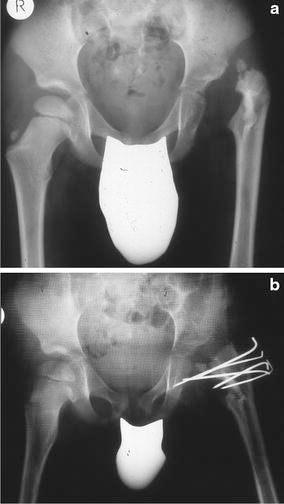
We performed a trochanter split osteotomy using the procedure explained above (Figs. 1b and 2b). After surgery, leg shortening of 2 cm remained, as well as a flexion contracture of the hip of 20° and a moderate Duchenne limp. Compared to pre-surgery-conditions, gluteal muscular insufficiency was significantly reduced.
Following surgery, a large, well-functioning femoral head substitute formed. At the age of 7 years, a stiff pseudarthrosis of the regenerated femoral neck developed (Fig. 3a).
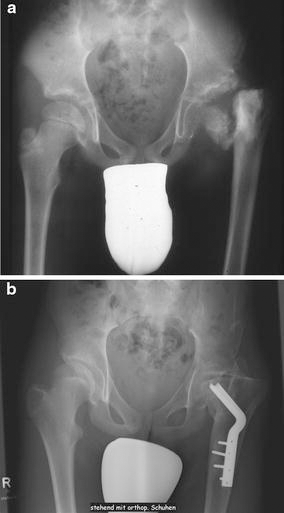
The pseudarthrosis completely healed after we performed a subtrochanteric valgisation osteotomy at the age of 11 years (Fig. 3b). At the age of 16 years, the remaining leg shortening of 4.5 cm was addressed with a lower leg lengthening procedure using an Ilizarov fixator. At the present time, a slight Duchenne limp and a slightly positive Trendelenburg's sign remain (Fig. 4a). The range of motion of the hip joint is currently extension/flexion 0°–20°–50° and abduction/adduction 20°–0°–20°. Rotation of the hip is hardly possible, and there is a contraction in external rotation of 15°. The total leg shortening is 1 cm; measured at the patella, the femur is 4 cm short. X-rays show a large, well-articulating femoral head in the nearly correct anatomical position (Fig. 4b). We found a slightly raised greater trochanter, while the former pseudarthrosis of the femoral head is no longer visible. The patient is able to walk completely free of pain. He swims competitively and frequently cycles long distances. The only compromising symptom in everyday activities is the limitation of hip flexion to 50°, which makes sitting on standard chairs difficult. In his job as an IT specialist, our case is planning to use a chair designed for patients with a hip arthrodesis.

Discussion
Our proposed surgical technique combines the advantages of the existing methods while avoiding their disadvantages. In contrast to the classical arthroplasty of the greater trochanter and the modified Albee arthroplasty, the vastogluteal muscle sling is preserved and there is no need to reattach it to the periosteum of the lateral femur. Thus, the risk of gluteal muscular insufficiency caused by surgery is greatly reduced. Among the established methods, only the arthroplasty of the greater trochanter places apophyseal cartilage of the greater trochanter into the acetabulum, while the other techniques place only bone tissue into the acetabulum. It is well known that apophyseal cartilage tissue is able to differentiate according to the given local load conditions and, therefore, compared to bone tissue, there is a higher ability to reconstitute a new femoral head [9, 10]. Our surgical procedure shifts the medial half of the greater trochanteric apophysis into the acetabulum and, thus, makes use of this advantage. Nevertheless, at present, the regeneration of hyaline cartilage covering the newly grown femoral head can only be presumed according to the above-mentioned facts. A histological examination of the remaining cartilage should be done when the femoral head is resected while performing a total hip replacement in the future.
The surgical procedure presented above is unique in that it simultaneously preserves the vastogluteal sling and places greater trochanteric apophyseal cartilage tissue into the acetabulum, creating perfect conditions for the reconstitution of a femoral head while minimising abductor muscle insufficiency as a result. By shifting the apophysis, a replacement for the epiphyseal growth plate is created, making the growth of a new femoral neck and, thus, a physiological offset of the hip, possible. By restoring normal biomechanics of the hip and enabling the growth of a new femoral head, also, the development of a well-shaped acetabulum is made possible, as the shape of the acetabulum is mainly determined by the biomechanical conditions during the growth period. Unfortunately, the presented procedure was not able to prevent the development of a pseudarthrosis of the femoral neck.
However, it remains unclear as to whether our patient developed the pseudarthrosis of the femoral neck as a result of a mechanical overload of the new growth plate leading to a pseudarthrosis. Due to the dislocation of the proximal femur and the already 4-year-long course of disease when we started therapy, our patient had already suffered from an insufficiency of the hip abductors that could not be completely corrected through surgery. According to the model of the vastogluteal muscle sling, this leads to increased shear force in the proximal direction on the proximal femur, which might have been the reason for the shearing off of the apophysis [11, 12]. If so, this problem could be addressed by performing an additional valgisation osteotomy of the proximal femur to equilibrate forces. Another factor for developing a pseudarthrosis of the reconstituted femoral neck might be the reduced growth in thickness in the region of the open-wedge osteotomy, which is caused by the absence of the growth–cartilage cap in this area. The absence of growth cartilage leads to an absence of growth in thickness where the osteotomy was performed, creating a mechanical weak point [13]. According to the anatomical findings of Gautier et al., the sagittal split of the greater trochanter and the greenstick fracture distally do not affect the blood supply of the femoral neck and head, as the medial femoral circumflex artery and its deep branch are not affected [14]. Thus, we assume that the pseudarthrosis of the femoral neck was not caused by a lack of blood supply.
Our operation led to a highly satisfying long-term result. In his daily activities, our patient is completely free of pain and is able to participate in ambitious sporting activities. The range of motion of the hip joint is satisfactory and pain-free. Through surgery, we created the perfect conditions for a total hip replacement in the future by restoring the anatomically correct shape of the proximal femur and the acetabulum, and a well-functioning vastogluteal muscle sling.
Based on the anatomical and functional aspects of a hip joint and our clinical and radiological findings, we consider our surgical procedure to be highly promising for addressing the problem of postinfectious aplasia of the femoral head in children. Reconstruction surgery should be performed as early as possible because the earlier the biomechanics of the hip joint can be optimised, the more normal a development of the hip joint can be achieved. Certainly, to enable further clinical and statistical analyses, a larger case series is needed.