
Abstract
Purpose
To determine if the detection of musculoskeletal pathology in children with a limp or acute limb disuse can be optimized by screening with blood tests for raised inflammatory markers, followed by MRI.
Methods
This was a prospective observational study. Entry criteria were children (0 to 16 years of age) presenting to our emergency department with a non-traumatic limp or pseudoparalysis of a limb, and no abnormality on plain radiographs. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) blood tests were performed. Children with ESR > 10 mm/hr or CRP > 10 mg/L underwent a MRI scan. When the location of the pathology causing the limp was clinically unclear, screening images (Cor t1 and Short Tau Inversion Recovery) of both lower limbs from pelvis to ankles (‘legogram’) was undertaken. Data was gathered prospectively from 100 consecutive children meeting the study criteria.
Results
In all, 75% of children had a positive finding on their MRI. A total of 64% of cases had an infective cause for their symptoms (osteomyelitis, septic arthritis, pyomyositis, fasciitis, cellulitis or discitis). A further 11% had positive findings on MRI from non-infective causes (juvenile idiopathic arthritis, cancer or undisplaced fracture). The remaining 25% had either a normal scan or effusion due to transient synovitis. ESR was a more sensitive marker than CRP in infection, since ESR was raised in 97%, but CRP in only 70%.
Conclusion
In our opinion MRI imaging of all children with a limp and either raised ESR or CRP is a sensitive method to minimize the chance of missing important pathology in this group, and is an effective use of MRI resources. We advocate the use of both blood tests in conjunction.
Level of Evidence
Level II
Introduction
It is not uncommon for children to develop a limp of spontaneous onset, without preceding trauma and without any abnormality visible on radiographs.1–4 Other children can develop disuse of an upper limb, sometimes termed pseudoparalysis. A proportion of cases will have a benign cause that does no harm and will resolve spontaneously given time. These include swollen lymph glands or muscle aches from viral illness, and transient synovitis.5,6 However, other causes of limp and pseudoparalysis include bacterial infections such as septic arthritis, osteomyelitis, pyomyositis, fasciitis, cellulitis and discitis. Rheumatological diseases such as juvenile idiopathic arthritis and acute rheumatic fever can present with a limp, as can malignancies such as sarcoma and leukaemia.1–4
While there has been some helpful research investigating effective methods to diagnose septic arthritis, 7 there has been very little work targeted towards the early detection of other conditions that may cause a limp in children. Indeed, investigation of a child with a limp is based upon consensus rather than research trials.1–4 Furthermore, the current approach is not very sensitive and milder cases of musculoskeletal pathology are frequently missed at their first presentation. 8
It would be a major step forward if we could develop a simple method of determining which children can be safely discharged from the emergency department, and which need admission for further investigation. We could then cut down on unnecessary hospital admissions for observation, while detecting pathological conditions at an early stage. The aim of this study is to determine whether we can use ESR and CRP blood tests to identify which of those children with a limp have a high likelihood of suffering with a serious pathology requiring treatment.
Patients and methods
The inclusion criteria for this prospective study were all children aged 0 to 16 years who presented to the emergency department of our hospital with a distinct limp of spontaneous onset, refusal to weight bear at all on one leg, or pseudoparalysis of the upper limb. A limp was defined as new onset asymmetry in the length of stance phase, compared with the normal walking ability of that child. Those with abnormalities on plain radiographs (such as fractures, Perthes’ Disease or slipped upper femoral epiphysis) were excluded from the study. The children underwent assessment with history, examination and plain radiographs, as well as blood tests including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) to detect pathology causing inflammation. A CRP over 10 mg/L or ESR over 10 mm/hr is regarded as an abnormal result in children and young adults. 9 Limping children with raised ESR or CRP were admitted and an MRI organized. Children with normal ESR and CRP were not included in the study and were allowed home as likely having transient synovitis, muscle aches or swollen lymph glands from a viral infection, and were reviewed in a paediatric fracture clinic the following week to ensure they were settling.
Children under the age of seven years had their MRI under general anaesthetic to ensure movement artefact did not adversely affect the quality of the images taken, but this was not required in older children. All children were imaged on a General Electric 1.5T HDXT MRI scanner (General Electric Company, Boston, Massachusetts). When the location of the pathology was clear from pain or tenderness, just that area was imaged. The standard imaging protocol for these children was three plane T1 and Short Tau Inversion Recovery (STIR) imaging with 3.5-mm slice thickness and 0.3-mm interspace covering the area of concern. Images were reviewed by a consultant radiologist (AL) prior to the end of the scan to ensure that there was adequate coverage of pathology.
When the location of the pathology was unclear due to the young age of a child then screening images (T1 and coronal STIR 3.5-mm slice thickness with 0.3-mm interspace) were taken of the pelvis and both legs for limping children (which we term ‘the legogram’), and of the entire arm for pseudoparalysis. These images were reviewed by a consultant radiologist (AL) and focused imaging was then undertaken of areas where abnormal fluid in bone, joint or soft tissues was detected on that screening STIR image, usually axial and sagittal T1 and STIR images. Contrast was only given in cases where imaging findings were equivocal and in cases of discitis to assess for epidural collections. The MRIs generally take about 30 to 40 minutes. If a limping child without signs to localize the pathology had a normal legogram scan, then the spine was subsequently imaged. Abnormalities on MRI were diagnosed using standard published criteria.10–13
Diagnostic criteria
Osteomyelitis was identified on MRI by the presence of bone oedema that did not follow a linear pattern (which is suggestive of fracture), periosteal oedema, subperiosteal collection and Brodie's abscess. Septic arthritis was suspected by the presence of a joint effusion, synovial oedema and inflammation in the surrounding pericapsular structures and muscles. Pyomyositis was identified by oedema within muscle bellies, abscess within a muscle and fluid within the muscle compartment. Fasciitis was indicated by oedema and fluid tracking in the plane deep to the fat but superficial to the muscle compartments. Discitis was identified by oedema within a disc and adjacent vertebral bodies, fluid collection under the anterior longitudinal ligament, collapse of the disc and bony destruction adjacent to the disc. Juvenile idiopathic arthritis was suspected by the presence of a florid effusion, thickened synovium with abnormal infolding and joint surface erosion but no inflammation in the surrounding muscles. Transient synovitis was suspected by the presence of a small to moderate effusion, no synovial thickening or infolds and no oedema in adjacent muscles or bone.
When a joint effusion was identified, the underlying pathology was determined following surgery. Tests performed included cell count and microbiological culture of joint fluid, and both histology and microbiological culture of synovial biopsies.7,14 Septic arthritis was diagnosed where bacterial organisms were visible on microscopy or cultured from the joint fluid, where joint fluid was thick in consistency and where cell count was > 50 000 white blood cells (WBCs) per mm 3 of fluid. Transient synovitis was diagnosed where no organisms were viewed on microscopy or cultured from joint fluid, where the cell count was < 50 000 WBCs per ml, where synovial fluid was transparent yellow in colour, where synovial biopsy showed no or slight inflammation on histology and where symptoms resolved spontaneously without the need for antibiotics. Juvenile idiopathic arthritis and other rheumatological diseases were diagnosed by absence of bacteria on microscopy and culture, by a florid joint effusion that was yellow in colour, by inflammatory changes on histological examination of the synovium and failure of antibiotics to improve symptoms.
The use of this data for research purposes has been approved by the UK Health Research Authority (IRAS project ID 244657, REC reference 19/HRA/0013).
Results
The study started in February 2010 and data collection was completed in August 2015, when 100 consecutive children presenting with a limp or pseudoparalysis and abnormal inflammatory markers were included. A mean of 18.2 children were admitted to the study each year, and our hospital has a catchment area of around 400 000 people. The length of time the limp had been present was described by the parents as a range from ‘about four weeks’ to the same day as the presentation to the emergency department. Six of the children had upper limb pseudoparalysis and the rest lower limb symptoms. Age and sex data are given in Table 1. The mean age of children was six years and three months. Of the 100 children who underwent MRI, 63 were under the age of seven years and so required general anaesthetic during their MRI. This was performed by specialist paediatric anaesthetists and there were no complications from any of the anaesthetics.
Age and sex data for the 100 children in the study
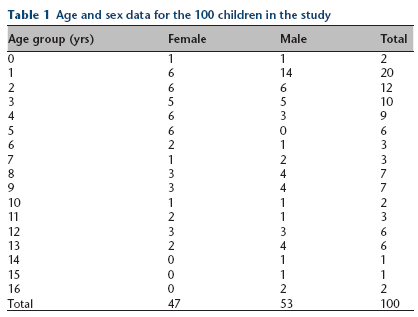
The most common stage of development for a child to present with a limp or limb pseudoparalysis were children of one, two, three or four years old (Table 1). Despite the high number in those aged 12 to 24 months (20% of the entire sample), only 2% of children aged between the age of 0 and 12 months of age were brought to the emergency department by their parents with limb disuse/pseudoparalysis. There was no statistical difference between the genders in the risk of developing a limp (47 female, 53 male). However, females were statistically more likely to have pathology identified on their scan than males (Pearson chi-squared(1) = 4.8307, Pr = 0.028). For example, juvenile idiopathic arthritis was three times more common in female patients (n = 6) than in male patients (n = 2).
During the study period two children with initially normal ESR and CRP deteriorated, rather than spontaneously getting better. When they were reviewed in clinic one week later they had repeat blood tests and were found to have raised inflammatory markers, and so underwent MRI at that stage, with both having positive scans for lower limb osteomyelitis. Both presented to the emergency department the same day their limp started, so it is likely that the blood tests failed to pick up their pathology at that stage as they were very early on in their disease process. This small number highlights that the vast majority of limping children with normal ESR and CRP will resolve without treatment, but that it is sensible to review all such limping children in clinic to pick up those with a serious disease who just presented very early in their disease course.
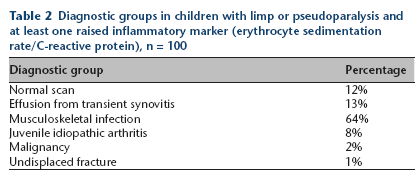
Of the 100 children in the study, 75 had changes on their MRI scan that either gave the diagnosis or contributed significantly to making the diagnosis. The largest group of conditions with abnormal scans was that of musculoskeletal infection, with 64 children being found to have osteomyelitis, septic arthritis, pyomyositis, fasciitis, abscess or discitis (Figs 1 to 3). Rheumatological causes for a joint effusion (such as juvenile idiopathic arthritis) were present in eight children (Fig. 4). Cancer was present in two individuals (one sarcoma and one leukaemia) and one child had linear bone oedema on MRI suggestive of an undisplaced fracture that was not visible on plain films (Tables 2 and 3).
Diagnostic groups in children with limp or pseudoparalysis and at least one raised inflammatory marker (erythrocyte sedimentation rate/C-reactive protein), n = 100
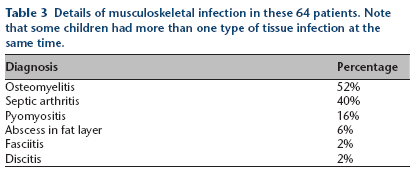
Details of musculoskeletal infection in these 64 patients. Note that some children had more than one type of tissue infection at the same time.

Tibial osteomyelitis, in child aged one year. Sagittal T2 weighted MR image with fat saturation. At presentation C-reactive protein < 10 mg/L, erythrocyte sedimentation rate 14 mm/hr. Arrow highlights bone oedema and periosteal oedema.
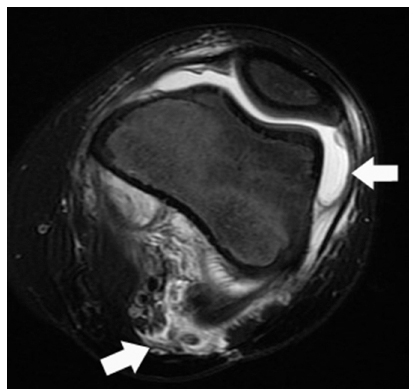
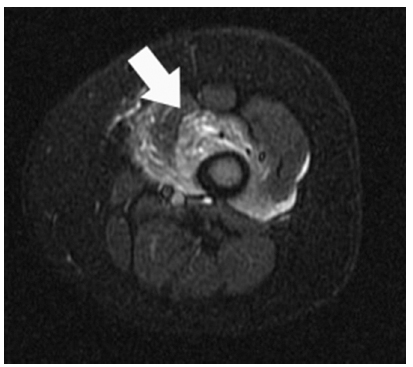
Septic arthritis of knee and pyomyositis in posterior thigh muscles, in child aged nine years. Axial T2 weighted MR image with fat saturation. At presentation C-reactive protein < 10 mg/L, erythrocyte sedimentation rate 27 mm/hr. Arrows highlight joint effusion and posterior muscle oedema.
Pyomyositis of quadriceps muscle, in child aged one year. Axial STIR MR image. At presentation C-reactive protein < 10 mg/L, erythrocyte sedimentation rate 35 mm/hr. Arrow highlights muscle oedema.
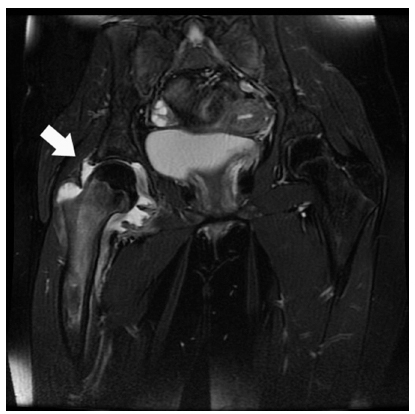
Right hip effusion with florid synovitis found to be juvenile idiopathic arthritis, in child aged 11 years. Coronal T2 weighted MR image with fat saturation. At presentation, C-reactive protein < 10 mg/L, erythrocyte sedimentation rate 25 mm/hr.
Of those who were found to have pathology on their MRI scan, 11 (15%) had previously seen a doctor elsewhere for the same problem. While they had been examined by that doctor, they had not undergone a MRI scan, were told they did not have a serious condition and had been allowed home with analgesia, later presenting to our hospital as they had failed to get better.
In all, 25 children were found not to have serious pathology causing their limp, and their symptoms resolved spontaneously over the following two or three weeks. Of these, a joint effusion secondary to transient synovitis was identified in 13 individuals, while a further 12 had normal scans and are presumed to have limped due to swollen lymph glands or muscle aches secondary to a more generalized infective illness that had caused their inflammatory markers to rise. The mean age of children with raised inflammatory markers and a diagnosis of transient synovitis was 3.9 years, compared with a mean age of 4.9 years in those with septic arthritis.
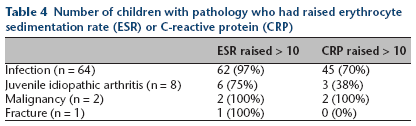
The use of ESR and CRP was compared to determine if just one blood test was effective in detecting cases of pathology, or if both were necessary. In those cases of musculoskeletal infection (n = 64), 62 (97%) had raised ESR while 45 (70%) had raised CRP. In cases of juvenile idiopathic arthritis (n = 8), six (75%) had raised ESR while three (38%) had raised CRP (Table 4).
Number of children with pathology who had raised erythrocyte sedimentation rate (ESR) or C-reactive protein (CRP)
Logistical regression models demonstrate that the higher the value of the CRP, the higher the likelihood of a positive MRI scan (Prob > chi-squared = 0.0090). However, once the ESR was raised above 10, increasing values further did not statistically increase the likelihood of a positive diagnosis on MRI (Prob > chi-squared = 0.1595). This would suggest that any rise in ESR is important, rather than the degree to which the value had risen. Table 5 shows the minimum, mean and maximum ESR and CRP levels per class of diagnosis.
Minimum, mean and maximum erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels per class of diagnosis

Mean values for CRP calculated assuming CRP < 10 is equal to zero.
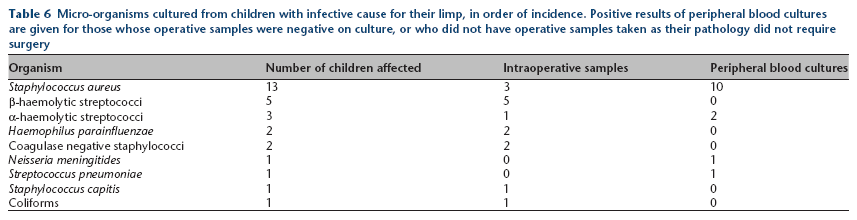
Table 6 gives details of the micro-organisms cultured from children with infective cause for their limp. It should be noted that the purpose of this study was not to investigate the microbiology of limping children, but to assess the potential for ESR, CRP and MRI in diagnosis. While all children had at least one peripheral blood culture taken, not all children with infection had positive culture from their blood cultures, and the study design did not include routine DNA analysis for organisms that do grow well on standard culture media (e.g. Kingella kingae). All those with a joint effusion (n = 38) had operative samples sent for microbiology, but children with other infections such as osteomyelitis, pyomyositis, fasciitis or cellulitis only had peripheral blood cultures taken. We have just included results for which a true infection is suspected, even if by an organism that is often regarded as a commensal bacterium. For example, the positive case of Staphylococcus capitis was cultured from more than one sample taken intraoperatively from septic arthritis of the hip in a one-year-old girl. This indicates that this normally commensal organism was more than likely pathogenic in that set of circumstances. Similarly, only Staphylococcus epidermidis isolated from operative samples from septic arthritis were included, since when cultured from peripheral blood samples it may indicate a skin contaminant.
Micro-organisms cultured from children with infective cause for their limp, in order of incidence. Positive results of peripheral blood cultures are given for those whose operative samples were negative on culture, or who did not have operative samples taken as their pathology did not require surgery
Discussion
This study of the causes of a limp or limb pseudoparalysis in children with raised inflammatory markers has shown interesting variation with increasing age. Only 2% of children in the study were aged 0 to 12 months, while 20% of children were aged 12 to 24 months. This may indicate a genuine difference in the incidence of pathology in the youngest of children (perhaps due to vertically acquired immunity from maternal antibodies) or just that a walking child who limps may be spotted by their parents more easily than a non-mobile baby with limb pseudoparalysis. It seems the most common stage of development for a child to be brought to the emergency department with a limp is when they are aged one, two, three or four years old, as 51% of children in the study were from this four-year age band. Older children of all ages presented with a limp, but much less frequently.
The aim of this study was to investigate whether testing for raised ESR or CRP in children with a limp or pseudoparalysis was an effective tool to identify those in need of further investigation and treatment. We then used MRI as the benchmark tool for detecting pathology and refined our diagnoses further with laboratory analysis of samples taken in the operating theatre. We have found that 75% of children with raised ESR or CRP had abnormalities on their MRI scan that either gave the diagnosis, or significantly contributed to the diagnosis. This would suggest that using this approach is an effective, targeted use of MRI resources. The fact that many did not have very high ESR or CRP may indicate that we are picking such cases up early in the disease course, which we would expect to be of benefit to the patients. Those detected without a very high ESR or CRP may also indicate that we are detecting infections by less aggressive bacterial organisms such as Kingella kingae that might otherwise be missed, 15 but still have the potential to cause long-term complications such as growth disturbance. Our findings suggest that a raised ESR or CRP should be an indication for admission of a limping child from the emergency department.
Past research has given rather mixed messages about the potential role of ESR and CRP in children with musculoskeletal infections. Much of this research has used these blood tests to develop algorithms that try to differentiate transient synovitis from septic arthritis. The fact that CRP may change faster than ESR in paediatric infections means that some have suggested CRP to be the inflammatory marker of choice when assessing for such infections.16,17 Others have concluded that ESR and CRP are very similar in their ability to detect bone and joint infections, and that it is best to perform both tests together.18,19 Work on septic arthritis undertaken in the United States has argued that only when an ESR is over 40 mm/hr should this raise concern. 7 Others have argued that these algorithms for identifying septic arthritis do not work quite as well in practice as initially hoped.20,21 Our study has found that certain causes for a limp, particularly osteomyelitis, may be present when the CRP is < 10 and the ESR is in the range of 11 mm/hr to 20 mm/hr. We had several young children with CRP < 10 and an ESR of 14 or 16, whose MRI demonstrated osteomyelitis (e.g. Fig. 1). This means that any value > 10 mg/L for CRP, or 10 mm/hr for ESR is worthy of further investigation in a limping child. Our results also show that failure to take an ESR will lead to clinicians missing a significant proportion of cases of conditions such as osteomyelitis or juvenile idiopathic arthritis. In consequence, we would strongly argue that both CRP and ESR are required for a robust assessment of the limping child.
Prior to this study we sometimes found it difficult to identify the location of pathology in those children who were too young to localize their symptoms well, despite a thorough history and careful examination. While the most common locations of pathology were the hip and knee joints and femur and tibia, pathology causing a limp did range in location from the spine to the metatarsals. In order to minimize the need for repeated MRI scans of different areas, we developed a method to screen for pathology in the lower limbs using coronal T1 and STIR images, which we term ‘the legogram’. This includes the entire pelvis and both limbs down to the ankles, and is possible in young children due to their limited size. High signal areas (appearing white) on the STIR images are easily picked up visually and allowed more focused imaging in axial and coronal planes as required. While this does not cover the forefoot or spine, it has improved our detection of pathology on the initial MRI scan and reduced our need for a second scan of different areas of the body a few days later, if the initial scan was normal but the patient failed to get better.
Children under the age of seven years may not lie still on the MR scanner for long enough for clear images to be obtained. When under six months of age, a feed and wrap strategy frequently allows the scan to take place while the baby sleeps. Older children aged five or six years may have a successful scan following the input of a play specialist and sedation. However, those children who move in the scanner required general anaesthetic to ensure clear images are obtained. 22 General anaesthetic is regarded as a safe intervention in those over three years of age, when performed by a paediatric anaesthetist. There is a possibility that general anaesthetic in children under the age of three years may be associated with a slight risk of neurodevelopmental disorders when older. 23 However, it is unclear whether this is a true association, and unknown whether such an association may be causative. For example, young children who already have a neurodevelopmental disorder may be more likely to require an MRI scan than would a healthy child, so in those cases while there would be an association, the scan would not be the cause of the neurodevelopmental disorder. This possible anaesthetic risk in young children should be weighed up by the clinician against the known potential risk of disability from missing a musculoskeletal infection or malignancy at an early stage when it would be easier to treat. We would argue that early detection of disease is likely to provide greater benefit than the potential risk from general anaesthetic in that age group.
We would anticipate that were this study to be repeated in different regions of the world, different proportions of pathology would be detected. Where an organism was identified, our infections were typically caused by Staphylococcus spp. and Streptococcus spp., or occasionally coliforms, Haemophilus sp. or Neisseria sp. (Table 6). We had no cases of tuberculosis in our study, and we are not a high-risk area for tick born infectious diseases. We also have fairly benign bacterial organisms with no cases of methicillin-resistant Staphylococcus aureus (MRSA) or Panton Valentine Leukocidin (PVL) secreting organisms in these children. Areas where MRSA and PVL are common may expect to find higher ESR and CRP at presentation in children with musculoskeletal infections.24,25 The attitudes of parents to the health of their children may vary between regions or countries so that a limping child may be brought for assessment early in one region but only later in the disease course in another region.26–28 Similarly, doctors in different countries may have different thresholds for how bad a limp needs to be before further investigation is warranted. These variations may well affect the blood results at presentation and again lead to different data regarding the sensitivity of ESR compared with CRP. Varying threshold in the degree of limp may also lead to differences in the proportion of children found to have pathology on their MRI. We only included children whom we regarded as having a distinct limp, but if children with a mild limp were scanned then the pick-up rate for pathology may be lower. In consequence, we are not arguing that 64% of limping children with raised inflammatory markers will always have a musculoskeletal infection or that 8% will always have a rheumatological arthritis. However, we do argue that a large proportion of children with a distinct limp and who have raised ESR or CRP are likely to have a significant pathology that would benefit from early diagnosis and treatment. For this reason, we would recommend that this screening approach to evaluating the limping child is applied by all those who have the necessary laboratory and MRI facilities to do so.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
None declared.