
Abstract
Abstract
Introduction
Displaced fractures of the lateral condyle of the humerus are usually treated with open reduction and fixation with smooth Kirschner wires. These may be passed through the skin and left exposed or buried subcutaneously. Exposed wires may be removed in the outpatient clinic, whereas buried wires require a formal procedure under anaesthesia. This advantage may be offset if there is a higher rate of complications with exposed wires. The aim of this study was to compare the safety and efficacy of exposed and buried wires.
Study design
Retrospective cohort.
Methods and materials
Children with lateral condyle fractures of the humerus who had undergone surgery were identified from our departmental database. Case records and X-rays of 75 patients were reviewed.
Results
Forty-two patients had buried wires and 33 had exposed wires. There were no serious complications in either group. In the exposed wires group, 1 patient had a superficial wound infection that was treated effectively with 1 week of oral antibiotics, while 2 patients had hypergranulation of pin tracts treated with topical silver nitrate. None of the patients showed loss of reduction, deep infection, or any other complications requiring additional procedures.
Discussion/conclusions
There was no statistically significant difference in the rate of complications between the buried and exposed groups. We conclude that open reduction and exposed wiring is a safe and effective option for lateral condyle fractures, and recommend a period of 4 weeks of K-wire fixation followed by 2 weeks of backslab immobilisation as adequate for union with minimal risk of infection.
Introduction
Fractures of the lateral humeral condyle are a common childhood injury typically caused by a fall onto an extended arm with a varus force [1]. Undisplaced fractures may be treated conservatively with casting, but displaced fractures have a high incidence of nonunion, and fractures with more than 2 mm of displacement require operative fixation [2–5]. Different methods of fixation have been described [6–10]; the most widely utilised method is open reduction and fixation with smooth Kirschner (K) wires [2, 4, 11]. K-wires may be buried beneath the skin or inserted through the skin with the wire ends exposed [12–15].
Buried K-wires require a second operation to remove the wires, while exposed wires may be removed in an outpatient setting. Thus, exposed wires offer logistical and cost advantages over buried wires. This advantage may be offset, however, if there is a higher rate of complications with the technique. Specific concerns are the risk of infection and adequacy of fixation [12].
By their very nature, exposed wires provide a potential portal for infection into the skin and deeper structures. Superficial infections may be treated with a short course of oral antibiotics, but deep infections (septic arthritis/osteomyelitis) may require surgical debridement and a prolonged course of intravenous antibiotics. Reducing the time to removal of exposed K-wires may reduce the risk of infection, but a short duration of fixation may not provide adequate time for secure union to occur [16]. In contrast, buried wires do not provide an entry point for infection, and wires may be left in situ for extended periods until union can be clearly demonstrated radiographically.
The preferred treatment for displaced lateral condyle fractures at our institution prior to 2005 was open reduction with buried K-wires. Since 2005, two of our consultant orthopaedic surgeons have been performing open reduction and fixation with exposed wires. Data in the literature specifically comparing exposed versus buried wiring after open reduction of lateral condyle fractures are scarce [12]. Our present study aims to compare the safety and efficacy of these two methods.
Methods
Study design
Retrospective cohort study.
Study population
Children who had undergone primary surgery for lateral condyle fractures of the humerus were reviewed retrospectively.
Inclusion criteria were children below age 16 with a lateral humeral condyle fracture treated with open reduction and fixation with K-wires. Patients had a minimum of 6 months from the time of injury to start of the study. Patients with other ipsilateral upper limb fractures, pathological fractures, or open fractures, as well as cases delayed for more than 14 days from injury were excluded.
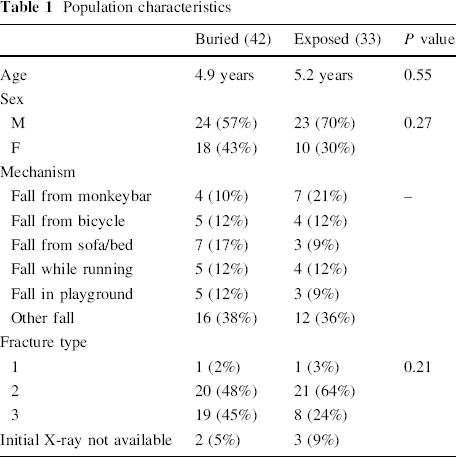
Demographic data, side of the fracture, displacement, and mechanism of injury were recorded. Fractures were classified according to a system modified from Jakob et al. [1]. Type 1 fractures were displaced by less than 2 mm, type 2 were displaced by more than 2 mm, and type 3 were displaced with rotation of the fragment.
Operative details recorded the insertion technique (buried or exposed), the number of wires used, and the angle of divergence for the wires. Baumann's angle and the presence of the intersection of the anterior humeral line (AHL) through the middle third of the capitellum on lateral view were recorded on postoperative X-rays.
Length of time that the wires were left in situ, radiographic union time, follow-up time, and subsequent complications were recorded.
Statistical analysis was performed with SPSS 17 for Windows (SPSS Inc., Chicago, IL, USA). Categorical data were compared with Pearson's chi-square test. Continuous data were compared with the Mann–Whitney test for nonparametric data and the independent t test for parametric data. Statistical significance was defined as P < 0.05.
Treatment
Buried wiring was fitted by various orthopaedic consultants and registrars (under consultant supervision) from our department. Exposed wiring was fitted by one of two consultant paediatric orthopaedic surgeons. The two surgeons who used exposed wires did so almost exclusively. Image-intensified X-ray guidance was used in all cases. Open reduction was performed by a lateral or posterolateral approach. The fracture was reduced with clamps. For cases treated with exposed wires, wires were pushed through the skin without opening additional skin incisions and drilled into the bone. Buried wires were inserted through the surgical wound and bent and buried beneath the skin. Postoperatively, all patients were immobilised in an above elbow backslab. All patients were seen at 1 week for X-rays, wound inspection, and for a change to a full cast. Patients with exposed wires were generally seen at 4 weeks postoperation for X-rays and wire removal; a removable backslab was applied for a further 2 weeks. Patients with buried wires were immobilised for 5 weeks (1 week of backslab followed by 4 weeks of full cast); subsequent immobilisation with a removable backslab for 2 weeks was employed at the discretion of the treating surgeon.
Results
Eighty-four patients had undergone open reduction and internal fixation of the lateral condyle of the humerus from 1st Jan 2005 to 31st Jan 2009. Nine patients were excluded according to our criteria. Seventy-five patients were included in our analysis. Forty-two patients underwent open reduction with buried wires, and 33 had exposed wires.
The characteristics of this population are shown in Table 1. Mean age was 5.0 years. There were 47 boys and 28 girls.
Population characteristics
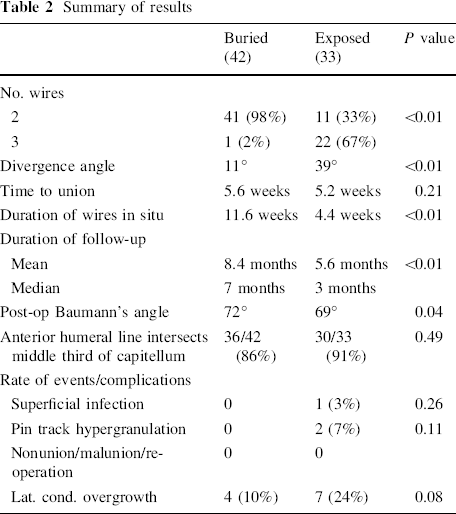
The results are summarised in Table 2. Patients with buried wires were usually fixed with 2 wires, whereas patients in the exposed group had 2 or 3 wires, with a larger divergence angle. Radiological union times were similar. There was a small postoperative difference in Baumann's angle that just reached statistical significance (P = 0.04). Rates of anterior humeral line intersection were similar. Buried wires were left in situ for more than twice as long as exposed wires. Length of follow-up was also significantly longer in the buried group.
Summary of results
Complications
There were no cases of nonunion, fracture displacement, or deep infection in our series. No patients required further surgery other than for the removal of buried K-wires.
In the patients with exposed wires, 2 patients developed hypergranulation of the pin tracts treated with topical silver nitrate. One patient developed a superficial pin tract infection that was effectively treated with 1 week of oral antibiotics. No cases of infection were noted in patients with buried wires.
A slightly higher incidence of lateral condylar overgrowth was noted in the exposed wire group.
Discussion
Advantages of exposed wires
We have found that leaving wires exposed for the fixation of lateral condyle fractures has logistical and cost advantages over buried wiring. The patient requires only one general anaesthetic for fixation, and the second procedure (removal) can be quickly and easily performed in the clinic. A simple cost analysis at our institution indicates a saving of S$1,100–1,500 (US$800–1,100) per patient (derived from day surgery and additional outpatient charges) with exposed wires before other, less tangible, benefits are considered (fewer hospital visits, resulting in savings from transport costs; less time off work/school; reduced patient/parental anxiety associated with a second operation, etc.). These advantages of exposed wires may be offset, however, if the clinical outcome is inferior to buried wiring.
Fixation technique
Beyond the use of buried or exposed wires, there were differences in surgical technique between the two groups. In particular, exposed wire patients were often fixed with three widely divergent K-wires, whereas patients with buried wires had only two wires and a much narrower divergence angle. The reason for these differences was concern about the adequacy of fixation of exposed wires. Buried wires are bent close to the bone, and the bend in the wire prevents the fracture fragment sliding along the wire and displacing. Exposed wires do not have a bend close to the bone, so a wider divergence angle and an additional wire was often deemed necessary to provide adequate stability. As we did not have any problems with loss of reduction or malunion, we believe that these measures are adequate for stable fixation.
Complications
The outcomes of both groups were good, with no serious complications. The one case of pin tract infection (3%) in the exposed group was effectively treated with a short course of oral antibiotics, and the two cases of hypergranulation (7%) of pin tracts responded to topical silver nitrate. This low rate of infection contrasts with the results of Launay et al. [12], who found a 28.1% infection rate with exposed wires, compared to 8% in patients with subcutaneous wires. The reason for this is unclear, but may reflect a lower threshold for diagnosing infection, differences in surgical technique, differences in perioperative antibiotic protocols, or a difference in the time to K-wire removal. Regarding surgical technique, for exposed wires we preferred to pierce the skin directly rather than to make skin incisions for insertion. Drilling through the skin may result in skin damage and necrosis and increase the risk of infection; it is prudent take steps to minimise skin damage, such as reducing drill speed and avoiding multiple passes. Patients in this series received intravenous antibiotics intraoperatively and for 24 h postoperatively, and exposed wires were removed at an average of 4.4 weeks (5.9 weeks for Launay et al.), with 2 weeks of further immobilisation with a backslab. Buried wires were left in situ until fracture healing was clearly visible on radiographs. In this series, the average time to removal of buried wires was 11 weeks. The shorter period of internal fixation did not result in any cases of late displacement or requirement for re-operation.
Time to radiographic union
Times to radiographic union were comparable, with a slightly longer time to union in the buried group that was not statistically significant.
A concern regarding exposed wires is that in cases of radiographic delayed union, it may be desirable to leave wires in for more than 4 weeks. Notably, the average time to radiological union in the exposed group (5.2 weeks) was longer than the time to removal of wires (4.4 weeks); i.e., wires were removed at 4 weeks regardless of the presence or absence of radiological bridging callus. In the patients where radiographic union was not evident at 4 weeks, the removal of wires at this juncture did not result in any problems, suggesting that radiological evidence of callus is not required before the removal of wires. In the literature, there is some controversy regarding the timing of the removal of wires and the importance of radiological union as a criterion for implant removal [16–18]; we have found a protocol involving removal at 4 weeks with 2 weeks of subsequent immobilisation in a backslab to be safe and effective, regardless of radiological evidence of callus.
Lateral condyle overgrowth
Overgrowth of the lateral condyle has been noted by some authors [12, 19]; however, this is rarely symptomatic, and is usually not regarded as a true complication. In this series, the finding was purely radiological, with none of the patients reporting clinically apparent lateral overgrowth.
Limitations
This study was retrospective and, as mentioned above, the groups differed in terms of the divergence angle and the number of wires used.
Follow-up in this series was short, with many patients not returning for late follow-up. This was particularly evident in the exposed wire group. Patients in this group may not feel the need to return for follow-up once implants are removed at 4 weeks, whereas patients in the buried wire group tend to remain on follow-up until after the removal of their wires. While this lack of late follow-up limits the ability to detect long-term problems (e.g., growth arrest, stiffness, cubitus valgus), it is likely to represent a good outcome with a low incidence of clinically significant problems.
Intrinsically, this study was not designed to detect more subtle differences in outcome, such as postoperative range of movement, carrying angle, etc.
Conclusions
This study shows good outcomes for both exposed and buried methods of wiring lateral condyle fractures. Leaving wires exposed following the open reduction of lateral condyle fractures is a safe and effective alternative to burying wires, and obviates the need for a second operation for removal. Concerns regarding the stability of fixation with exposed wires may be adequately addressed with widely divergent wires and the use of a third K-wire as necessary. A four-week period of K-wire fixation followed by 2 weeks of backslab immobilisation is adequate for fracture union with minimal risk of complications.