
Abstract
Purpose:
The objective of this study was to evaluate the outcomes of various methods of fixation for pediatric lateral condyle fractures. The null hypothesis was that there would be no difference between the three treatment groups and time of return to the full range of motion.
Method:
There were three fixation groups—Algemeinshaft fur osteosynthesegragen (AO) cannulated screws (n = 11), buried Steinmann pins (n = 13), and unburied Steinmann pins (n = 36). Variables evaluated were time to return to full range of motion of the elbow, whether therapy was required, average number of follow-up visits, fracture classification (Milch), time to operating room, duration of immobilization, degree of initial fracture displacement, time to radiographic healing, complications, and if manipulation under anesthesia was done, whether this was planned or not.
Results:
Average return to full range of motion for Algemeinshaft fur osteosynthesegragen cannulated screw, buried Steinmann pins, and unburied Steinmann pins were 113, 82.7, and 94 days, respectively. A one-way ANOVA revealed a p-value of 0.11711. p-Values were also insignificant for the average number of follow-up visits, time to operating room, and time of immobilization. The p-value for time to radiographic healing was <0.00001, with times for Algemeinshaft fur osteosynthesegragen cannulated screw, buried Steinmann pins, and unburied Steinmann pins being 75, 35, and 34.9 days, respectively. Notably, the Algemeinshaft fur osteosynthesegragen screw group averaged 9 years old, more than twice the Steinmann pin groups’ 4 years.
Conclusion:
Data from this sample suggest that there is no difference in return to full range of motion when comparing the three fixation methods. There was a difference in time to radiographic healing with Algemeinshaft fur osteosynthesegragen screws taking the longest, potentially due to age differences.
Introduction
Lateral condyle fractures account for 12%–17% of all distal humerus fractures in the pediatric population. The most common complication following pediatric lateral condyle fracture is lateral condylar overgrowth; however, other possible complications include cubitus varus or valgus, fishtail deformity, osteonecrosis, neurological injuries, physeal arrest, and malunion.1 A 10-year retrospective study found that surgical intervention was required in approximately 36.2% of cases of lateral condyle fractures of the humerus. 2 Fractures are categorized as non-displaced or displaced, and, if displaced, furthermore stable or unstable. Lateral condyle fractures with less than 2 mm of displacement are generally deemed stable and treated conservatively. Fractures with greater than 2 mm of displacement are potentially unstable and may require operative intervention. Fractures with greater than 4 mm of displacement usually require open reduction and internal fixation.
Fractures with minimal displacement and intact articular hinges can be treated with closed reduction and percutaneous pinning. Unstable and displaced fractures require open reduction internal fixation (ORIF) using either Steinmann pins/Kirschner wires or Algemeinshaft fur osteosynthesegragen (AO) cannulated screws. Steinmann pins can be either buried or unburied (percutaneous). 1 Percutaneous implants are cheaper, easier to implant, and can be removed in a clinic without the need for anesthesia. However, according to a study by Li and Xu, compared to AO cannulated screws are associated with higher rates of infections, lateral prominence, nonunion requiring further surgical intervention, and require prolonged immobilization resulting in elbow stiffness. Buried AO screws require return to operating room to remove, and have higher risks of avascular necrosis as well as potentially damaging effects on the ossification nucleus of the capitellum. 3 However, AO screws allow for more stable fixation, higher chances of union, and opportunity for earlier ROM. Buried pins require removal in the operating room but offer an opportunity for manipulation of the elbow under anesthesia.4,5 One of the most commonly reported concerns following ORIF is decreased ROM, with data showing there is a delay in achieving elbow motion.5,6 Another study demonstrated similar union rates when lateral condyle fractures were treated with Steinmann pins compared to AO screws, but had a higher rate of infections and stiffness. This study compares the return of ROM between lateral condyle fractures treated with buried Steinmann pins, percutaneous pins, and AO screws. 7 To our knowledge, no studies compare the return of ROM with buried Steinmann pins, unburied Steinmann pins, and AO screws.
Methods
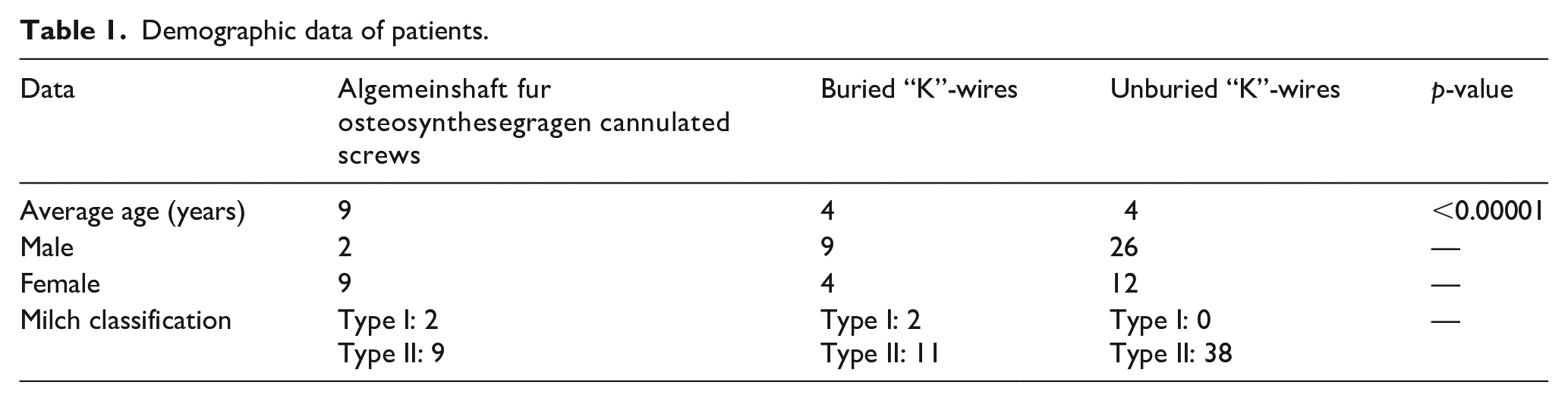
This was a single-center retrospective study for the last 8 years (2016–2024) of pediatric patients, <16 years of age, with isolated lateral condyle fracture of the distal end of the humerus that requires ORIF. Patients with polytrauma, closed reduction percutaneous pinning, subacute injuries (over 3 weeks), and associated neurologic injuries were excluded. Patients were divided into three groups based upon what type of ORIF was performed—AO cannulated screws, buried Steinmann pins, and unburied Steinmann pins. Data was recorded in REDCap with patients de-identified. Demographic data can be found in Table 1.
Demographic data of patients.
From chart review the following data was collected—time to return to full range of motion (FROM) of the elbow, whether therapy was required or not, average number of follow-up visits, fracture classification (Milch), time to operating room, time of immobilization, degree of initial fracture displacement, time to radiographic healing, complications, and if manipulation under anesthesia (MUA) was performed (unplanned or planned). Complications this study looked for included nonunion, malunion, infection, hardware complications, and unplanned return to the operating room. FROM was considered obtained in patients where FROM or a ROM from within 0 to 5 degrees extension to 130–140 degrees flexion was noted in their chart. For patients requiring MUA, time to radiographic healing was defined as the interval from surgery to the appointment immediately preceding MUA. For others, it was defined as the time from surgery to the clinic visit during which pin removal occurred, or when noted based on radiologic read in the chart.
The number of patients in the AO cannulated group and buried Steinmann pin who were scheduled for planned removal of hardware and MUA was recorded. The protocol for MUA is as follows. Prior to the removal of the pin, the elbow was manipulated. ROM is measured before and after MUA. Following the MUA, a small incision was made over the lateral aspect of the elbow, and the pins or screw were removed. Incisions were injected with local anesthetic, a soft dressing applied, and patients instructed on resuming regular ROM after surgery. For the other two groups, ROM was initiated at the time of cast removal.
Statistical analysis included a one-way ANOVA to assess if there was any statistically significant difference between the groups (p < 0.05). This was done with each variable collected in order to determine whether the groups were comparable in terms of patient age and fracture severity. Where the ANOVA revealed a p < 0.05, individual post-hoc Tukey tests were run between the three groups in order to determine which groups were significantly different.
Results
There were 62 patients who underwent ORIF for isolated displaced lateral condyle fractures. A chart review was conducted to collect the desired data. A summary of this data can be found in Table 2. The groups were not comparable in terms of age (p < 0.00001). Post-hoc Tukey test indicated differences between the AO cannulated screw and the buried pin groups, as well as the AO cannulated screw and the unburied pin groups—with the buried pin group as well as the unburied pin group patients being both significantly lower in age compared to the AO cannulated screw group patients. However, groups were comparable in terms of fracture severity (mostly Milch 2, and similar initial displacement), time to OR, number of follow-up visits, and time immobilized. In all patients, anatomic reduction was obtained, with no noted loss of reduction.
Data collected.
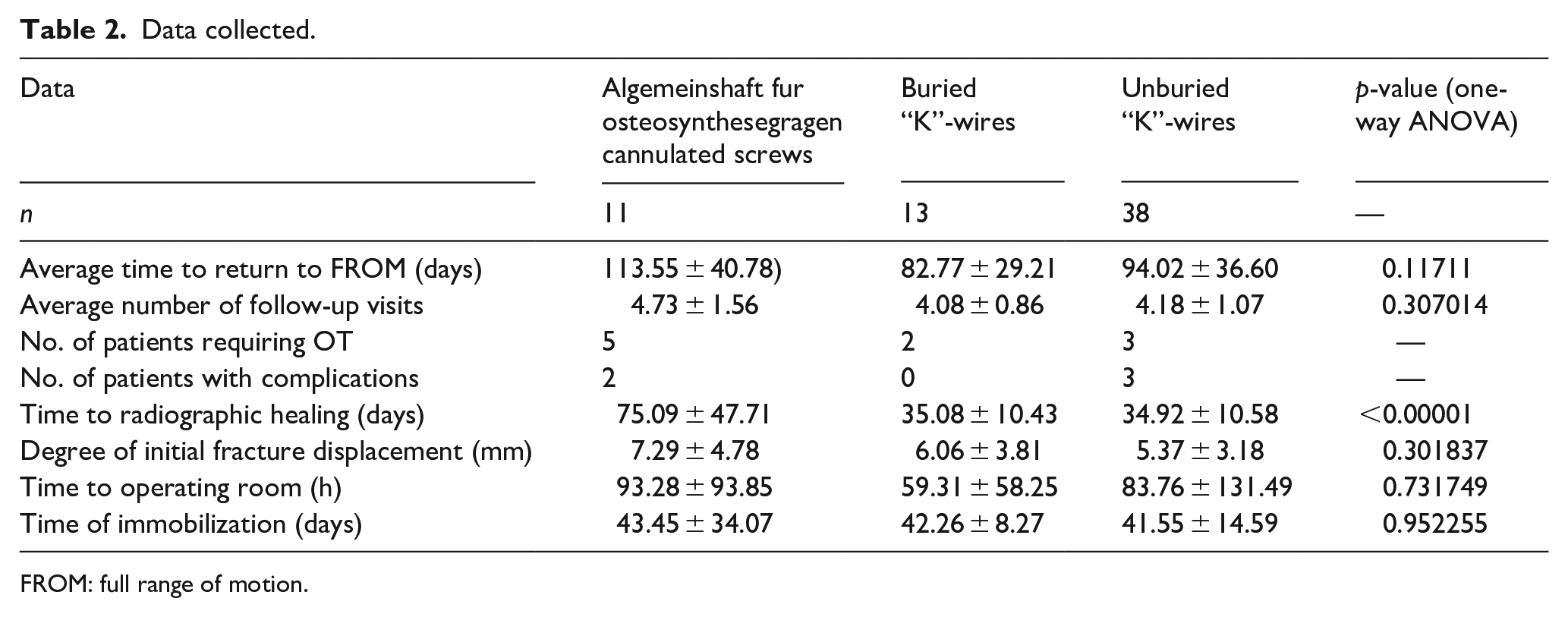
FROM: full range of motion.
Notably, average return to FROM for AO cannulated screw, buried Steinmann pins, and unburied Steinmann pins were 113, 82, and 94 days, respectively, with no statistically significant difference (p = 0.11711). However, for time to radiographic healing, the p-value was <0.00001, with times for AO cannulated screw, buried Steinmann pins, and unburied Steinmann pins being 75, 35, and 34 days, respectively. A post-hoc Tukey test revealed significant differences between the AO cannulated screw group and the buried pin group (p = 0.00002), as well as the AO cannulated screw group and the unburied pin group (p = 0.00002). The buried pin group, as well as the unburied pin group, both took significantly less time to obtain radiographic healing compared to the AO cannulated screw group. There were also complications noted in the AO cannulated screw group as well as the unburied pin group. In the AO cannulated screw group, there was one case of nonunion and one case in which an unplanned MUA was needed. In the unburied pin group, there was one case of malunion, one case of pin site infection requiring antibiotics, as well as one case of pin infiltration in which antibiotics were prescribed prophylactically. In the cases of malunion and nonunion independent radiographic review was also done.
Discussion
This study aimed to evaluate the outcomes of different fixation methods for lateral condyle fractures in pediatric patients, specifically comparing AO cannulated screws, buried Steinmann pins, and unburied Steinmann pins. The primary focus was on the time to FROM of the elbow, the necessity for OT, time to radiographic healing, and the incidence of complications.
The findings suggest that the method of fixation did not significantly impact the time to return to FROM. Although numerically the average time to FROM was longest in the AO cannulated group, shortest in the buried pin group, and intermediate in the unburied pin group, this difference did not reach statistical significance. The notable statistical difference in time to radiographic healing, with the AO cannulated screw group taking the longest compared to buried and unburied pins, could suggest that the choice of fixation may influence the duration of the overall recovery process, even if functional recovery of FROM occurs at similar time points. However, the statistically significant difference in the age groups—with the AO cannulated group being older than both the buried and unburied pin groups—cannot be disregarded, with younger age patients having greater potential to heal fractures faster. Other results worth discussing are the number of patients requiring therapy as well as the number of patients with complications. The AO cannulated screw groups had 5 of the 11 patients (45%) requiring therapy to help obtain FROM, with one needing an unplanned MUA, as well as one case of nonunion. This again may be related to the healing capability of older patients, but is worth noting. In the unburied pin group, there were three patients with reported complications, with two related to pin site infection and one malunion. The buried pin group had no complications, but the additional anesthesia event for MUA is not without risk.
Several limitations warrant consideration when interpreting these results. The study’s retrospective design introduces potential biases, and the relatively small sample sizes within each group, particularly the disproportionately large unburied pin group, limit the generalizability of our findings. In addition, the definition of FROM relied on clinician documentation of “FROM” or a range within a specified near-anatomic limit at the time of discharge from active follow-up. This introduces a degree of subjectivity as the endpoint was based on individual clinical assessment rather than standardized goniometric measurements. Lastly, patients who underwent screw fixation were chosen based on physician preference, not fracture severity or age of patient; however, this was not reflected in the results of this study. These are limitations faced as a retrospective study.
Larger, multicenter prospective studies are needed to confirm these results and further explore the long-term outcomes associated with each fixation method. Future research should match groups in terms of age and fracture severity and further consider other factors such as functional outcomes, fracture characterization, and patient-reported outcomes to provide a more comprehensive assessment of the advantages and disadvantages of each fixation method.
Conclusion
The data from this sample of patients suggests that there is no difference in time to return to FROM when comparing the AO screw fixation, buried Steinmann pins, and unburied Steinmann pins. However, there were differences in time to radiographic healing, OT requirements, and rates of complications, with AO cannulated screws having the longest time and most OT requirements. This may be due to significant age differences in the groups, with that of the AO screw group being just over twice that of both of the Steinmann pin groups. The unburied Steinmann pin group exhibited the highest overall complication rate, primarily related to pin site issues, but had the fastest time to radiographic healing—not to a significant difference. While buried Steinmann pins demonstrated the fastest return of FROM and fewest complications, the lack of statistical significance in FROM across all three groups suggests multiple factors contribute to functional recovery. Given the limitations of this study, future larger-scale studies with age-matched cohorts and standardized outcome measure are recommended to more definitively determine the differences in the three fixation methods (Figure 1).
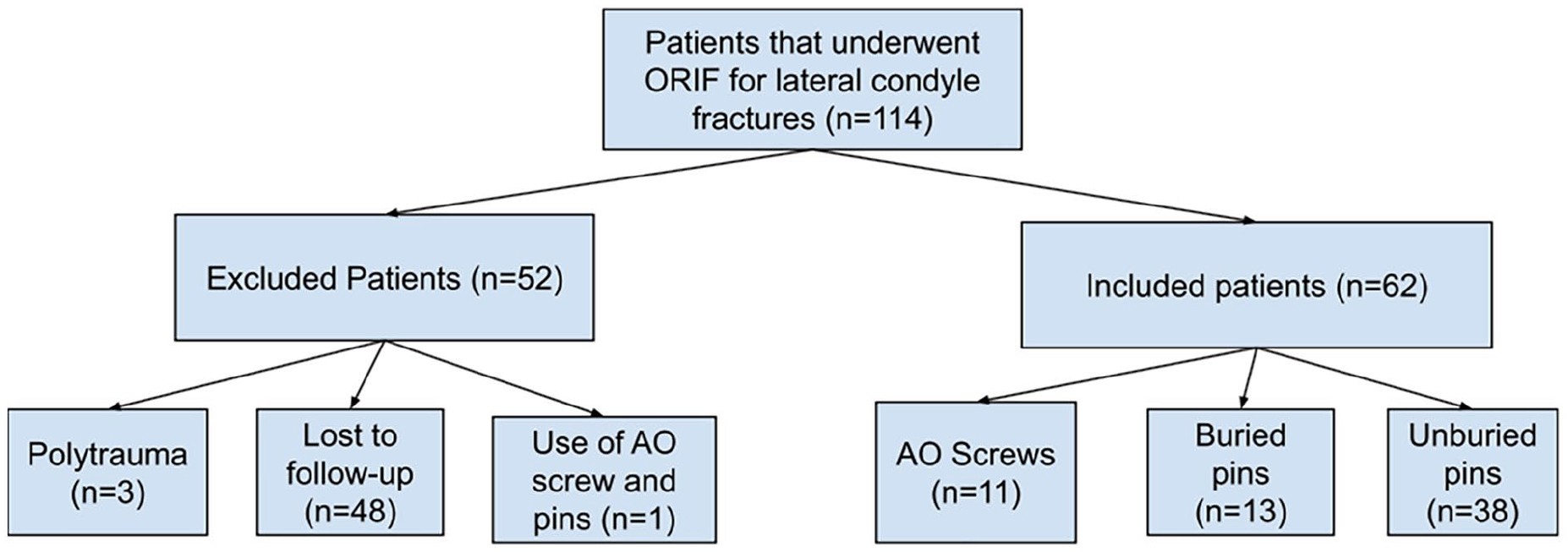
Flowchart of patients reviewed.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251368279 – Supplemental material for Assessment of postoperative range of motion in pediatric patients undergoing surgical reduction and fixation of lateral condyle fractures
Supplemental material, sj-pdf-1-cho-10.1177_18632521251368279 for Assessment of postoperative range of motion in pediatric patients undergoing surgical reduction and fixation of lateral condyle fractures by Gabrielle Rogie, Timothy Borden, Lindsay Crawford, Surya Mundluru, Brennan Roper, Rohini Mahajan Vanodia and Shiraz Younas in Journal of Children's Orthopaedics
Footnotes
Acknowledgements
The authors would like to thank Mason Chimenti for his contribution to the retrospective review to determine patient eligibility for the study.
Ethical considerations
The study was approved by the Ethics Committee of the University of Texas at Health Science Center at Houston IRB (no. HSC-MS-23-0110) in March 2023, with the need for written informed consent waived.
Author contributions
Gabrielle Rogie: Formal analysis, investigation.
Timothy Borden, Lindsay Crawford, Surya Mundluru, Brennan Roper: Resources, writing—review and editing.
Rohini Mahajan Vanodia: Project administration.
Shiraz Younas: Conceptualization, writing—review and editing, supervision.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.