
Abstract
Purpose:
Minimally displaced pediatric proximal humerus fractures can be reliably managed non-operatively; however, there is considerable debate regarding the appropriate management of severely displaced proximal humerus fractures, particularly in older children and adolescents with limited remodeling potential. The purpose of this study was to perform a systematic review to answer the questions: “What are the functional and quality-of-life outcomes of pediatric proximal humerus fractures?” and “What factors have been associated with a poorer outcome?”
Methods:
A review of Medline and Embase was performed on 4 July 2021 using search terms relevant to proximal humerus fractures, surgery, non-operative management, pediatrics, and outcomes. Studies including ≥10 pediatric patients with proximal humerus fractures, which assessed clinical outcomes by use of an established outcome measure, were selected. The following clinical information was collected: participant characteristics, treatment, complications, and outcomes.
Results:
Twelve articles were selected, including four prospective cohort studies and eight retrospective cohort studies. Favorable outcome scores were found for patients with minimally displaced fractures, and for children aged less than 10 years, irrespective of treatment methodology or grade of fracture displacement. Older age at injury and higher grade of fracture displacement were reported as risk factors for a poorer patient-reported outcome score.
Conclusion:
An excellent functional outcome can be expected following non-operative management for minimally displaced pediatric proximal humerus fractures. Prospective trials are required to establish a guideline for the management of severely displaced proximal humerus fractures in children and adolescents according to fracture displacement and the degree of skeletal maturity.
Level of evidence:
level V.
Purpose
Proximal humerus fractures (PHFs) comprise between 0.45% and 2% of all pediatric fractures,1–4 with an estimated incidence between 31.4 and 680/100,000 children per year and a 3:1 male preponderance.4,5 85% of pediatric PHFs are minimally displaced, Neer–Horowitz (NH) Grade I or Grade II fractures.2,6 It has been suggested that PHFs that occur prior to skeletal maturity rarely lead to a functional or cosmetic deficit. 7 These fractures have a profound ability to remodel, as the proximal humeral growth plate is responsible for 80% of humeral longitudinal growth.8–14 The glenohumeral joint has the widest range of motion of any joint in the body and can accommodate a large degree of deformity without causing significant functional impairment.8,15,16 Because of these unique attributes, pediatric PHFs have historically been treated non-operatively.3,17 This practice continues to be accepted for NH Grade I and Grade II fractures; however, there is considerable debate regarding the management of NH Grade III and Grade IV fractures, particularly in teenagers with relatively limited remodeling potential.2,4,9,13,18,19 Proposed treatment algorithms are based on patient age and grade of displacement;3,5,20 however, no generally accepted guideline has been established.2,21,22 The aim of this systematic review was to synthesize the current literature regarding the functional and quality-of-life outcomes of pediatric PHFs, and identify factors associated with a poor clinical outcome.
Methods
This study was carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, and is registered at the International Prospective Register of Systematic Reviews (PROSPERO). The published protocol for this review can be found on the PROSPERO website, registration no. CRD42021241929. 23
Eligibility criteria
Included articles were original research studies written in English and published in a scientific journal. The studies must have reported the clinical outcomes of pediatric patients treated for PHF, by use of an established outcome measure, such as the Constant–Murley Score (CMS), the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire, or American Shoulder and Elbow Surgeons score (ASES).24,25 Only studies with at least 10 subjects aged 18 years or younger at the time of injury. Studies that evaluated the efficacy of a novel surgical technique were excluded.
Search strategy
A librarian-assisted search was performed on Medline and Embase on 4 July 2021, from inception until the date of the search (see Supplementary Files 1 and 2). The search syntax consisted of six categories of keywords and/or subject headings intersected by the Boolean terms “AND” or “OR.” These categories were terms related to: (1) the proximal humerus; (2) fractures; (3) surgery; (4) non-operative management; (5) pediatrics; and (6) outcomes. The reference lists of studies selected for full-text review were reviewed, to ensure literature saturation. All citations were uploaded to Endnote 20®, where duplicates were removed. Relevant articles were read in full text by the two reviewers (S.A. and B.R.), and any discrepancies were resolved with discussion.
Data collection
Standardized extraction forms were developed with the use of the Covidence® tool for systematic literature reviews. The study data extracted included study type, year of publication, methodology, number of participants, participant characteristics, treatment, complications, and outcomes.
Data synthesis
Results of the individual studies were synthesized qualitatively, with consideration made for study design and potential biases.
Risk of bias within studies and quality assessment
The quality of the selected studies was assessed using the Coleman Methodology Score.26,27 The CMS allocates up to 100 points according to 10 criteria: study size, mean duration of follow-up, number of different surgical procedures discussed, the type study, diagnostic certainty, whether a description of the surgical procedure is given, whether outcome measures are clearly defined, methods of reporting outcomes, and description of the subject selection process. A study with a perfect CMS of 100 is largely devoid of the influences of chance, biases, and confounding factors. 20
Results
Study selection
The search retrieved 2450 results, 481 of which were duplicates. Of the 1969 individual articles screened, 1943 were excluded because of an irrelevant title or abstract. Therefore, 26 articles underwent full-text review. The initial agreement on articles selected for final inclusion was 68% (kappa = 0.429; moderate agreement). Fourteen were excluded on full-text review for the following reasons: involved adult subjects only,28–34 focused on surgical technique,35–38 conference presentation, 39 non-English language, 40 and did not evaluate outcomes using a validated instrument. 5 Twelve articles were ultimately deemed eligible for inclusion.6,9–11,13–15,21,41–44 This process is outlined in the PRISMA diagram (Figure 1).
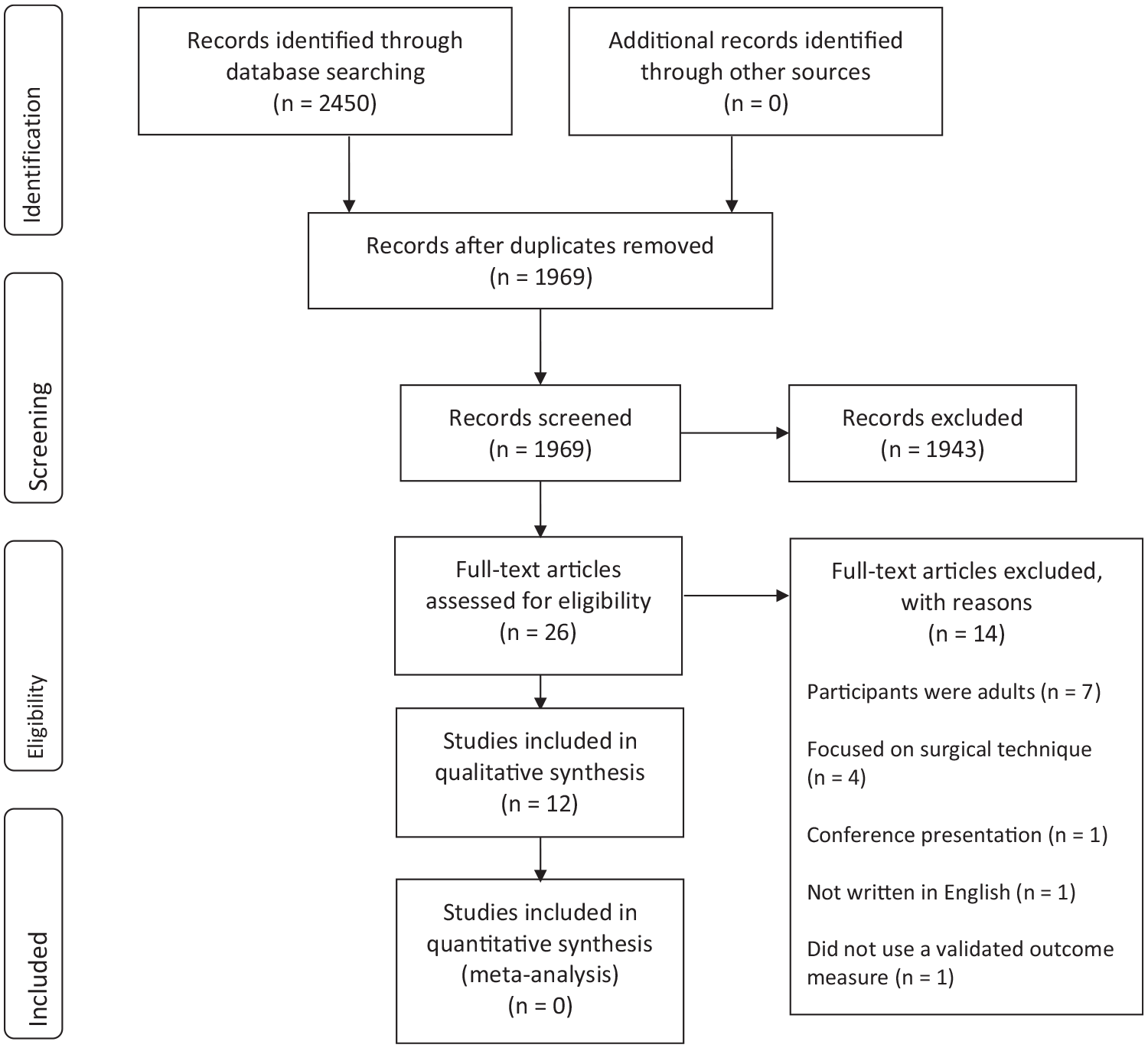
PRISMA flow diagram outlining the process by which articles were screened.
Study design
There were four prospective cohort studies and eight retrospective cohort studies, including a total of 791 subjects. The mean age was 10.8 years (standard deviation = 3.2, range = 1–18), and 56.5% were male. Six hundred eighty-five participants (86.6%) were followed-up for a median duration of 2 years (range = 2 weeks–18 years). Seven studies only included physeal fractures and graded fractures by use of the NH classification,6,11,13,14,21,41,44 while one study included only metaphyseal fractures and categorized fractures according to the degree of fracture angulation. 10 Four studies included both physeal and metaphyseal fractures; two classified fractures according to the AO system42,43—one categorized patients according to the degree of fracture angulation 15 and one used both the NH classification (for physeal fractures) and degree of angulation (for metaphyseal fractures). 9 Six of the eight studies that analyzed physeal fractures excluded participants with NH Grade I and Grade II fractures,6,9,14,21,41,44 while the other two included all grades.11,13 Six studies included only skeletally immature patients, as indicated by an open epiphyseal plate on plain radiographs.6,21,11,42–44 The functional outcome measures reported are shown in Table 1. These were as follows: CMS (six studies),6,10,11,13,14,41 QuickDASH (four studies),6,21,42,43 ASES (one study), 44 Neer Shoulder Score (NSS) (one study), 9 and the functional classification of Razemon and Baux (one study). 15 Pavone et al. 6 used the QuickDASH as well as the “Delta Constant,” namely, a comparison of the CMS of the affected shoulder with that of the contralateral shoulder, and Kraus et al. 14 used both the DASH and CMS.
Study design of the included articles.
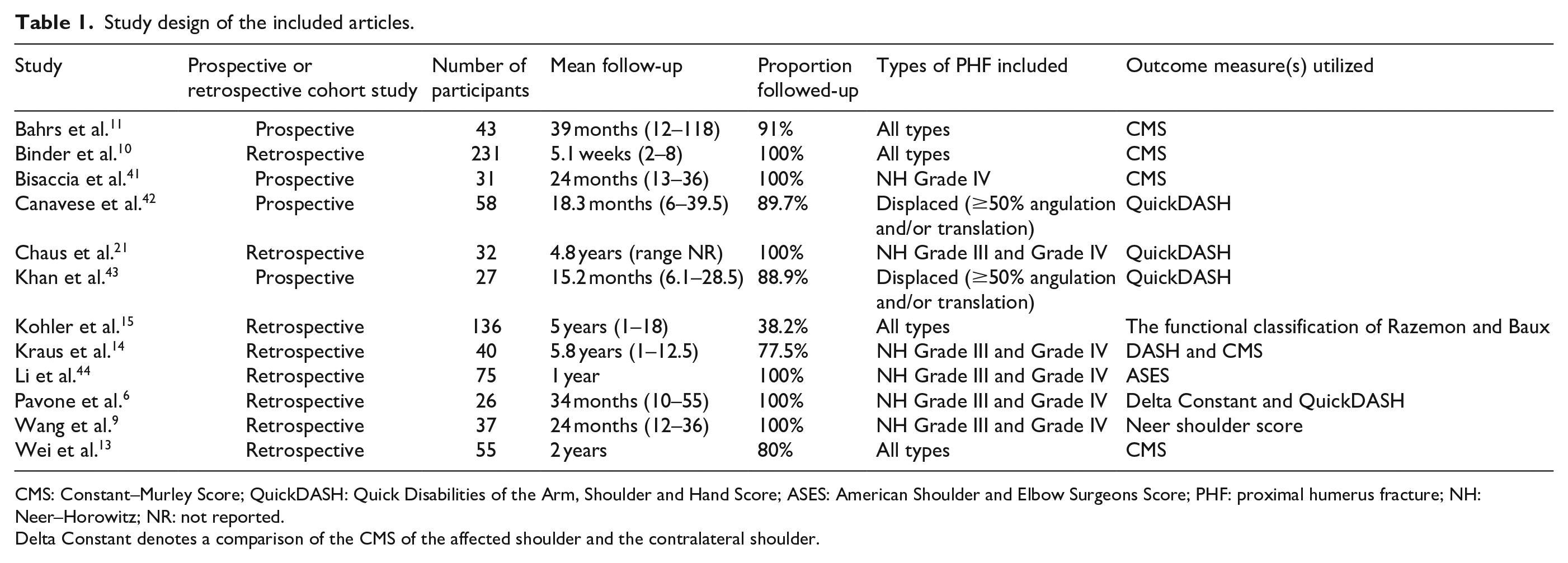
CMS: Constant–Murley Score; QuickDASH: Quick Disabilities of the Arm, Shoulder and Hand Score; ASES: American Shoulder and Elbow Surgeons Score; PHF: proximal humerus fracture; NH: Neer–Horowitz; NR: not reported.
Delta Constant denotes a comparison of the CMS of the affected shoulder and the contralateral shoulder.
Quality assessment
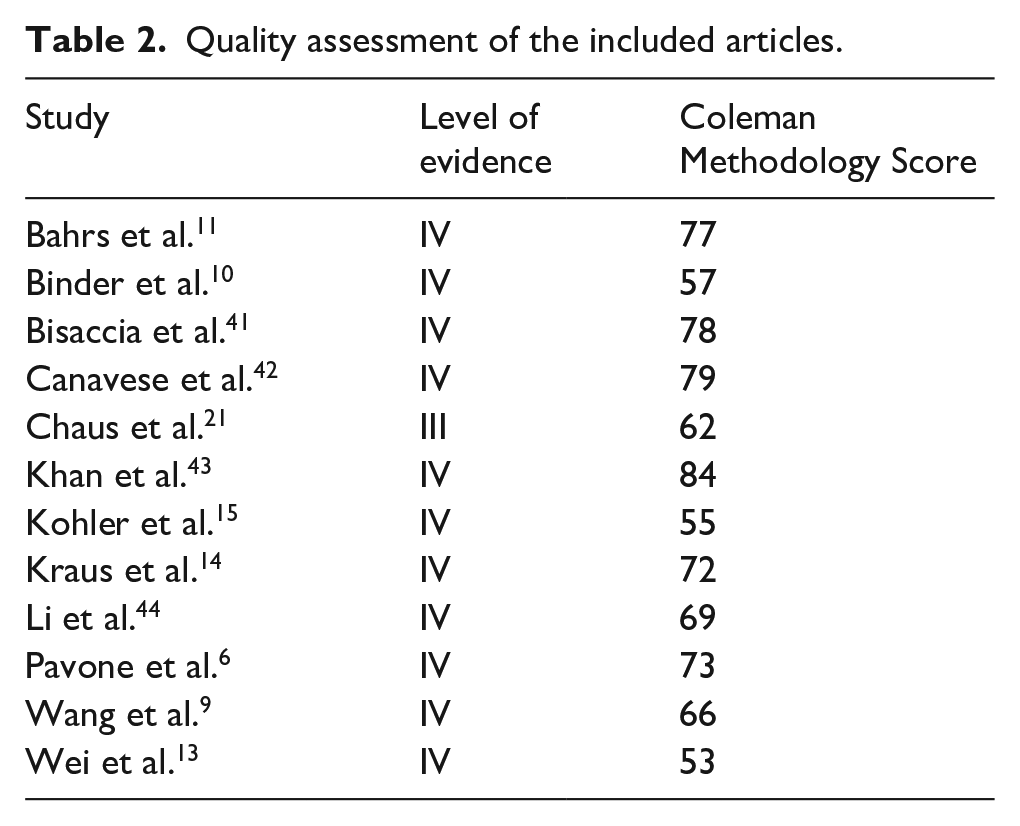
One study matched participants who underwent surgical versus non-operative management of their PHF. 21 All other studies were level IV case series, as according to the Oxford Centre for Evidence-Based Medicine. The mean Coleman Methodology Score was 68.8/100 (standard deviation = 10.2, range = 53–84; see Table 2).
Quality assessment of the included articles.
Functional outcomes
Studies including only physeal fractures
All participants in the study by Wei et al. 13 were managed conservatively for physeal PHFs of all grades of severity. A significantly higher number of cases in the <11-year-old group had an “excellent” rather than “good” CMS at 2-year follow-up compared with the ≥11-year-old group (p < 0.05). In Bisaccia et al.’s 41 study of NH Grade IV PHFs treated with an external fixator for 6 weeks, all patients had at least a very good functional outcome, with an average CMS at 6-month follow-up of 97.5. The patient with the lowest CMS (84) was 15 years old, while the lowest CMS for patients <11 years old was 94. Bahrs et al. 11 treated 43 participants either surgically or non-operatively according to NH grade and whether they were older or younger than 10 years. All patients with non-displaced fractures had a perfect CMS at final follow-up, and there was no statistically significant difference between the CMS of any groups of participants according to age, NH grade, or treatment modality. Participants treated non-operatively for NH Grade III and Grade IV fractures in the study by Chaus et al. 21 had a mean QuickDASH score that was 1.8 points higher (i.e. worse) than the surgical group; however, this difference was not statistically significant (p = 0.1723). With every 1-year increase in age at initial injury for patients treated non-operatively, the odds ratio of a less than desirable outcome increased by a factor of 3.81 (95% CI = 1.31–21.0). 21 Pavone et al. 6 similarly favored surgical management for NH Grade III and Grade IV PHFs in their cohort with a mean age of 12.8 years. The mean QuickDASH score at final follow-up was excellent (0.56; range = 0–1.7); however, the authors found significantly worse Delta Constant scores for participants with NH Grade IV rather than Grade III fractures (p < 0.01). 6 In a study with a similar cohort (mean age 11.3 years, treated surgically for severely displaced PHFs), Kraus et al. 14 found that patients had favorable outcomes, irrespective of whether they underwent K-wire fixation or ESIN (p = 0.26). Li et al. 44 found excellent functional results in adolescents treated for severely displaced PHFs with either K-wire fixation or external fixation, with a mean ASES of 93.6 or 93.7 at 6-month follow-up, respectively.
Study including only metaphyseal fractures
Binder et al. 10 reviewed the short-term functional outcomes of patients treated surgically versus non-operatively for metaphyseal PHFs after an average follow-up of 5 weeks. The authors found that all seven patients who were treated non-operatively for fractures with >20 degrees angulation had only an “average” outcome, whereas all patients treated non-operatively for fractures with <20 degrees had excellent outcomes. 10
Studies including both physeal and metaphyseal fractures
Khan et al. 43 found promising functional outcomes for children with displaced PHFs treated surgically with elastic stable intramedullary nailing (ESIN), in their study with a mean age of 11.2 years. The mean QuickDASH scores for patients with metaphyseal fractures were 1.8 compared to 2.7 for those with physeal fractures (p > 0.05), indicating a low level of impairment. Canavese et al. 42 also analyzed the outcomes of 58 patients with PHFs treated with ESIN by use of the QuickDASH. The mean QuickDASH score at final follow-up for patients with physeal fractures was 1.6, and for those with metaphyseal fractures was 1.0, although this difference was not statistically significant. The authors did not comment on any relationship between functional outcome and patient age. 42
All participants in the study by Kohler et al.15,45 had either good (n = 15) or very good (n = 37) functional outcomes as per the functional classification of Razemon and Baux. The authors did not categorize patients according to age, fracture pattern, or treatment modality. Similarly, Wang et al. 9 did not report a relationship between functional outcome and their participants’ age or fracture pattern in their study of 37 patients treated surgically (14 with physeal fractures and 23 with metaphyseal fractures). The mean NSS at final follow-up was 96.65 (range = 83–100), indicating an excellent outcome. The authors did not comment on any relationship between NSS and fracture pattern.
Factors associated with a poor clinical outcome
Higher grade of fracture displacement was associated with a worse outcome in three studies.6,10,15 For patients with severely displaced fractures treated surgically, two studies found no correlation between fracture severity and outcome,21,43 while Pavone et al. 6 found superior outcomes for patients with NH Grade III rather than Grade IV fractures. Older age at initial injury was predictive of a poorer patient-reported outcome score in three studies, especially for children ≥12 years old who were managed non-operatively.10,13,21 Chaus et al. 21 found that, for patients treated non-operatively, an overall worse treatment outcome was significantly associated with increasing age (p = 0.0043), but not with sex (p = 0.81). No other study commented on any correlation between sex and functional outcome.
Complications reported
Among the 546 patients treated surgically, there were 35 reported superficial infections,6,14,15,21,41,44 but no cases of deep infection or systemic sepsis. There were 21 reported cases of arm-length discrepancy >5 mm. Five of these occurred in the study by Wei et al., 13 in which all patients were managed conservatively, and 16 occurred in the study by Kohler et al., 15 in which the authors did not specify the treatment received. Wei et al. 13 also reported that eight patients had loss of reduction at final follow-up; five in the <11-year-old group and three in the ≥11-year-old group, two of whom required operative intervention. Two patients in the study by Pavone et al. 6 who were managed with closed reduction and percutaneous pin fixation were found to have loss of reduction at 2-week follow-up, requiring open reduction and internal fixation. There were 18 reported cases of severely displaced PHFs who underwent an unsuccessful closed reduction due to interposition of soft tissues within the fracture site, requiring subsequent open reduction.9–11,42 Twelve were due to entrapment of the long head of biceps tendon, and six were due to interposition of the periosteum. Moderate radiological deformities at final follow-up occurred in two patients treated surgically: one case of the humerus in varus with an Alsberg angle of <30 degrees, and one in valgus with an Alsberg angle of >65 degrees. 15 No study demonstrated a significant difference between the degree of deformity at final follow-up for patients treated surgically versus non-operatively, or for patients aged greater or less than 12 years.6,13,14 There were no cases of non-union reported in any study.6,9,11,13,42–44 Table 3 shows the relative numbers of complications for each grade as per the Clavien–Dindo classification.46,47
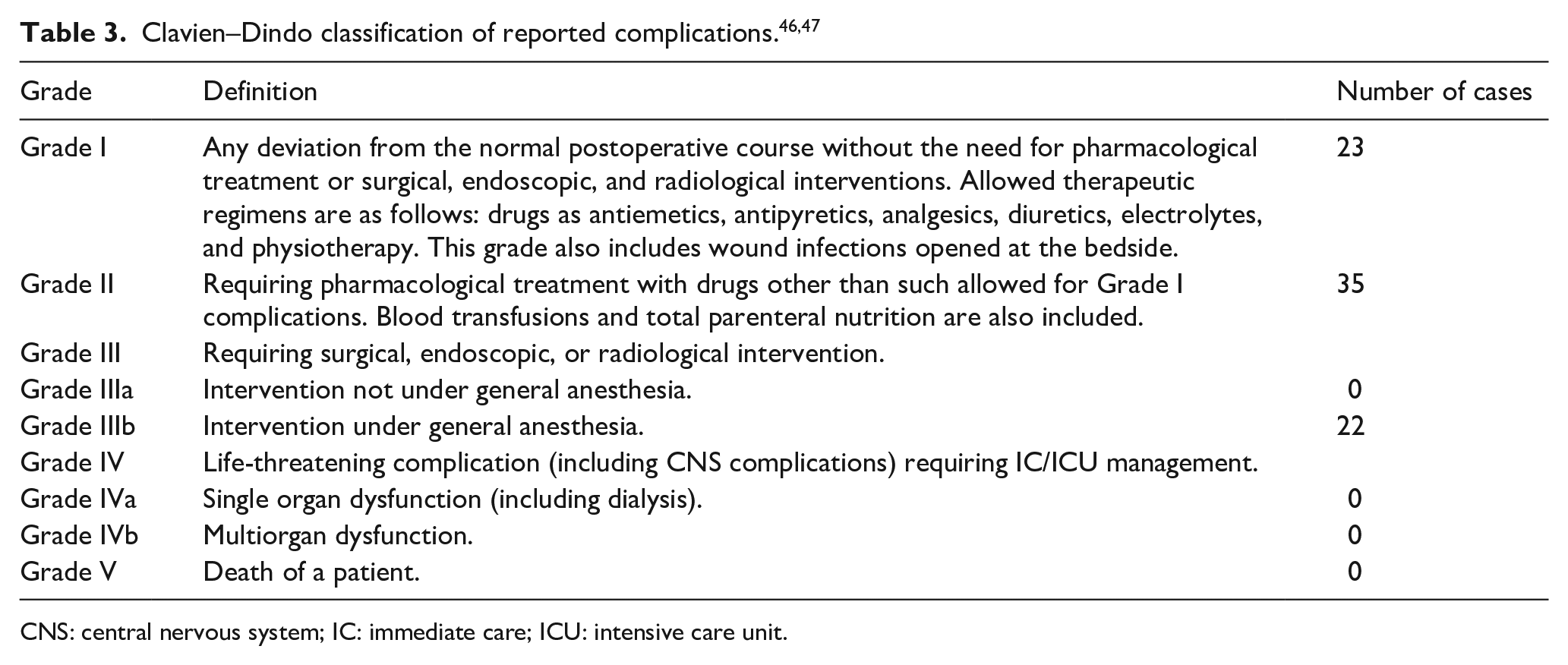
CNS: central nervous system; IC: immediate care; ICU: intensive care unit.
Discussion
In this review of functional and quality-of-life outcomes of pediatric PHFs, excellent functional outcomes were experienced for the vast majority (88.1%) of patients. This likely reflects the appropriate selection of treatment in each of the studies, for participants of different ages and degrees of fracture displacement. The oldest study suggested that the outcomes of pediatric PHFs are always satisfactory, regardless of their anatomy or treatment, and thus recommended non-operative management. 15 However, in this study, there were 16 patients with an arm-length discrepancy of >5 mm at final follow-up, and two with moderate persisting deformities. The other five cases of limb-length inequality occurred in Wei et al.’s 13 study, in which all fractures were treated conservatively regardless of the degree of displacement; two occurring in the group <11 years old and three in the group >11 years old. There was a general consensus in the studies written since 2013 that adolescents managed conservatively for severely displaced fractures are at risk of a poorer clinical outcome.6,9,10,13,14,21,41–44 Excellent outcomes were observed for patients ≥12 years with severely displaced PHFs treated surgically with K-wire fixation,6,14,44 ESIN,9,14,42,43 and external fixator.10,44 Pavone et al. 6 reported only two adolescent patients with Grade IV PHFs who had a “fair” outcome following surgery; the remaining 14 patients with Grade IV fractures treated surgically had either a good or excellent outcome. Similarly, Bisaccia et al. 41 found that 27 of their 31 participants treated surgically for an NH Grade IV PHF were “very satisfied,” with the other 4 being “satisfied” at final follow-up. Conversely, four (17.3%) patients with a mean age of 13.9 years had a less than desirable outcome after being managed non-operatively for a severely displaced PHF in the study by Chaus et al. 21 In their subgroup analysis of patients treated non-operatively, the authors identified that for every 1-year increase in age at injury, the odds ratio of a poor clinical outcome increased by a factor of 3.81. While there are possible selection and publication biases of recent studies aiming to demonstrate the efficacy of different surgical techniques for severely displaced PHFs in older children, it is evident that these patients do better with surgery. The ongoing dilemma is ascertaining a coherent guideline for what constitutes a surgical indication, on the basis of patient age and degree of fracture displacement. Based on their analysis of 28 patients with NH Grade III and Grade IV PHFs, Dobbs et al. 5 recommended a protocol for patients following closed reduction. For patients <7 years old, a post-reduction angulation of <70 degrees can be accepted; for patients aged 8–11 years, <60 degrees can be accepted; and for patients ≥12 years, <45 degrees can be accepted. It was concluded that greater deformities require open reduction and internal fixation. The protocol suggested by Binder et al. 10 was more aggressive for patients over 10 years old. They recommended non-operative management for children <10 years old with <20 degrees angulation, and surgery for children >10 years with >20 degrees angulation, citing an increased risk of soft tissue interposition in fractures with >20 degrees of angulation.
The results of this review confirm that NH Grade I and Grade II physeal PHFs, as well as metaphyseal fractures with <20 degrees angulation, can be managed non-operatively. The difficulty of determining an age- and displacement-based guideline for the management of severely displaced pediatric PHFs is due to the fact that the ability of the proximal humerus to remodel depends on the degree of skeletal maturity rather than exact chronological age. This is further confounded by the typically earlier age at which girls reach skeletal maturity compared to boys. While six studies excluded skeletally mature patients, the degree of skeletal maturity was not accounted for in any study, and the relationship between gender and functional outcome was only assessed in one study. 21 Designing a prospective study analyzing outcomes of pediatric PHFs for participants according to their bone age, chronological age, and sex may be useful to assist with this predicament.
Conclusion
An excellent functional outcome can be expected following conservative management for minimally displaced pediatric PHFs. The current literature suggests that adolescents may benefit from surgical management of NH Grade III and Grade IV PHFs; however, based on the current evidence, it is not possible to make recommendations regarding surgery versus non-operative management for individual patients. Prospective clinical trials are required to establish a guideline for the management of severely displaced PHFs in children and adolescents according to fracture displacement and the degree of skeletal maturity.
Supplemental Material
sj-docx-1-cho-10.1177_18632521221117445 – Supplemental material for Predictors of outcomes of proximal humerus fractures in children and adolescents: A systematic review
Supplemental material, sj-docx-1-cho-10.1177_18632521221117445 for Predictors of outcomes of proximal humerus fractures in children and adolescents: A systematic review by Samuel Abbot, Susanna Proudman, Bhuvanesh Ravichandran and Nicole Williams in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Samuel Abbot: literature search, screening of articles, data extraction, data analysis, and writing of the manuscript.
Susanna Proudman: data analysis, interpretation of data, and critical revision of the manuscript.
Bhuvanesh Ravichandran: screening of articles and data extraction.
Nicole Williams: data analysis, interpretation of data, and critical revision of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.