
Abstract
Background
Purpura fulminans is a rare and extremely severe infection, mostly due to Neisseria meningitidis. Nineteen patients were followed up immediately after the initial multivisceral failure in order to diagnose late-onset orthopedic sequelae. We report our experience with these 19 patients, in light of our medical follow-up protocol and surgical management.
Materials and methods
Nineteen patients were referred for acute purpura fulminans between 1987 and 2005 to our institution and followed up prospectively until the present. We collected information on all diagnosed orthopedic sequelae, all surgical procedures performed, and the actual orthopedic outcome.
Results
Fourteen patients developed at least one orthopedic sequel after a mean of 2 years delay, with a mean of 8.65 years follow-up (range 3–22 years). The most common presentation was lower limb physeal growth plate arrest in eight patients involving 18 growth plates, leading to five limb length discrepancies and 12 significant knee and/or ankle deviations. Patients were treated by completing epiphysiodesis in addition to limb lengthening and/or reaxation osteotomies, except for two patients, in which epiphysiolysis was performed. All outcomes are, to date, satisfactory, with both knee and ankle axes within the physiological range. Among the seven patients who underwent below-knee amputation, six needed stump revision because of skin conflict (4) or prosthetics misadaptation due to upper tibial varus (2). Regarding the upper limb, three patients presented with four cicatricial scar bands, one located on a ring finger, two at the first commissure, and one at the wrist (all were successfully treated by enlargement Z-plasties). Two patients developed hip avascular necrosis.
Conclusion
It is important for children diagnosed with meningococcal purpura fulminans to be followed up closely starting from the very beginning by a pediatric orthopedic surgeon. It ensures that late-onset orthopedic sequelae will be diagnosed early. In accordance to the literature, this study highlights the high rate of lower limb epiphysiodesis, above all other types of sequelae. This study reports a possible link between purpura fulminans and avascular necrosis of the hip.
Introduction
Purpura fulminans is an extremely severe form of infection, mainly due to Neisseria meningitidis or meningococcus. Meningococcus is a Gram-negative diplococcus found only in human respiratory secretions. It creates microthrombotic processes depriving the more distal and less oxygenated tissues from sufficient blood supply, and also deprivation in coagulation factors, leading to shock and multiple-organ damage [1, 2]. Orthopedic consequences may arise if histological structures linked to growth are concerned, except that the early diagnosis of these sequelae is often difficult.
Patients are mostly referred to orthopedic surgeons when late-onset sequelae appear, especially when purpura fulminans was initially treated in another hospital. The initial management and clinical presentation during the acute phase of purpura fulminans has been reported. It has given the opportunity to follow these children frequently thereafter, thus, offering the possibility to diagnose orthopedic sequelae almost as soon as they appeared. It is not yet well known which pathophysiological processes take part in the development of growth arrest [3], thus, there is little guidance in the literature regarding the management of late-onset orthopedic sequelae [4, 5]. Our aim in this retrospective study was to review the case histories in light of our medical follow-up protocol and surgical management in order to discuss what seems important to us regarding the improvement of long-term follow-up.
Materials and methods
Nineteen patients were referred to our institution for “acute meningococcal septicemia” between 1987 and 2005. After the primary orthopedic management during the acute phase of purpura fulminans, all children were subsequently followed-up in order to detect as early as possible any possible late-onset orthopedic sequelae.
There were 11 males and eight females, with a mean age of 3.97 years (range 0.1–16 years, standard deviation 3.3 years) at initial referral. Follow-up consisted of orthopedic check-ups every 6 months with clinical measurements of either the limbs or remaining stumps. Patients and their parents were asked to seek advice in the meantime as soon as they noticed any complication, such as lameness, leg length discrepancy, leg axis abnormality, disturbance in the range of motion of any joint, or the misadaptation of prosthetic fittings. In such cases, radiographs of the concerned joint and/or pangonograms were prescribed.
The clinical features of all of our 19 patients are summarized in Table 1.
Clinical features after follow-up in the 19 cases included in the series
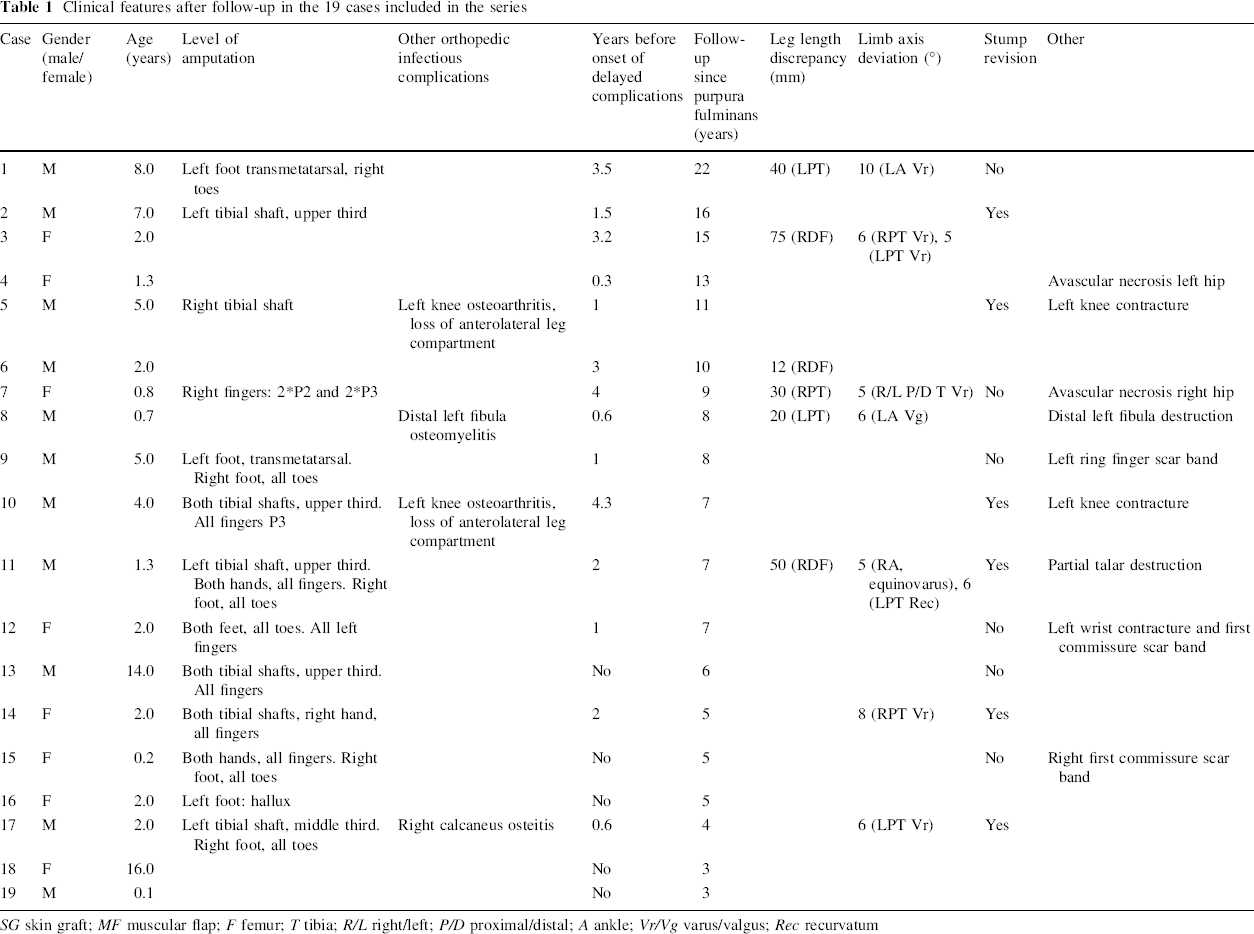
SG skin graft; MF muscular flap; F femur; T tibia; R/L right/left; P/D proximal/distal; A ankle; Vr/Vg varus/valgus; Rec recurvatum
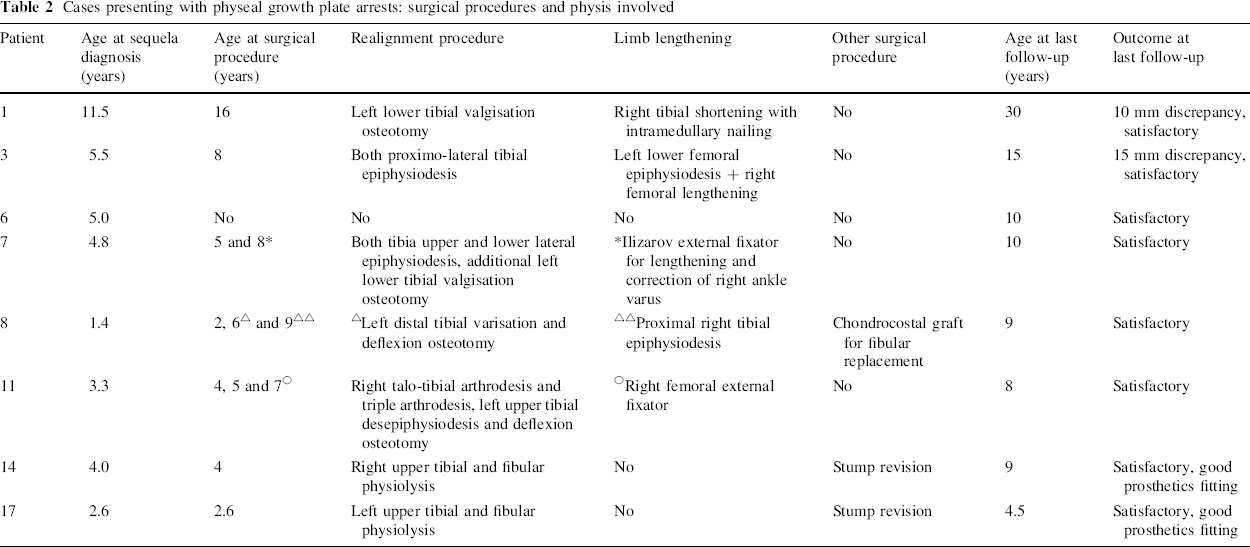
The delay between initial purpura fulminans and development of the first orthopedic sequel was noted. All surgical procedures performed for each patient, along with radiological measurement of the leg length discrepancy and axis deviation at the time of the surgical intervention was collected. The involved physis was mentioned; thus, it was chosen to highlight patients developing lower limb growth disturbance. The surgical procedures addressing these growth disturbances in these particular patients are summarized in Table 2. Leg length discrepancy was considered to be major when it was over 15 mm, as it requires surgery, whereas leg length discrepancy under 15 mm was considered to be moderate because it can be addressed by a compensation orthesis in the shoe. Outcome was assessed to be satisfactory when the leg length discrepancy was under 15 mm and both knee and ankle axes were within the physiological range until the latest follow-up, without lameness or pain during walking.
Cases presenting with physeal growth plate arrests: surgical procedures and physis involved
Results
Nineteen patients with a mean age of 3.97 years at the onset of the purpura fulminans were initially treated to address immediate orthopedic consequences of the purpura. Since growth disturbances were feared above all other late-onset sequelae to develop in these children, a semestrial follow-up to perform clinical examination was proposed. There is a mean of 8.6 years follow-up (range 3–22 years, standard deviation 4.5 years).
Fourteen patients developed, to date, at least one late-onset sequel, with a mean of 2 years delay (range 0.6–4.3 years).
The most common presentation was physeal growth plate arrest, resulting in axis deviation and/or limb length discrepancy. It concerned eight patients, involving 18 growth plate arrests. There were ten proximal tibial growth plate arrests, five distal tibial arrests, and three distal femoral arrests. These growth plate arrests led to four major limb length discrepancies of over 15 mm (three tibial and one femoral) and one moderate, and to 12 significant axis deviations (seven below-knee located at the upper tibial physis and five located at the distal tibial physis resulting in ankle deviation). Surgical procedures and involved physis in these eight patients are summarized in Table 2.
All ankle deviations were treated by performing both distal complete and definitive epiphysiodesis, with one patient (#11) presenting with additional equinovarus with partial talar destruction requiring tibiotalar arthrodesis and hind foot triple arthrodesis to prevent recurrence. Patient #8 presented with total post-infectious destruction of the distal left fibula, which required further chondrocostal grafting harvested on the right fifth thoracic rib. The patient, nonetheless, developed recurrence of ankle valgus due to further distal tibial growth plate arrest (Fig. 1).

Patient #8
Regarding the knee, all femoral growth plate arrests were complete and resulted only in exhibiting leg length discrepancy. As for the proximal tibial growth plates, there were three complete arrests exhibiting total length discrepancy and seven incomplete, including six varus deviations and one recurvatum. The seven varus deviations were treated by performing complementary proximal fibular and tibial epiphysiodesis before worsening of the deviation. The recurvatum needed both the completion of epiphysiodesis and a deflexion osteotomy.
In all cases, the outcome has proven to be satisfactory at the latest follow-up.
Among the seven patients who underwent below-knee amputation in the initial phase of purpura fulminans, six needed further stump revision. Two patients included in the previous paragraph presented with difficulty in fitting prosthetics due to upper tibial varus, thus, needing physiodesis of both the tibia and fibula. The remaining four patients presented with a skin conflict and another osteomyoplasty was performed, this time without any recurrence of prosthetics misadaptation.
Regarding the upper limb, there were three patients presenting with four cicatricial scar bands, one located on a ring finger, two at the first commissure, and one at the wrist. All were successfully treated by enlargement Z-plasties.
In addition to these three most commonly encountered sequelae, two patients developed knee contracture. Both patients suffered from specific knee osteoarthritis shortly after the initial purpura fulminans, which can explain this outcome. Physiotherapy was unsuccessfully tried, and these children will probably benefit from arthrolysis.
Two patients, #4 and #7, developed left hip osteochondritis. It is impossible to say if there is a particular ischemic link between the previous history of purpura fulminans and avascular necrosis (Fig. 2).
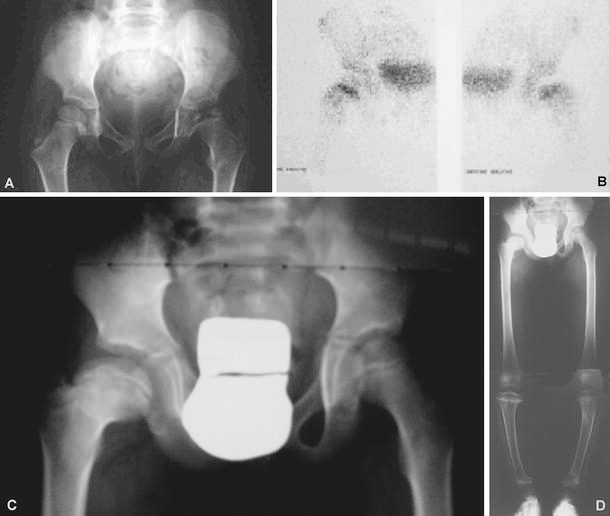
Patient #4:
Discussion
Early sequelae after the initial phase of purpura fulminans have already been reported several times in the literature and between 50 and 60% of survivors have major morbidity [5]. On the contrary, it is not yet known the exact incidence of late-onset orthopedic sequelae in this particular population. We have had the opportunity to follow up this series of 19 patients from the very beginning of their disease until the present. Unlike other studies, all 19 patients come from the same hospital and were followed by the same surgical team, thus, facilitating the precise collection of all possible sequelae. However, having 14 patients out of 19 (73.7% of our population) presenting with a late orthopedic complication, it remains difficult with such a short series to extrapolate solid figures from this study. As has already been noted during acute phase management, it seems to be rather unpredictable which patient will develop what sequel. Therefore, it was decided to follow up closely every patient who was referred to us for purpura fulminans in order to detect early physeal growth arrests essentially, since it is one of the most frequent and anciently described complications [3, 6].
There are several interesting comments that can be made regarding our series in comparison with the literature. Bache and Torode [5] identified 41 growth arrests, all but five in the lower limb. All of our 18 growth arrests concerned the lower limb too. Since there was initially quite a few skin necrosis in the upper limb, it seems that growth arrests do occur preferentially under areas of cutaneous scarring. Bache and Torode report 16 patients out of a cohort of 40 children presenting major sequelae after meningococcal septicemia (40%), which is exactly the same percentage as in our study (8 out of 19 patients) and Belthur et al. [4] report 23 out of 24 (almost 96%). These studies, though focused on similar patients, have very different figures concerning growth disturbances because Bache and Torode's study is a follow-up of patients treated for meningococcal septicemia, while the Belthur et al. paper focuses strictly on children referred for orthopedic sequelae. In light of physiopathology, that is, blood shunt and prolonged hypo oxygenation during all phases of shock and multiorgan failure, it seems insufficient to acknowledge this unique factor as being solely responsible for growth arrest. While our figures confirm the fact that growth arrests are found preferentially peripherally and in the lower limb, it can be seen from Table 1 that there seems to be no link between initial presentation, gravity, and early sequelae on the one hand, and further development of late-onset sequelae on the other hand (Graph 1). It is, unfortunately, too small a population to allow any reliable statistical analysis, and it is only a general feeling that can be underlined here. Of the three patients with extensive skin necrosis >15%, none developed growth plate arrests, but this seems to be coincidental. Though these patients have had tibial amputation, there were no clinical hints that proximal tibial or distal femoral growth arrest had occurred. Moreover, there seems to be no topographical link between the location of skin necrosis and the development of growth plate arrest.
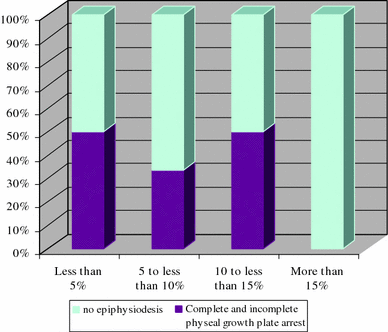
Occurrence of physeal growth plate arrest with regard to initial soft tissue necrosis
No large series assessing numerically leg length discrepancy and axis deviation were found in the literature. Our figures represent radiological measurements before surgical treatment, which has a mean of 37.8 mm overall length discrepancy, and deviations that were between 5 and 10°. By following children every 6 months at least, it was possible to detect growth arrests at their commencement, allowing better planning for surgical correction and surgical options that were, in the majority, complementary to epiphysiodesis. Thus, lengthening could be performed for smaller amplitudes (patients #3 and #7). Patient #1 is the oldest case, and is the only patient who underwent tibial shaft shortening with intramedullary nailing. We do not perform this surgical technique any more, since it is at high risk of compartment syndrome.
Axis deviations were all treated by completing epiphysiodesis to prevent recurrence, along with an additional osteotomy when needed. Only one complex ankle deviation needed correction with an Ilizarov device (patient #7). There were no recurrences at the latest follow-up. Six out of 8 children are still growing, and it is reasonable to think that they will very likely need limb lengthening and contralateral epiphysiodesis, even though the outcome is, at present, satisfactory. Physeal magnetic resonance imaging (MRI) was performed in the most recent cases to assess the surface of epiphysiodesis bridging. When under 35% of the total physeal surface, desepiphysiodesis was performed using Palacos® Bone Cement (Zimmer™). It could be done only in one case (patient #11) successfully. It is a very challenging technique and it should be an option only in younger children, as leg length discrepancy will inevitably be greater and more difficult to address if the completion of epiphysiodesis is surgically completed. However, if the desepiphysiodesis fails, it will more likely result in a complete epiphysiodesis, but it will have at least given an additional opportunity for a given child to regain growth.
Sterilization of the proximal fibular growth plate in children with below-knee amputation is strongly advocated in our department, as it has been needed to perform stump revision for prosthetics misadaptation because of tibial varus resulting from differential fibular growth. Belthur et al. report two similar cases. However, it is well known that, in young children, below-knee amputation often leads to secondary upper tibial varus, regardless of the amputation indication [7].
Besides these two cases, a high rate of tibial stump revision (6 out of 8 patients) was noted. It seems that there was initial overconfidence with the underlying tissue quality, and some time after osteomyoplasty, the distal tip of the stump gradually melted in such a way that the cross-section of the tibia provoked skin ulceration when walking was begun with prosthetics. Again, there seems to be no link between this phenomenon and the initial presentation or skin necrosis surface (which should be considered only as an immediate prognosis indicator [8]). The tibial shaft had to be shortened while performing felt tips because secondary osteomyoplasty proved to be very difficult given the quality of the underlying muscles. It seems that one should consider very carefully the level of amputation regarding this possible torpid evolution.
In this series, two cases of avascular necrosis of the hip diagnosed in children followed up for purpura fulminans sequelae are reported. It is very well known on the one hand that systemic meningococcemia can cause, alike any other septicemia, growth disturbances, joint hyperpression, chondrolysis, and, sometimes, epiphyseal necrosis [9]. On the other hand, the exact physiopathology of osteochondritis dissecans is not well known, transient femoral head ischemia being the most probable cause. These two physiopathological paths could easily be in complete agreement with osteochondritis dissecans being a consequence of purpura fulminans multiorgan ischemic failure. However, no extrapolation can be made from these two observations and further studies will tell us if we are right to suspect such an association. Fernández et al. [6] also reported such changes in the hip after severe meningococcic sepsis.
To conclude, early detection allows pediatric orthopedic surgeons to deal with smaller leg length discrepancies and axis deviations, which can be addressed with less aggressive surgical options. Two patients were referred by another hospital to our unit many years after a purpura fulminans without any skin necrosis, and presented with extensive growth plate arrest which was very difficult to address. Word should be given in every hospital in which purpura fulminans is dealt with, that it is of the most extreme importance that children should be referred to orthopedic and/or plastic surgeons very early in order to initiate a very sharp orthopedic follow-up, regardless of the initial clinical presentation. We are strongly convinced that such measures can help spare children from further more invasive surgical procedures, having had the unique opportunity to follow up this series of children from the very beginning of their disease until the present. It has not proved very informative since the small number of patients does not allow statistical analysis, but it seems that purpura fulminans is a very unpredictable disease both regarding initial sequelae and late-onset sequelae. Furthermore, there seems to be no links between initial presentation and orthopedic outcome several years after the initial shock phase. Further studies including more children will, possibly, help us to both define a better prognostic pattern and to understand the long-term ischemic consequences of the disease.