
Abstract
Purpose
Paediatric femur fractures are commonly encountered and often successfully managed with spica casting. Despite spica casting's long history there is little formal guidance for optimal outcomes and no consolidation of existing literature. The purpose of this study is to review the available literature regarding the use of spica casting for the management of paediatric diaphyseal femur fractures.
Methods
The PubMed database was queried for all research articles including the phrase “spica”. A total of 788 abstracts were reviewed for relevance to the current study. Data was extracted from all available research studies which specified tolerance for fracture angulation or shortening in the cast. Additionally, all articles describing alternative materials, methods for spica application, and complications of spica casting were reviewed.
Results
In all, 106 articles were found relevant to the management of diaphyseal femur fractures in the paediatric population. The aggregated, accepted fracture shortening decreased from 16 mm to 18 mm before age ten years to 12 mm to 14 mm after puberty. Aggregated, accepted angulation decreased from 14° to 16° varus/valgus and 18° to 22° pro/recurvatum before age two years, to 6° to 8° and 10° to 12° by puberty, respectively. The overall reported complication rate was 19.6%, with the most common complication being skin compromise in 8.2% of patients, followed by unacceptable angulation at the fracture site in 4.2% of patients and excessive limb shortening in 1.9% of patients.
Conclusion
This article reviews the available spica casting literature and compiles the available data. Spica casting offers a safe, effective means for definitive management of paediatric diaphyseal femur fractures. Future research identifying the rate and pattern of remodelling as it relates to angulation and shortening at various patient ages, particularly beyond the aforementioned norms, would be valuable to identify true biological tolerances versus accepted expert opinion.
Level of evidence Level II
Review of level II evidence
Introduction
Hip spica casting has been a widely used, effective method for the nonoperative management of paediatric diaphyseal femur fractures for over 80 years. 1 With an estimated 1.6% of children sustaining a femur fracture, femur fractures represent the third most common lower extremity fracture. 2 Among North American paediatric orthopaedic surgeons, spica casting is overwhelmingly the preferred management for patients less than six years old with any diaphyseal femur fractures, excluding polytrauma. 3 The most recent American Academy of Orthopaedic Surgery guidelines for the treatment of diaphyseal femur fractures recommends the use of spica casting for children between six months and five years old with < 20 mm of fracture shortening. 4 However, we were unable to identify any comprehensive review of available literature on spica casting.
The purpose of this systematic literature review is to consolidate the English language literature and present the best evidence for the use of spica casting in the management of paediatric diaphyseal femur fractures.
Literature search
A comprehensive PubMed search was performed to identify all English-language articles relating to spica casting of diaphyseal femur fractures. An initial search was performed for all articles containing the word “spica” from 1900 until March of 2017, which generated 788 results. Titles and abstracts were reviewed for relevance to the current study. Only English-language articles relating to hip and femur fractures were included for detailed evaluation. All others (e.g. thumb or shoulder spica, adult hip fracture and developmental dysplasia of the hip) were excluded. We additionally pursued all references of reviewed articles to further identify relevant literature. We selected 106 articles which met inclusion criteria and were related to the current topic.
Overview of the literature
Limb immobilization for the treatment of fracture has been dated as far back as the Ancient Egyptians, based on archaeological discoveries of wooden sticks surrounding a preserved mummy with a femur fracture. 5 The development of plaster impregnated fabric strips which allowed the modern techniques of splinting and casting has been attributed to Mathijsen in 1851. 6 Applying and maintaining controlled traction specifically to femur fractures may have originated with the Thomas splint, developed in 1865, and was popularized during World War I. 7 These splints were for adults and were valued for their relative ease of application, enablement of patient transportation and in some instances allowed for patient ambulation. The earliest article we could find specifically mentioning hip spica casting for paediatric femur fractures was by Moore and Shafer, 1 who described a fixed traction spica in 1948. Dameron and Thompson 8 provided the first available detailed description of spica casting application and short-term outcomes in 1959. Since these initial articles, five randomized control trials,9–13 37 cohort studies,1,14–50 37 retrospective reviews,8,51–86 13 technique articles,87–99 and three guidelines4,100,101 have been published relating to the use of spica casting in paediatric diaphyseal femur fractures. This review focuses on three major aspects of over five decades of literature: 1) fracture position tolerance to prevent unacceptable limb alignment; 2) complications associated with spica casts; and 3) technique and material recommendations. Also included in this review are other notable spica cast concepts that do not fall within those main categories.
Fracture position tolerance
Traction and shortening
The degree of acceptable shortening in paediatric diaphyseal femur fractures has been the topic of academic interest since Aitken's 1940 article 51 detailing the significant overgrowth phenomenon seen in long-term follow-up of paediatric femur fractures treated with traction. We found 53 articles identifying their shortening tolerance at initial casting or at follow-up.8,9,12–21,23,25–27,29–31,36,38,39,41,42,45–48,50,53,55,56,60,62–67,69, 71,73,74,76,79–83,89,97,100,102,103 The most recent (2009) American Academy of Orthopaedic Surgeons Guidelines for the management of diaphyseal femur fractures in the paediatric population is to use spica casting for those with < 2 cm of shortening. 4 The mean and sd of all studies which specified their tolerances is shown in Figure 1. Tolerance values for the initial casting versus the final measurements at follow-up were evaluated separately, but found to have < 0.2 cm difference at all ages (data not shown). This aggregated analysis shows that throughout the literature, 17 mm to 18 mm shortening tolerance was acceptable until age ten years, with acceptable shortening decreasing to between 12 mm to 14 mm at the age of puberty and beyond. The rates of final shortening which exceeded acceptable limits were too low in any reported study to identify initial fracture shortening which correlated with increased rates of unacceptable shortening at final radiographic or clinical follow-up.
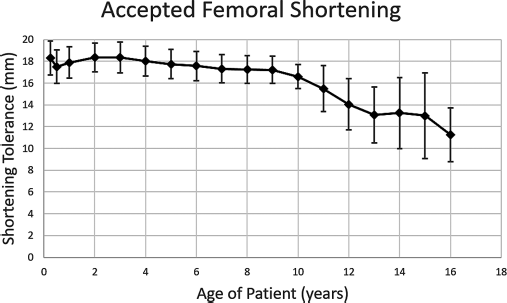
Limb shortening limitations determined to be radiographically or clinically acceptable. Combined tolerances from 52 primary research studies.
Overgrowth phenomenon
Aitken 51 identified the phenomenon that the shortened, fractured femurs of young children may outgrow the uninjured side. Our review is not intended to review the overgrowth phenomenon, but Hariga et al's 62 review determined that overgrowth is more influenced by initial shortening than factors such as age, gender, treatment or type of fracture. Femoral overgrowth tends to peak in the first 18 months following fracture.43,71 In patients younger than two years old, Nork et al showed that the average overgrowth in long-term follow-up was 5 mm. 73 Three long-term, follow-up studies have shown the average overgrowth to be between 9.6 mm and 13 mm.51,62,71 Frech-Dorfler et al, 61 in the longest available follow-up which looks at overgrowth, showed that in unstable fractures with an initial average shortening of 12 mm, 59.1% of patients had < 0.25 cm leg-length discrepancy and only one patient (4.5%) had a persistent leg-length discrepancy > 1 cm which was due to excessive overgrowth and not shortening at 7.5 year follow-up.
Angulation in the frontal and sagittal planes
We found 35 articles specifying accepted varus or valgus angulation8,9,11,13–16,18–21,23,25–27,29–31,36,38,41,45,47,48,53,55,56,60,65,69,74, 79,80,82,102 and 34 articles specifying the accepted sagittal plane angulation8,9,11,13–16,18–21,23,25–27,29,30,36,38,41,45,47,48,53,55, 60,65,69,74,76,79,80,82,102. Figure 2 displays the mean and sd of accepted varus/valgus angulation at initial casting based on patient age. Approximately 16° varus or valgus is accepted for patients under two years old, decreasing to 6° for adolescents treated with a spica cast. Figure 3 displays the accepted angulation in the sagittal plane. Again, a general trend exists of less accepted deformity with increasing age, although at all ages the sagittal plane tolerance is greater than the frontal plane tolerance. It should be emphasized that these graphs represent only each author's preference. There are no longitudinal studies that have followed patients to correlate angular deformity to eventual femur alignment or leg length equality at skeletal maturity.
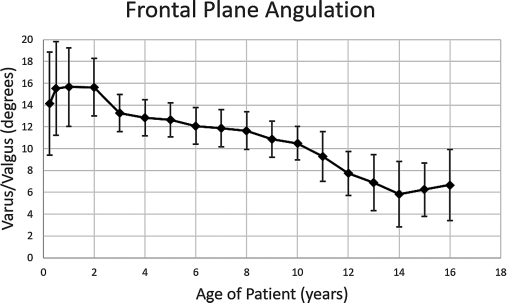
Aggregated accepted coronal plane radiographic angulation (varus/valgus) from 35 primary research articles.
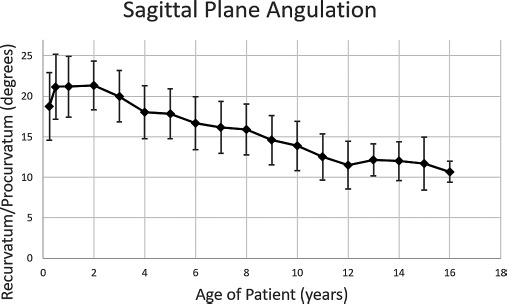
Aggregated accepted sagittal plane radiographic angulation (procurvatum/recurvatum) from 33 primary research articles.
Complications
Minor complications
The most commonly reported complication from spica casting for paediatric femur fractures has been skin breakdown and other skin complications. Table 1 summarizes the complications of spica cast treatment identified in studies over the last ten years which specified the total number of patients in the studies and addressed complications. Only studies from 2007 to 2017 were included to minimize the effect of older techniques for casting, traction and materials. The most commonly reported radiographic complication was excessive final angulation; however, very few authors report long-term outcomes to provide insight whether the angulation remains purely radiographically substantial or represents a clinically significant complication resulting in limb length discrepancy, pain or re-fracture. The rate of cast removal or revision varied widely among studies and the reasons were inconsistently reported. Some authors reported increased angulation as a complication but did not specify whether this was detected at an early visit and accepted, or developed too late in the course to consider revision casting. Due to the inconsistent clarity of indications for re-casting, as well as the lack of long-term outcome studies showing clinical implications of the various unacceptable radiographic positioning assessments, we noted there is inadequate data to recommend a specific angulation or shortening as a tolerance limit.
Compilation of all complications specified in randomized control trials, cohort studies, or retrospective reviews 2007 to 2017
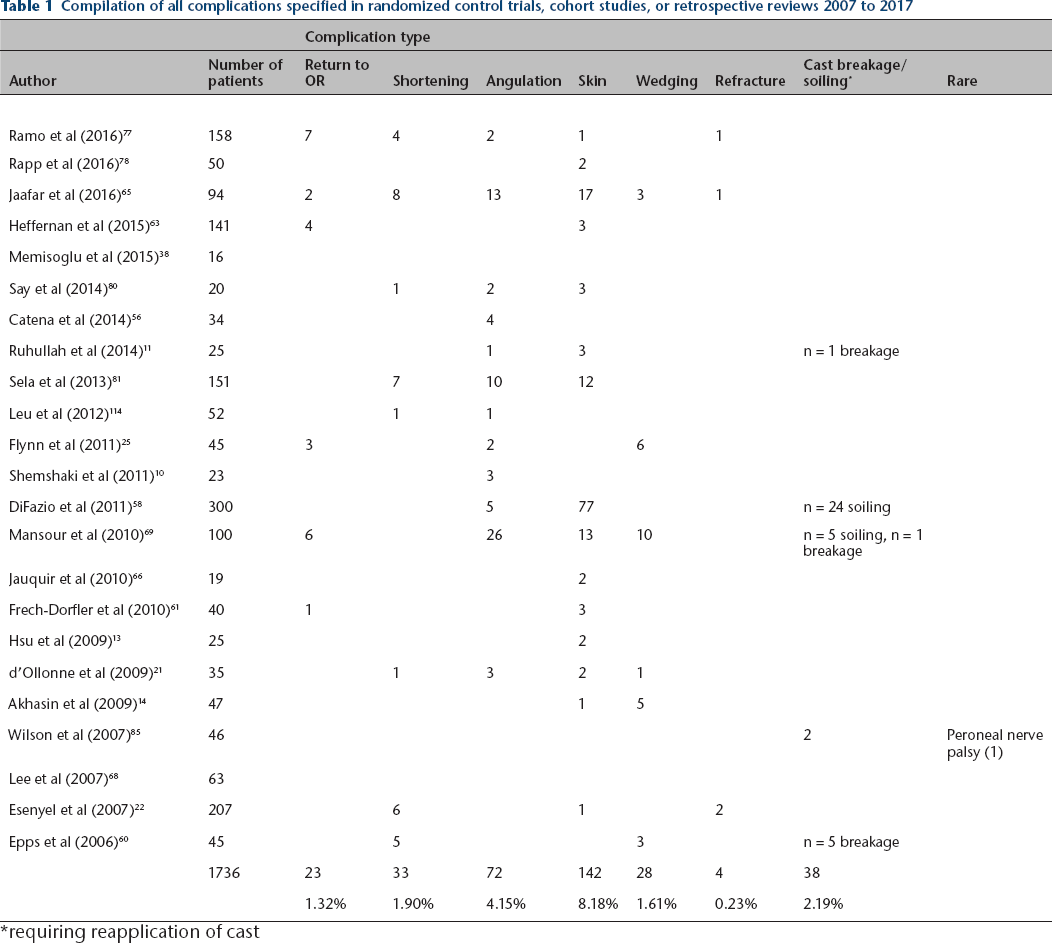
requiring reapplication of cast
Devastating complications
Severe complications of spica casting in children, while rare, are noted in multiple case series in the literature. One author noted superior mesenteric artery syndrome in a 10-year-old female 104 and, subsequently, techniques for abdominal windows93,96 and casting with adequate abdominal space to incorporate room for expansion during inhalation89,91 have been described to avoid this specific complication. Mubarak et al 105 detailed a series of nine patients who developed compartment syndrome of the lower extremity in 90/90 spica casts fabricated with the below-knee cast portion used to impart traction on the femur while the above-knee cast portion was molded. This author recommended casting the hip and knee both at 45°, not elevating the cast, and not applying traction on the below-knee cast portion during application of the cast after reduction of the fracture. While no large cohort or retrospective studies in paediatric spica casting have suggested baseline rates of compartment syndrome or superior mesenteric artery syndrome, the techniques used in casting should be targeted at avoiding these rare, but serious, complications.
Techniques
In 1981, Kumar 106 described and illustrated what most orthopaedists would probably consider representative of modern standard spica cast fabrication technique. While his work is well cited, there are variations proposed in literature. A detailed description of the multiple relatively minor modifications described is beyond the scope of this review. Broadly, these variations include optimal positioning of patients during casting,32,88,90,91 techniques to prevent soilage,30,95 variations in home-care for spica-casted patients,92,98 and materials used in the casting process.99,107
Traction
In all, 51 articles specifically mentioned the use or non-use traction in their description of spica application and the course of patient care. Of the articles detailing the use of traction, seven specifically had no traction,12,15,23,25,27,61,103 12 used isolated skin traction,20–22,35,36,46,48,53,59,62,68,76 and 19 used skeletal traction on some, if not all, of their patients via a Kirschner wire applied to either the distal femur,10,18,19,24,33,38,41,57,64,67,72,80,94 proximal tibia13,26,45,97 or unspecified pin location.52,82 Eight retrospective reviews had patients within their cohorts who had received either skin traction or skeletal traction,17,34,40,56,64,82,86,102 but no direct comparison was made between these two treatment options. Overall, in the last ten years, authors have preferred either no traction or skeletal traction, with only three articles21,62,68 explicitly using skin traction.
Double-leg versus single-leg spica casting
There are multiple variations on the extent of casting needed for adequate femoral fixation when using a spica cast for primary management. In 1976, Irani et al 30 recommended not incorporating the foot into the spica cast, suggesting that pressure against the foot plate increases femoral shortening. Four articles have studied the use of less-restrictive spica casting in the paediatric population. Leu et al 12 performed a randomized controlled trial comparing single-leg versus double-leg casts in 52 patients which showed similar rates of fracture shortening, angulation and time in cast, but found that single-leg patients had improved fit in car seats and lower caregiver burden. Flynn et al 25 compared single-leg casts to double-leg casts with the single-leg group having increased rate of wedge adjustment (26% versus 4%) but decreased malunion (0% versus 8%), both statistically significant, and a similar need for repeat spica casting (5% versus 8%). 25 Epps et al 60 reviewed single-leg casting and reported that five of 45 patients’ casts failed at the hip joint and an additional five of 45 patients had shortening requiring recasting or operation; one additional patient fell sustaining a contralateral tibia fracture without shortening or increased angulation of either fracture three years later. Jaafar et al 65 showed similar rates for repeat reduction or cast wedging in single-leg versus double-leg casting. Overall, the rates of complication and acceptable radiographic outcome appear similar in all head-to-head comparisons of single-leg casts versus double-leg spica casting in the treatment of paediatric diaphyseal femur fractures.
Materials and mechanics
In all, 19 articles specifically mentioned the use or non-use of a cross-bar in their applications of the spica casting. Bar materials include wood,22,29,40,108 fiberglass12,89 and plaster 1 while the remainder of studies do not use a bar.14,19,25,28,35,44,55,60,74,87,90,106
We found no studies comparing the failure rates, need for cast changes or cost between fiberglass spica casts and plaster-based casts in the treatment of paediatric diaphyseal femur fractures. However, Walter et al 99 suggests that using Gore-Tex liner (Newark, Delaware) instead of standard cotton may result in fewer cast changes for soilage, based on its use in extremity fractures. 109
Wan et al 110 performed a biomechanical analysis of the strength of Kumar's standard spica application versus their proposed method incorporating strut wraps beneath the hips of the patient imparting increased stiffness and load-to-failure at the hip joint. This was a purely mechanical study and no patient outcomes or comparisons were reported.
Parental care
Few articles detail care of the children from the perspective of the parents or other caregivers. Common parental complaints and difficulty with management of these patients include how to maintain routine child washing, prevent cast soilage from excretion, manage the increased weight of the child in the cast and transportation.29,44,92 Leu et al 12 and Flynn et al 25 surveyed parents or caregivers about their experience in double-leg versus single-leg spica casts and one-and-a-half leg versus walking cast, respectively. In both studies, the parents preferred the less restrictive of the two casts. The walking cast had a significantly lower Impact on Family Score compared with the one-and-a-half cast, while the single-leg cast resulted in fewer parent days off work, easier patient transport, and increased ease of sitting when compared with the two-leg cast.
Comparison to operative techniques
Common operative options for paediatric diaphyseal femur fractures include plating, flexible titanium nails and even conventional intramedullary nails for taller or heavier children. Comparing the surgical outcomes with one another and with spica casting is beyond the scope of the current article. A notable randomized control trial by Shemshaki et al 10 showed that parents of older children, aged six to 12 years, preferred elastic nails over spica casting.
Summary
The spica cast has been used as a definitive treatment option for paediatric diaphyseal femur fractures since the mid-20th century and remains an indispensable skill for an orthopaedist. A Cochrane review was published in 2014 of ten randomized and quasi-randomized controlled trials of diaphyseal femur fracture management in patients under age 18 years. 111 Seven studies were on operative options, and three reported on nonoperative care. One author 112 noted 4/21 children immediately placed in a spica cast had shortening or excessive angulation whereas only 1/21 children did who had skin traction before spica casting; this difference was not significant. Another author 113 found 6/15 patients treated with a functional brace and 11/27 patients treated with a spica cast had radiographic malunion at five years (not significantly different) and both groups had a mean hospitalization of 26 days. The third author 114 compared single- versus double-leg casts and was discussed elsewhere in our review. The authors of the Cochrane review assessed the quality of their evidence to be low for most outcomes measured and did not find adequate support to make guidelines or specific recommendations for nonoperative care. In this situation of insufficient prospective trial data, along with the most recent comprehensive review of nonoperative management techniques of paediatric femur fractures being over 15 years old, we felt it valuable to provide an updated assessment and interpretation of available literature.
Excessive radiographic shortening or angulation as defined in each reviewed study is a complication in 6.1% of patient based on our compiled data. Clinically significant adverse outcomes as patients grow, while lacking data from literature, likely represent an even smaller proportion of those who had radiographically unacceptable outcomes. With the currently available data, we find it difficult to identify specific tolerance limits for varus/valgus, procurvatum/recurvatum or shortening, but we were able to review what has been acceptable radiographically in each year of life to help inform future consensus. Our review does suggest that for patients under ten years old, 10° to 20° of angulation in any plane and 10 mm to 20 mm of shortening are consistent with published tolerances and can be expected to have < 10% rate of radiographic ‘failure’ and even lower rates of clinically significant complication. Variations in technique and home care may allow for easier, more durable and cost-effective treatment of these fractures. The devastating and common complications of spica casting treatment are reviewed and some recommendations exist for complication avoidance, but there is a scarcity of clinical evidence behind these recommendations.
Spica casting for the management of diaphyseal paediatric femur fractures continues to be a mainstay of modern orthopaedic management despite the push for operative management of paediatric fractures. This review investigates the available literature for the use of spica casting for the definitive management of diaphyseal femur fractures in the paediatric population.
Footnotes
Open access
This article is distributed under the terms of the Creative Commons Attribution-Non Commercial 4.0 International (CC BY-NC 4.0) licence (https://creativecommons.org/licenses/by-nc/4.0/) which permits non-commercial use, reproduction and distribution of the work without further permission provided the original work is attributed.