
Abstract
Purpose
Spica casting of femoral shaft fractures is standard practice for young children. In 1983, Dr. Rang published an illustration demonstrating that radiographs can be misleading when measuring femoral fracture shortening. Today, fluoroscopy is used to determine shortening after closed reduction and spica casting. This paper aims to determine the accuracy of fluoroscopy when measuring 25 mm of shortening in a femur fracture sawbone model.
Methods
Magnification, elevation and angulation were evaluated using a femur fracture sawbone model with a fixed overlap of 25 mm. Two C-arm machines used in clinical practice were studied: the OEC 9900 Elite GE C-arm and the Fluoroscan InSight mini C-arm.
Results
The OEC 9900 Elite GE C-arm demonstrated a 1.75 × magnification. The Fluoroscan InSight mini C-arm demonstrated a 2.5 × magnification. An 11% and a 17% magnification with elevation of the femur to 8 cm occurred using the OEC 9900 Elite GE and the Fluoroscan InSight mini C-arm respectively. Changing the tube angulation from 0° to 60° resulted in a 36% and 16% change in measured femur fracture shortening on the OEC C-arm and Fluoroscan mini C-arm respectively.
Conclusion
C-arm images are inaccurate. When measuring 25 mm of shortening of a paediatric femur fracture, each machine has a unique amount of magnification that should be determined and accounted for in clinical practice. Elevation of the femur above the C-arm receiver and angulation of the femur further increase the inaccuracies when measuring 25 mm of fracture shortening. Images perpendicular to the fracture are most accurate.
Introduction
Femoral shaft fractures in children heal with an overgrowth phenomenon. Unique to children, overgrowth often helps to equalise a limb length discrepancy following a femur fracture. Shapiro 1 reported that in patients aged less than 13 years the average overgrowth at the femur was 0.92 cm (0.4 to 2.7). In addition, overgrowth at the tibia was 0.29 cm (0.1 to 0.5). Overgrowth occurred in children age < 12-years-old with a femur fracture.
Acceptable fracture shortening at initial reduction varies by author from < 1.5 cm to 3.5 cm.2–4 Recent literature suggests that fractures with < 25 mm of shortening in patients up to six years of age can be treated with early spica casting.5–9 In such cases, overgrowth will usually restore femoral length to < 1 cm of inequality. Fractures with > 25 mm of shortening may require treatment with traction, plating or external fixation in order to minimise excess shortening. 5
After closed reduction and spica casting, accurate measurement of fracture shortening is pivotal in the treatment of femoral shaft fracture in young children. In 1983, Rang 10 demonstrated that fracture shortening based on radiographs can be inaccurate. The purpose of this paper is to expand on this and to determine the accuracy of fluoroscopic radiographs when measuring 25 mm of shortening in a femoral fracture sawbone model.
Materials and methods
A sawbone model of a femur fracture with a fixed overlap of 25 mm was used. The radiographic parameters of magnification, elevation and angulation were investigated. Each parameter was tested on an OEC 9900 Elite GE C-arm (General Electric Health, Inc., Chicago, Illinois) and on the Fluoroscan InSight mini C-arm (Hologic, Inc., Newark, Delaware). These two image-intensifiers are used in the operating room at Penn State College of Medicine and were available for our study. The fracture line was created in the middle third of the diaphysis with a transverse angle of 20°. The two free ends of the fracture were secured with an overlap of 25 mm.
To test the effect of radiographic magnification, an object of known diameter (a metal coin of 20 mm diameter) was imaged directly onto the image intensifier of the C-arm OEC 9900 Elite GE and Fluoroscan InSight mini C-arm. We placed the metal coin on the receiver, aligned parallel to the shaft of the femur.
To investigate image distortion related to change in distance from x-ray source to the fracture, the sawbone model was imaged at 0 cm, 2 cm and 8 cm above the plate receiver on the C-arm OEC 9900 Elite GE as well as on the Fluoroscan InSight mini C-arm.
To test the effect of beam angulation on fracture shortening, interpretation images of the sawbone model were taken at 10° increments ranging from 0° to 60° with both C-arms. The length of overlap was measured on the radiograph screen image as commonly done in clinical practice (Fig 1). Of note, angled radiographs often lead to a double contour of the bone edge at the fracture site, especially with oblique and spiral fractures. To minimise errors in measurement, we measured the leading bone edge at the fracture site.
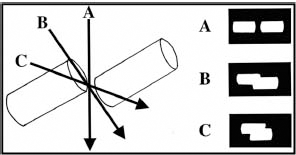
The fracture may appear shortened or lengthened based on the angle at which the x-ray is taken. Line B, perpendicular to the fracture, is most accurate.
Results
Magnification
The OEC 9900 Elite GE C-arm magnified the diameter of a metal coin 1.5 × and the on-screen fracture overlap was magnified 1.3 ×. The Fluoroscan InSight mini C-arm magnified the diameter of a metal coin 2 × and the on-screen fracture overlap was magnified 1.7 ×. Compared with the metal coin, which was placed directly onto the C-arm image intensifier, the sawbones fracture model by its design was elevated 2.5 cm above the image intensifier.
Elevation of the femur above the C-arm receiver
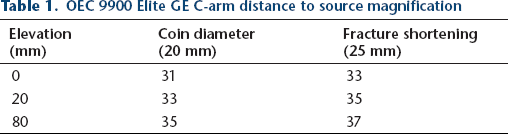
The human femur is surrounded by varying thickness of soft tissue and therefore will be elevated above the C-arm image intensifier. Elevation of the femur sawbone model above the image intensifier resulted in image magnification (Table 1). When using the OEC 9900 Elite GE C-arm, elevation of the femur sawbone model to 8 cm resulted in an 11% increase in image size. When using the Fluoroscan InSight mini C-arm, elevation of the femur sawbone model to 8 cm resulted in a 17% increase in image size.
OEC 9900 Elite GE C-arm distance to source magnification
Angulation of the femur fracture
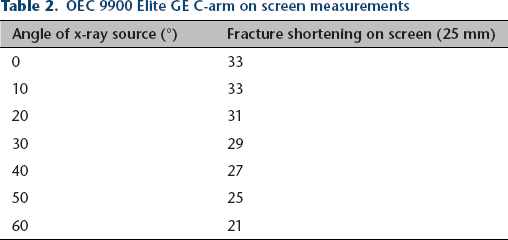
Fracture overlap ranged from 33 mm to 21 mm as angulation of the femur increased from perpendicular to the C-arm (0°) to 60°on the OEC 9900 Elite GE C-arm (Table 2). Fracture overlap ranged from 45 mm to 38 mm as angulation of the femur increased from perpendicular (0°) to 60° using the Fluoroscan InSight mini C-arm (Table 3).
OEC 9900 Elite GE C-arm on screen measurements
Fluoroscan InSight mini C-arm onscreen measurements
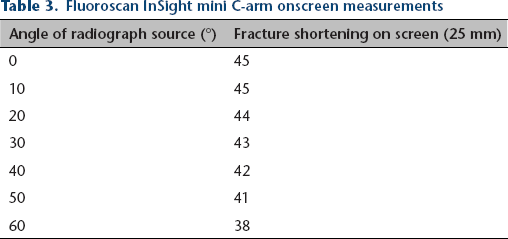
The degree of angulation demonstrated a linear relationship to the measured shortening using the OEC 9900 Elite GE C-arm and the Fluoroscan InSight mini C-arm (Figs 2 and 3). The shortening measured on the OEC 9900 Elite GE C-arm varies 2 mm with each 10° change in femur angulation. The Fluoroscan InSight mini C-arm demonstrated a variation of 1.1 mm with each 10° change in femur angulation.
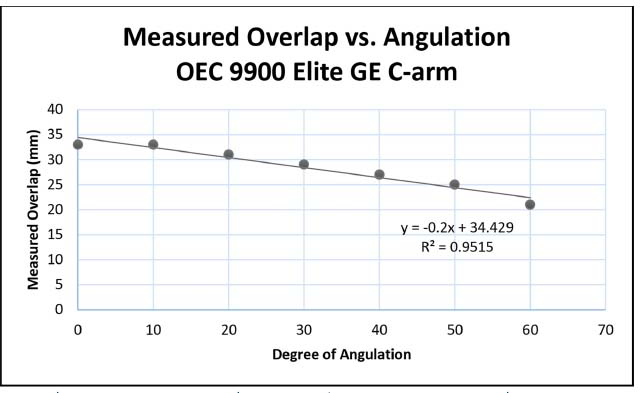
Measurement of shortening versus increasing degree of angulation to x-ray source using the GE C-arm.
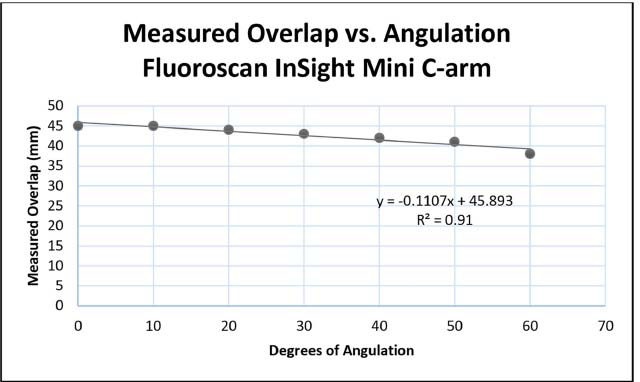
Measurement of shortening versus increasing degree of angulation to x-ray source using the mini C-arm.
Discussion
Femoral shaft fractures are a common injury in the paediatric population. Anteroposterior and lateral plain films of the femur, including the hip and knee joints, are used in the workup of a paediatric femur fracture. 5 The lateral view is essential in determining initial shortening and fracture overlap.10,11 In most cases, the individual aligning the x-ray beam and receiver is better able to achieve a perpendicular alignment on a lateral view. In 1983, using a simple diagram, Rang 10 suggested that accurate measurement of paediatric femur fracture shortening can be influenced by magnification, angulation and elevation. The concept of parallax and apparent changes in the length and position of fractures and surgical implants on a radiographic image have since been studied. Kummer and Grant 12 showed that measurement errors during tibia pin insertions are compounded not only by the alignment of the x-ray beam, but also the inherent magnification of the C-arm. In the current study, our aim was to investigate how the magnification of the C-arm, elevation of the femur on the receiver and angulation of the x-ray beam impacts the accuracy of fluoroscopic images when measuring 25 mm of shortening in a femoral fracture sawbone model.
The measurement of fracture shortening based on radiographic images is a key factor that guides treatment decisions and evaluation of fracture alignment and overlap while in the cast. Although the exact amount of shortening considered unacceptable is controversial, fractures with < 25 mm of shortening in patients up to six years of age are often considered acceptably aligned when treated with a spica cast.5–9 Fractures with shortening of > 25 mm are more commonly treated with plating, traction or external fixation. 5 As such, accurate measurement of fracture shortening is crucial to decide on the appropriate management strategy for a paediatric patient with a femur fracture. We recognise that a 25 mm fracture overlap is not a rigid scientific principle but it served as an acceptable guide for our study. In clinical practice, the patient's age, weight, mechanism of injury, the fracture pattern and the amount of shortening all influence treatment decisions. 6
The fracture site itself is not imaged directly on the image intensifier. Varying amounts of cast material, skin, muscle and fat influence the distance from image intensifier to fracture. In our study, the sawbone model was elevated above the C-arm image intensifier to account for this. As demonstrated, image size can increase by as much as 17% when the fracture is elevated 8 cm above the C-arm receiver.
Magnification is inherent in radiograph images due to the diversion of the x-ray beams. To account for this inherent magnification Rosenstein recommended that the magnification for a specific imaging system be quantified. 13 In the current study, magnification of two C-arm machines was calculated. When controlling for magnification, a C-arm image perpendicular to the fractured femur was most accurate. This principle of perpendicular images is supported by Blane et al, 14 who demonstrated that perpendicular images of the fracture during Ilizarov limb lengthening cases in the paediatric population were the most accurate method to measure the distraction gap.
In the current study, we report variation of 2 mm with every 10° angulation from perpendicular. In addition, magnification is increased an additional 1.7 × based on the elevation of the fracture site above the C-arm plate. The compounding variables of elevation and beam angulation contribute to inaccurately increased measurement of fracture shortening. This apparent increase in the measurement of fracture shortening could lead a surgeon to abandon spica casting in favour of surgical treatment. All inaccuracies were measurements of over-magnification and none of reduction.
Based on the results in this study, C-arm images are potentially inaccurate for measuring 25 mm of shortening in a paediatric femur fracture. To our knowledge, there are no commercially available C-arm machines that account for these errors. Therefore, the orthopaedic surgeon needs to evaluate and account for inherent magnification in the C-arm devices available at their practice as well as the elevation and angulation of the affected limb off the receiver. In the current study, we used a metal coin to assess these parameters. Alternatively, a metal sphere of know diameter placed at the level of the bone can also be used as done in pre-operative templating during total hip and knee arthroplasty. 15 These parameters affect the accuracy of the image when measuring femur fracture shortening.
In conclusion, as previously noted by Rang, 10 radiographs can be misleading when measuring paediatric femoral fracture shortening. The current study demonstrates that each C-arm machine has a unique amount of magnification and this magnification should be measured and accounted for at the time of treatment. Additionally, elevation of the fractured bone off the image intensifier and the angulation of the limb relative to the C-arm can also affect accurate measurement of fracture shortening. Lastly, we recommend that the image should be taken with the source perpendicular to the facture site.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Ethical approval: No funding was received for this study. This article does not contain any studies with human participants or animals performed by any of the authors. Informed Consent: Not required.