
Abstract
Purpose
Spinal deformity in neurofibromatosis, when associated with dystrophic change, is a major treatment challenge. Early anterior and posterior spinal fusion is the accepted treatment plan for severe progressive kyphoscoliosis. Resection of the vertebral body as an additional step in correction and fusion has not been previously investigated. Information on the functional status of the neurofibromatous curves is also scarce in the literature. The purpose of this study is to report an experience with corpectomy and circumferential fusion in dystrophic spines of neurofibromatosis.
Methods
Among 16 patients with dystrophic spinal curves, nine cases who had undergone anterior and posterior fusion with 6.7 years (range 2–11.9) average follow-up were evaluated clinically, radiographically, and functionally (SRS-22).
Results
Nine cases with a mean age of 11.8 years (range 7.8–17) at surgery consisted of seven kyphoscoliotic patients, who had received one or two levels of cord decompression and corpectomy, and two cases of scoliosis with hypokyphosis. Surgery improved the mean preoperative scoliosis of 87 (range 60–110) and local kyphosis of 69.3° (range 50–100) to 49 (range 15–85) and 49° (range 35–70), respectively. Loss of correction of 5° in the scoliosis and 13° in the kyphosis angles was observed in the final follow-up. One surgery resulted in an immediate postoperative mortality. Fusion was achieved in all cases. The average SRS-22 score of 4.1 (range 3–4.6) was obtained.
Conclusions
Simultaneous anterior and posterior fusion with corpectomy for dystrophic neurofibromatous spinal deformities is associated with a high fusion rate, good correction, and also good functional outcome.
Introduction
Spinal deformity is the most common musculoskeletal manifestation of neurofibromatosis, affecting 10–30% of cases [1–4]. It is grouped into dystrophic and non-dystrophic curves [2, 5, 6]. Non-dystrophic curves, which may modulate to dystrophic ones, have a more benign course and behave like idiopathic scoliosis [4, 7]. The dystrophic group, with their sharp-angulated, short-segment, and often kyphoscoliotic deformities, are usually rapidly progressive and do not respond to conservative treatment [2, 3]. Surgery in hyperkyphotic dystrophic curves—especially with only posterior operation—has been, traditionally, associated with high complication rates of pseudoarthrosis and paraplegia [2, 6, 8]. Early anterior and posterior spinal fusion with meticulous bone grafting has, however, decreased the pseudoarthrosis rate [8].
Instrumentation is often difficult, since the subjects are small children with very soft bones, distorted anatomy, and severe deformities, and, sometimes, the presence of neural tumors in and around the cord or nerve roots [2].
Anterior decompression of the cord in the apex of sharp kyphosis is often necessary for the already present neurologic compromise or in cases with expanding tumors or significant angulations [2, 9]. Removal of the vertebral body at the apical level makes the correction of deformity easier, and may facilitate decompression of the cord [10]. There is very scant literature on this section of treatment for dystrophic curves [11, 12]. We would like to report our results for anterior decompression with corpectomy, along with anterior and posterior fusion and limited instrumentation, and also provide a functional assessment in a small homogenous group of patients.
Materials and methods
This is a case series study of patients with neurofibromatosis, who had been treated for their spinal deformities secondary to neurofibromatosis in Nemazee hospital, the main teaching hospital of Shiraz Medical University.
The medical records of all cases who met the criteria for neurofibromatosis [13], and had been referred to the senior author (G.H.S.), were collected. Among the patients who had been referred to our center for neurofibromatous spinal deformity, over a 20-year period, 16 cases had dystrophic-type curves. They were all considered for surgical intervention. These patients had evidence of progression and high magnitude of curves at the time of presentation to our center. They were all surgical candidates. In fact, as a result of delayed referrals, non-surgical treatment could no longer be considered an option.
As a result, 11 patients have already had their spinal surgery, three more recent cases are on the waiting list for surgery, and two cases have refrained from surgery. One patient with good correction and in a stable condition had a short follow-up of only 1 year, and was not included in the series. One case expired in the recovery room in the immediate postoperative period and, therefore, could not have functional or long-term follow-up reports, but is included in the complication list. All of the cases had received preoperative pulmonary function assessment by a pulmonologist. Magnetic resonance imaging (MRI) evaluation of the spine with special attention to possible dural ectasia, intra-dural tumors, etc., had been performed for each patient. Flexibility of the curves was assessed by side bending and traction antero-posterior radiographs, as well as lateral, flexion/extension views. No case was considered for halo-femoral traction.
The surgical technique consisted of thoracotomy or thoraco-abdominal exposure in the decubitus position, entering from the convex side. The discs and end-plates were excised in all of the involved levels, with an attempt to preserve segmental vessels as much as possible. The spinal canal at the apex of the kyphotic deformity was always found to be very narrow with a flattened cord, so that even a tiny neural probe or very narrow feeding tube could not be passed through. Bulbous nerve roots were often seen at or close to the area of corpectomy, at the start of their exits from the foramina. The findings, however, were not uniform.
Anterior cord decompression at the apex of the kyphotic deformity and at least one level above and one level below the apex was performed in all cases of kyphoscoliosis. Corpectomy in one or two levels at the sagittal apex was also performed. Strut grafting of the anterior bodies with single or double non-vascularized rib grafts were done. The patients would be then transferred to the prone position and posterolateral fusion of all the deformed levels, with the addition of the Harrington distraction system, spanning the whole primary scoliotic vertebrae, was performed. The rod was mainly used as an internal splint and no attempt was made to achieve correction with that distraction system. The addition of a few inter-spinous wires to secure the rod placement or sublaminar wire in one or two levels (away from the apex and where no intra-dural tumor was suspected) were all supplementary for fixation and not for correction of the deformity. Pediatric segmental fixation devices were not available at the time in our center for the majority of these cases. Autogenous rib and iliac crest bone grafting supplemented the posterior fusion. No somatosensory evoked potential test or neurosensory monitoring was available, but a wake-up test was performed on all of the cases. All of the patients had early postoperative ambulation with thoraco-lumbosacral orthosis. The use of orthosis continued for about 2 years, because fixation was not segmental and the internal support in the soft bone of growing children needed additional external support.
For this study, all nine cases were called in for clinical and radiographic evaluation. They also filled out the Scoliosis Research Society-22 patient questionnaire, which consisted of 22 questions encompassing five areas of pain, self-image, function, mental health, and satisfaction status of the treated patients [14]. All cases were examined thoroughly with a detailed neurologic evaluation for their spinal problems. Supine and standing antero-posterior radiographs, stress-bending films, and, in some cases, computerized tomographies (CT) were obtained. We looked, in detail, for bridging bony trabeculae, any motion at the fused levels, and any evidence for a change in orientation or shape or location of instruments. The pre- and postoperative and all follow-up radiographs were assessed meticulously for their curve magnitude, dystrophic changes, correction gained postsurgery, maintenance or loss of correction, and signs of fusion. We are, therefore, reporting the experience in a time frame of about 12 years with dystrophic neurofibromatous spinal deformity surgery, which consisted of corpectomy, anterior cord decompression, circumferential spinal fusion, and posterior instrumentation. Ten consecutive cases with a mean follow-up of 6.7 years (range 2–11.9) had the above procedure. With one early death, nine cases have had sufficient clinical, radiographic, and functional assessment to be reported. The statistical analysis was by a non-parametric Pearson correlation test.
Results
The nine cases of dystrophic spinal deformities, consisting of four girls and five boys, had an average age of 11.8 years (range 7.8–17, median 11) at surgery and 18.5 years (range 9.8–24, median 17.4) at follow-up. They consisted of seven kyphoscoliosis and two scoliosis cases with thoracic hypokyphosis. None of the cases had received any treatment for their deformities prior to referral to our center. The apices were all thoracic, varying from T6 to T11, and the curves included 3–5 bodies.
The average preoperative scoliosis Cobb angle was 87° (range 55–110, median 100) and kyphosis (in seven cases) was 69.3° (range 50–100, median 70). Two cases of thoracic hypokyphosis had 0° and 25° sagittal Cobb angles (Table 1).
Detailed characteristics of the nine neurofibromatous spines
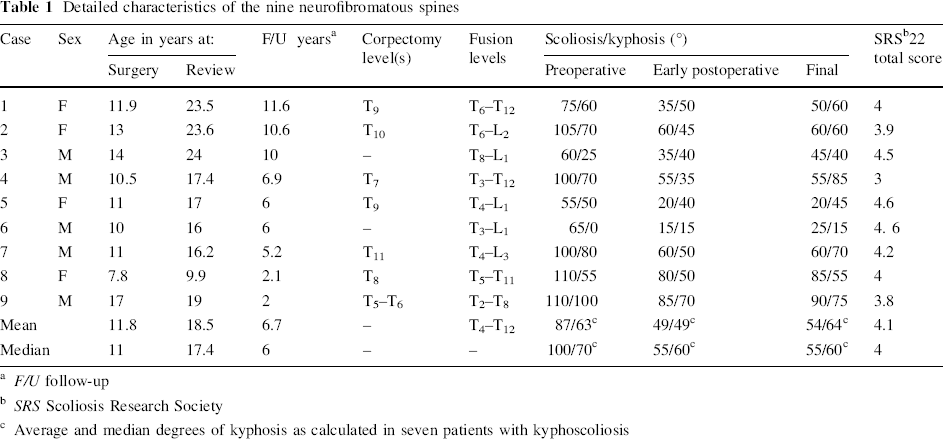
F/U follow-up
SRS Scoliosis Research Society
Average and median degrees of kyphosis as calculated in seven patients with kyphoscoliosis
From the six radiographic and clinical signs of curve dystrophy (rib penciling, vertebral body scalloping, transverse process spindling, foraminal enlargement, severe apical rotation, and adjacent soft tissue neurofibroma), four signs were observable in all nine patients (Table 2).
Distribution of signs of dystrophy
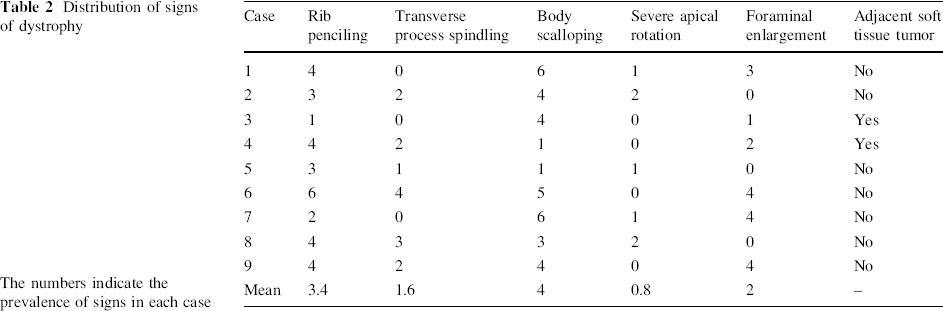
The numbers indicate the prevalence of signs in each case
Plexiform neurofibromatous skin lesions at the site of spinal curvature in two patients (cases 4 and 9) (Fig. 1) and macrodactyly in the foot of one patient (case 5) were the associated neurofibromatosis findings. At the time, no case had an MRI-proven brain tumor, long-bone pseudoarthrosis, hemihypertrophy, seizure disorder, or hypertension. Five of these cases had neurofibromatosis in first-degree relatives and four others seemed to be new mutations. All of the cases were neurologically normal before surgery and had moderate pulmonary function compromise. The pressure effect on the cord by the severe kyphosis was evident on MRI signals in all of the apices. No rib protrusion, cord tumor, or cyst was present. Bulbous roots in and around the apical levels were recognized in six cases.

Plexiform neurofibroma at the site of surgery
The average levels of anterior release and fusion was 5.8 (range 4–8) and 8.8 (range 6–12) levels for posterior fusion. The average surgical time was 5 h (range 4–8). The main surgical complication was the death of one patient. In those nine cases with follow-ups, however, one patient (case 9) had the more significant complication. This case, with 100° kyphosis and 110° scoliosis, could not be weaned off the respirator until the fifth day postsurgery. One patient (case 3) developed a lumbar (L5 root) schwannoma presenting as leg pain 6 years after his spine fusion. This was removed without any side effect and did not effect his fusion surgery.
There were no neurological or wound complications. (The one individual who died in the recovery room and is not included in the final follow-up of this series was a 16-year-old girl with scoliosis/kyphosis of 75°/70°. She was awake and neurologically intact following surgery in the postanesthetic room for about 1 h. She then developed sudden cardiorespiratory arrest apparently from a transfusion reaction to a newly hanged blood. The patient was not revivable and no autopsy was allowed by the parents.) Intraoperative blood loss of 20–25% of the total blood volume (including the one mortality case) was observed, mainly during the anterior approach. Blood transfusion was done in the latter part of the procedure in all cases.
Radiographic assessment for fusion was performed regularly every 6 months. The final follow-up evaluation was performed 6.7 years (range 2–11.6 years) postsurgery. Final correction, in the fused levels, of 30% for the localized kyphosis and 45.2% for scoliosis was observed (Fig. 2).

Pre- and postoperative films of a case of kyphoscoliosis.
There were two cases with 0° and 25° curves at the dystrophic segments on lateral views that had become 15° and 40°, respectively. Comparing the initial and the final radiographs, the mean loss of correction was 5° in the frontal plane and 13° in the sagittal plane. The change in degree of scoliosis was minimal and usually stabilized within 1 year postsurgery. Only three cases had loss of local kyphosis correction of 13° at the apex of kyphosis and not above or below the instrumentation level. These three, however, stabilized by 2.5 years and remained unchanged in 3-, 4.5-, and 8-year follow-ups. The scoliosis, however, did not change in these three patients.
Secondary curves above and below fusion levels were not seen in follow-up radiographs. In general, the higher the initial kyphosis, the higher the degree of correction loss (P-value = 0.036, correlation coefficient [CC] = +0.7). The age of the patient at the time of surgery or duration of follow-up had no relation with correction loss.
The more detailed evaluation of fusion status (no implant failure, no change in number of ‘notches’ of the Harrington rod above or below the upper hook, visible fusion mass with bridging trabeculae on radiographs, or CT scan) was confirmed in all nine cases. One patient (case 4) whose 70° local kyphosis at age 10.5 years had improved to 35° postsurgery, but decreased his correction to 85° by age 13 years and has stayed at that level to his present age of 17.4 years. The CT reconstruction views show no evidence of pseudoarthrosis. This seems to have been a plastic deformation just above the apex, but still in the instrumented level. This patient had a plexiform neurofibroma at the apex of his deformity, through which posterior surgery had to be done. Interestingly, the second case (case 9), who had a huge cutaneous plexiform neurofibroma at the apex, did not have any change in his deformity correction with the passage of time.
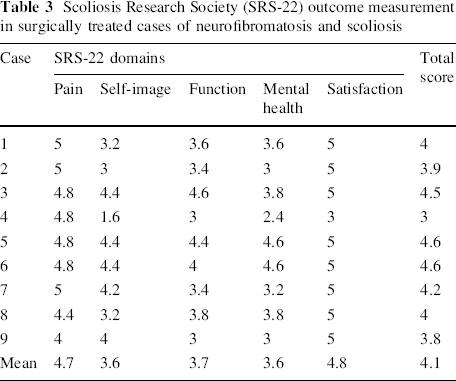
The SRS-22 outcome instrument showed a mean total score of 4.1 (the maximum score being 5). The mean scores for each of the five domains were above 3.5 (Table 3). Both preoperative and final measurements of the kyphosis angle had reverse correlation with the total SRS-22 scores (P = 0.02, CC = −0.75 and P = 0.003, CC = −0.86). In terms of scoliosis, the preoperative and final degrees had a reverse correlation with the SRS-22 total scores (P = 0.02, CC = −0.75 and P = 0.03, CC = −0.73). The relation of each domain with curve magnitude was also assessed. Although with this small number of cases a meaningful conclusion is hard to ascertain, the self-image section of SRS-22 had a more clearer correlation with the final kyphosis (P = 0.03, CC = −0.71). Case 4 with the highest degree of kyphosis correction loss had low scores in each domain and this seemed to affect the total mean score as well. The satisfaction scores were 5 in all patients except for case 4 (Table 3).
Scoliosis Research Society (SRS-22) outcome measurement in surgically treated cases of neurofibromatosis and scoliosis
Discussion
The number of neurofibromatous spinal deformities requiring surgery is few. There is no report in the recent literature of any large series on this subject. Winter et al. [2] reported on 102 patients with 80 dystrophic curves in 1979. The 1999 paper by an Italian group [8] on 56 patients was, in fact, an updated report of the original 1983 paper. Crawford states that only 3% of patients in a regular scoliosis clinic would have neurofibromatosis [9]. The number of dystrophic patients would be even less [1]. This might be the reason why the personal experience of any single spine surgeon with such an entity would not be extensive and why there are not very many articles on this subject in the literature.
The need for early fusion for dystrophic neurofibromatous spinal deformity is now a well established and widely accepted fact [2, 3, 5, 6, 8]. The malignant behavior of such sharp and short angulated curves may result in major cosmetic, cardiopulmonary, and spinal cord problems [2, 3, 15].
The pseudoarthrosis rate has been high, so that for doubtful cases, surgical re-exploration and repeated bone grafting in 6 months has been advocated [2, 9].
This manuscript is only a small but personal experience with such a challenging spinal condition. We had late referral of cases and it was determined during their first visits that they were all surgical candidates. The sharp angulations usually produced a frightening pressure effect at the apex, revealed by the MRI studies of the cord. With the usual rapid progressive course, eventual cord compromise seemed prudent. That was one reason for why, even without neurologic deficit, all hyperkyphotic cases were considered for anterior cord decompression.
Malaligned apical vertebrae with severe rotation would make effective anterior release and strut grafting difficult, and probably technically inadequate [5, 8]. Corpectomy of the thoracic apical vertebrae, which are usually out of the support axis and are squeezed against each other in a complex three-dimensional pattern, provides better cord decompression, removes a major part of deformity, and produces some mobility for the correction of kyphosis with the strut bone graft [8, 10, 16]. A strong anterior strut graft could probably help with the maintenance of any obtained correction. The bone in the remaining bodies is often very soft and a strong fibular graft could potentially perforate into the canal. To avoid the morbidity of another graft site, we recommend using a rib strut graft. The very soft ribs can be doubled or tripled before insertion for added strength, if the small space allows such a thickness.
Extensive bleeding is a major concern in treating dystrophic high-grade deformities. In the soft vertebral bodies, during piece-meal corpectomy, frequent stops and compression of bleeding surfaces is necessary. Hasty insertion of strut grafts can perforate epidural veins, contributing to more bleeding. Therefore, meticulous attention to details of slow corpectomy, hemodynamic stability, and then a well-placed graft could prevent complications. The segmental vessels are best to be preserved as much as possible. Only the vessels at the corpectomy level need to be ligated to avoid compromise of Adamkiewicz’ artery and potential cord circulation problems. This precaution has proved effective in the cases reported here.
There is only scant literature on thoracic corpectomy for kyphoscoliosis [10]. It becomes indicated, at times, for burst fractures, tumor resection, and infection or in congenital scoliosis and very rigid major deformities [10]. In neurofibromatosis, only a couple of reports referring to such a procedure are present [11, 12].
Winter et al. [2] reported 64% pseudoarthrosis in posterior fusion alone in patients with kyphoscoliosis. The same author reported pseudoarthrosis in 2 out of 8 cases of planned anterior and posterior fusion [2]. Crawford et al. [9] reported 13% pseudoarthrosis in the posterior fusion of 46 dystrophic and non-dystrophic neurofibromatous curves. He also mentioned five cases of pseudoarthrosis after multiple surgical procedures for eight patients with dystrophic curves that had more kyphosis than scoliosis. Sirois and Drennan reported 38% pseudoarthrosis in 23 dystrophic curves undergoing isolated posterior fusion [17].
Parisini et al. [8] achieved 47% fusion with the posterior approach, with 7 of their 11 kyphoscoliotics ending up with pseudoarthrosis. When they combined anterior and posterior techniques, the fusion rate was 77% for dystrophic curves and 4 out of 20 kyphoscoliosis cases resulted in pseudoarthrosis.
In the five cases of kyphoscoliosis in the series of patients reported from Hong Kong, one developed persistent pseudoarthrosis with circumferential fusion (even with repeated bone grafting) and the other four patients had progression of kyphoscoliosis [5]. A later report of 27 cases by Winter et al. with a more aggressive surgical approach to dystrophic curves with a high degree of kyphosis resulted in fusion in all [15]. The more recent reports from Hungary and China have had 1 case out of 11 and 3 out of 39 dystrophic curves with pseudoarthrosis [18, 19].
In the current study, maintenance of achieved correction and the degree of progression in the frontal and sagittal planes were different. An average of 5° loss of scoliosis correction was observed, while the sagittal correction loss was 13°. These findings as reported by Calvert et al. [3] were 7° for both scoliosis and kyphosis in 12 stable fusions out of 15 cases of posterior spinal fusion and Harrington instrumentation. The other three cases developed pseudoarthrosis and progressive deformity. Shen et al. [18] from China reported 5° frontal plane and 4° sagittal plane correction loss in thoracic curves. Sirois and Drennan, however, reported an average curve progression of 12.7° in 23 dystrophic curves after isolated posterior fusion [17].
Loss of some correction of kyphosis, significant in three cases in the present series, does not always herald pseudoarthrosis. Among 19 dystrophic scoliotic patients treated by posteriorly instrumented fusion by Parisini et al. [8], ten cases achieved stabilization and lost 10° of their correction at final follow-up. Three of the remaining nine patients had a second exploration, and in one of these cases, despite significant curve progression, no definite pseudoarthrosis was found. The authors explained plastic deformation of fusion mass as the cause of progression. This point has been also implied by Betz et al. [6]. The instrumentation in neurofibromatous curves is not easy, especially in children, due to small vertebrae, osteoporotic bone, and tumors in and around the cord [2, 16]. As a result, we did not plan for major surgical correction; segmental instrumentation with excessive crowding of the bony spinal canal seemed to increase the risk of cord or root injury [8]. Even in the anterior strut grafting, we suggest caution against attempting a major correction with the use of a long or very rigid strut. A major force in obtaining correction can stretch not only the anterior vascular structures, but also the cord. It is realized that more secure present-day segmental fixators may provide more stability and would possibly avoid significant loss of initial correction. There is, however, -concern for the holding power of small osteoporotic spinal elements in these patients, and also the common bulbous neurofibromatous roots that compromise the available space. Multiple-segment instrumentation, although producing higher correction, could also contribute to increased pseudoarthrosis risk. The rod used in this series was only a holding device and was not intended for distraction. The authors believe that a less rigid fixation may facilitate a better fusion, as demonstrated in the present paper. We believe in the long duration of postoperative brace immobilization and early ambulation as pointed out by Winter et al., as well as Crawford et al. [2, 16]. Betz et al. [6] used to keep the patients in bed rest for 6 months.
We, however, managed to obtain 46% correction in scoliosis and 30% in kyphosis. The claimed correction was 33% in scoliosis and 32% in kyphosis in cases with round (not angular) kyphoscoliosis, but was much lower in angular kyphoscoliotics in series reported by Hsu et al. [5]. Shen et al. [18], however, reported 49% coronal and 48% sagittal correction obtained in dystrophic thoracic curves. Parisini et al. [8] obtained 14.5% correction in scoliotics alone, while in kyphoscoliotic cases, 22.5% frontal plane and 33.4% sagittal plane correction were achieved. They considered the stoppage of progression as a good result, despite only modest correction.
A structured outcome assessment in dystrophic spinal deformities has not been reported previously, and only mentions of daily activities or ambulatory status have been made in the literature [6, 19]. SRS outcome instruments [20], including SRS-22 [14], are designed for idiopathic scoliosis, but can be used as a condition-specific instrument for the postoperative evaluation of non-idiopathic spinal curves or even other spinal conditions [21, 22]. The present paper found a generally high postoperative score (4.1) in SRS-22 functional assessment in neurofibromatosis. Finally, kyphotic deformity had a more significant correlation with the obtained score.
The small number of cases is the main limitation of this study; being only a personal experience is another shortcoming of this paper. The fact, however, remains that dystrophic neurofibromatous spine deformities are relatively rare and not very many orthopedic surgeons have long-term experience with its multi-faceted problems. Corpectomy with circumferential fusion along with a less rigid ‘internal splint’ can be another armamentarium in the hands of a spinal surgeon in managing such complex problems. It produces high fusion rate, good correction, and also a good functional outcome.