
Abstract
Abstract
Purpose
The erythrocyte sedimentation rate (ESR) and white blood cell (WBC) count are frequently obtained in the work-up of post-operative fever. However, their diagnostic utility depends upon comparison with normative peri-operative trends which have not yet been described. The purpose of this study is to define a range of erythrocyte sedimentation rates and white blood cell counts following spinal instrumentation and fusion in non-infected patients.
Methods
Seventy-five patients underwent spinal instrumentation and fusion. The erythrocyte sedimentation rate and white blood cell count were recorded pre-operatively, at 3 and 7 days post-operatively, and at 1 and 3 months post-operatively.
Results
Both erythrocyte sedimentation rate and white blood cell count trends demonstrated an early peak, followed by a gradual return to normal. Peak erythrocyte sedimentation rates occurred within the first week post-operatively in 98% of patients. Peak white blood cell counts occurred with the first week in 85% of patients. In the absence of infection, the erythrocyte sedimentation rate was abnormally elevated in 78% of patients at 1 month and in 53% of patients at 3 months post-operatively. The white blood cell count was abnormally elevated in only 6% of patients at 1 month post-operatively. Longer surgical time was associated with elevated white cell count at 1 week post-operatively. The fusion of more vertebral levels had a negative relationship with elevated erythrocyte sedimentation rate at 1 week post-operatively. The anterior surgical approach was associated with significantly lower erythrocyte sedimentation rate at 1 month post-operatively and with lower white cell count at 1 week post-operatively.
Conclusion
In non-infected spinal fusion surgeries, erythrocyte sedimentation rates are in the abnormal range in 78% of patients at 1 month and in 53% of patients at 3 months post-operatively, suggesting that the erythrocyte sedimentation rate is of limited diagnostic value in the early post-operative period.
Introduction
Surgical site infections (SSIs) following instrumented spinal fusion are an infrequent but potentially devastating complication, reported to occur in 0.9–8.3% of fusions [1–8]. Deep wound infection represents the most frequent complication of scoliosis surgery requiring reoperation [9]. The presence of instrumentation within the fusion bed creates an environment that fosters bacterial growth through glycocalyx formation and further increases the risk of SSI [10].
SSIs after spinal instrumentation and fusion can have a non-specific presentation and be difficult to definitively diagnose. SSIs are most commonly characterized by the presence of non-specific symptoms, including pain, a fluctuant peri-incisional area, and wound drainage [2, 6]. This non-specific presentation and the absence of diagnostic laboratory tests to differentiate SSIs from other causes of pain, fever, or implant failure can delay the diagnosis of SSI.
There are no known reliable laboratory parameters to diagnose or predict infection after spinal fusion. Inflammatory markers including the white blood cell (WBC) count and erythrocyte sedimentation rate (ESR) are often employed as diagnostic tools in orthopedics. These laboratory parameters have successfully been utilized in the diagnosis of septic arthritis in children [11], infected total joint arthroplasty [12–17], and pediatric acute hematogenous osteomyelitis [18–20]. Because of this, the ESR and WBC count are frequently obtained in the work-up of early post-operative fever following spine instrumentation and fusion. However, normative peri-operative trends of these parameters remain to be described following pediatric spinal deformity surgery. The utility of inflammatory parameters as diagnostic entities in the early peri-operative period depends on the knowledge of normative trends.
The objectives of our study were to define the normative range of the ESR and WBC count following spinal instrumentation and fusion in non-infected pediatric patients, to characterize the trends of these parameters in this period, and to determine whether or not operative or demographic parameters are correlated with increased ESR or WBC count in the early post-operative period.
Materials and methods
The study cohort consisted of 75 primary spinal fusions performed at one of our tertiary-care pediatric hospitals between April 1994 and January 1997. Surgery was performed by three different staff orthopedic surgeons. The WBC count and ESR were checked pre-operatively, at 3 and 7 days post-operatively, and at 1 and 3 months post-operatively. Diagnosis, age of the patient, duration of anesthesia and surgery, surgical approach, estimated intraoperative blood loss, and the number of vertebral levels fused were all recorded. A note was made of any patients who returned to the operating room for any complication or for any signs or symptoms consistent with infection, including post-operative wound drainage or dehiscence, back pain, fevers, or chills. Infection was defined by the presence of positive intraoperative cultures taken at the time of removal of instrumentation or, if cultures were negative, a clinical presentation consistent with infection.
All patients received pre-operative cefazolin (or vancomycin, in case of penicillin allergy) at an appropriate weight-based dose 30 min prior to incision. In all patients, antibiotic therapy was continued until the deep and superficial hemovac drains were discontinued, on post-operative days 3 or 4. All patients had a pre-operative urinalysis which was negative for infection. No patients had post-operative courses complicated by other infections (i.e., pneumonia, urinary tract infections, etc.).
For analysis, SPSS (SPSS Inc., Chicago, IL) was used to determine whether or not specific operative or demographic factors correlated with the ESR and WBC counts in the post-operative period. Pearson's correlation coefficient was used to analyze the surgical time, estimated blood loss, and number of vertebral levels fused. One-way analysis of variance (ANOVA) was completed in order to analyze the relationship between the surgical approach and diagnosis. Significance was established at a p-value < 0.05.
Results
Seventy-five patients (50 female and 25 male) were included in the study. Diagnoses included idiopathic scoliosis (n = 56, 74.6%), congenital scoliosis (n = 14, 18.6%), and neuromuscular scoliosis (n = 5, 6.6%). The mean age of the patients at the time of surgery was 14.6 ± 2.42 years (range 4.9–19.6 years). Patients were followed for a mean of 5.3 ± 2.58 years post-operatively. The mean duration of surgery was 7 h, 5 min (range 2 h, 35 min–12 h, 40 min). The mean estimated blood loss was 898 ± 620 mL (range 200–3,970 mL). Forty patients (53.3%) received intraoperative salvage of autologous blood with the use of cell saver and/or infusion of pre-operatively donated autologous blood. Fifteen patients (20%) received both pre-operatively donated autologous blood and salvaged blood intraoperatively. One patient received banked blood transfusion alone.
In 38 patients (51%), a posterior surgical approach was utilized and in 21 patients (28%), an anterior approach was used. A total of 16 patients (21%) underwent a circumferential fusion; of these, 14 patients underwent a combined anterior–posterior approach on the same day, while two patients underwent both anterior and posterior fusions in a staged manner. A mean of 11 ± 3.34 vertebral levels (range 3–17) were included in the arthrodesis.
Six patients (8%) had a subsequent operative procedure: three for the removal of prominent instrumentation and one each for re-instrumentation and fusion after curve progression, pseudarthrosis, and deep wound infection. Intraoperative cultures were taken in all cases of return to the operating room. All secondary surgeries occurred at least 3 months after the primary surgery.
Only non-infected patients were included in the analysis. The single patient which was excluded was a 17-year-old male with adolescent idiopathic scoliosis that underwent a posterior spinal instrumentation and fusion from T2-L3. At 4 years post-operatively, he was diagnosed with a deep implant infection by Staphylococcus epidermidis and Propionibacterium acnes. He underwent a single irrigation and debridement procedure with retention of his implants and the administration of intravenous and oral antibiotics. At the last follow-up at 20 months after the irrigation and debridement, he was asymptomatic. At the index fusion surgery, the total length of anesthesia was 455 min, the length of surgery was 385 min, and the intraoperative blood loss was 1,200 cc.
At our pediatric hospital, the normal range of ESR is defined as 0–10 mm/h. The mean ESR pre-operatively was 8 ± 7 mm/h (range 0–32 mm/h). At 3 and 7 days post-operatively, the mean ESRs were 72 ± 21 and 70 ± 24 mm/h, respectively (ranges 7–120 mm/h and 10–115 mm/h, respectively). One month after surgery, the mean ESR was 22 ± 13 mm/h (range 0–57 mm/h). Three months post-operatively, the mean ESR was 13 ± 8 mm/h (range 4–40 mm/h). There was no significant difference between the ESR in patients with idiopathic, congenital, or neuromuscular scoliosis at any of the recorded time points (pre-operative p = 0.912, 3 days p = 0.0699, 7 days p = 0.181, and 1 month p = 0.166). Figure 1 demonstrates the trend of the mean ESR in the first 3 months post-operatively for non-infected patients.
Peri-operative ESRs demonstrate an early peak followed by a slow decline toward normal in all patients, regardless of surgical approach
In 40 patients (54%), the peak ESR occurred at 3 days post-operatively. In 32 patients (43%), the peak ESR occurred at post-operative day 7. One patient had equivalent peak ESRs at post-operative days 3 and 7 and, for unclear reasons, one patient had a peak ESR at 1 month post-operatively. In 18 of 74 patients (24%), the ESR was abnormally elevated prior to surgery. At 3 days post-operatively, 66 of 68 patients (97%) had an elevated ESR. Similarly, at 7 days post-operatively, 67 of 69 patients (97%) had an abnormally elevated ESR. At 1 and 3 months post-operatively, 56 of 72 (78%) and 21 of 40 patients (52%) continued to have abnormally elevated ESRs. Figure 2 demonstrates the relative percentage of patients who had an abnormally elevated ESR at the various post-operative time points.
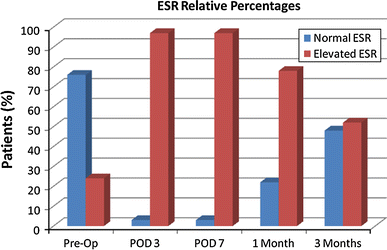
The relative percentages of patients with abnormally elevated ESR in the peri-operative period
At our institution, the normal range of WBC count is defined as 3.8–9.8 × 109/l. The mean WBC count pre-operatively was 6.3 ± 1.8 × 109/l (range 3.5–11.7 × 109/l). At 3 days post-operatively, the mean WBC count was 9.1 ± 2.20 × 109/l (range 5.2–14.3 × 109/l). At 7 days post-operatively, the mean WBC count was 7.3 ± 2.58 × 109/l (range 3.6–19.8 × 109/l). At 1 month post-operatively, the mean WBC count was 6.8 ± 1.67 × 109/l (range 3.5–11.6 × 109/l). There was no significant difference between the WBC count of patients with idiopathic, congenital, or neuromuscular scoliosis at any of the recorded time points (pre-operative p = 0.282, 3 days p = 0.850, 7 days p = 0.821, and 1 month p = 0.157). Figure 3 demonstrates the trend of WBC counts in the first month after surgery for all non-infected patients.
Peri-operative WBC counts demonstrate a rapid increase in value followed by a slow decline toward normal
The one patient with a deep wound infection had the following ESR values: pre-operative, 7; 3 days post-operative, 90; 7 days post-operative, 35; and 1 month post-operative, 6.0. The WBC counts were: pre-operative, 8.5, 3 days post-operative, 10.8; 7 days post-operative, 8.8; 1 month post-operative, 7.2. When compared to the mean values of the non-infected patients, there were no significant differences or trends identified.
Similar to the ESR, the WBC count trends were characterized by an early peak, followed by a gradual return to normal levels. Forty-eight patients (65%) had peak WBC counts at post-operative day 3. Ten patients (14%) had peak WBC counts at post-operative day 7, and 5 patients (7%) had equivalent peaks at post-operative days 3 and 7. For unclear reasons, 9 patients (12%) had peak WBC counts at 1 month post-operatively and 2 patients (3%) had peak WBC counts pre-operatively.
At the measured time points, elevated WBC counts were documented as follows: 3 of 74 patients (4%) pre-operatively, 23 of 74 (31%) patients at 3 days post-operatively, 10 of 69 patients (15%) at 7 days post-operatively, and 4 of 72 patients (6%) at 1 month post-operatively. Figure 4 demonstrates the relative percentage of patients who had an abnormally elevated WBC count at the various post-operative time points.
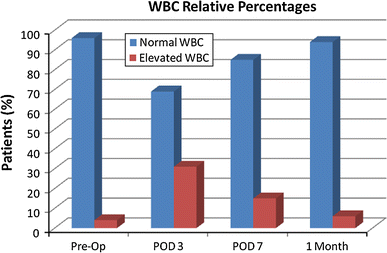
The relative percentages of patients who had an abnormally elevated WBC count at various post-operative time points
Data were analyzed to determine which specific patient or treatment factors were correlated with elevated ESRs and WBC counts in the post-operative period. The length of surgery did not correlate with the ESR at any of the recorded post-operative time points, but it did correlate weakly with elevated WBC count at 7 days post-operatively (r = 0.366, p = 0.002). Similar correlations between the WBC count and length of surgery at other time points were not identified. Neither the ESR nor WBC count were found to be correlated with the intraoperative estimated blood loss at any point during the measured post-operative period.
A weakly negative correlation was found between the number of vertebral levels fused and elevated ESR at 1 week post-operatively (r = −0.284, p = 0.025). No similar correlation was found at any of the additional measured post-operative time points. The WBC count was not found to be significantly correlated with the number of vertebral levels at any of the measured time points.
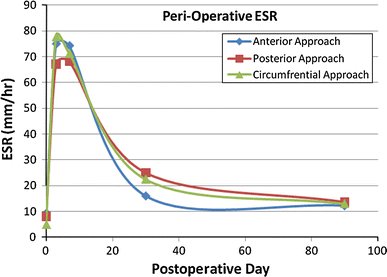
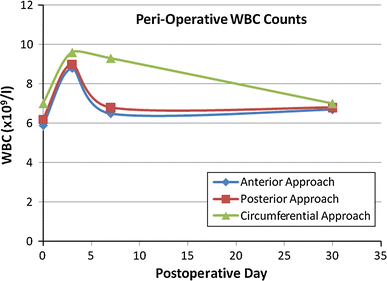
When the patient population was analyzed on the basis of surgical approach, two statistically significant differences were found. First, those patients who underwent instrumentation and fusion from an anterior approach were found to have lower ESRs at 1 month post-operatively when compared to those undergoing posterior or circumferential approaches (p = 0.038). No similar correlations were found between the ESR and approach at the other measured time points. Secondly, patients undergoing a circumferential approach were found to have significantly higher WBC counts at 1 week than those who had instrumentation and fusion through either an isolated anterior or posterior approach (p = 0.001). The WBC count was not correlated with the surgical approach at any of the other measured time points. Diagnosis did not predict WBC count or ESR trends at any of the measured time points. Figures 5 and 6, respectively, demonstrate the trend of the ESR and WBC count in the peri-operative period, with various surgical approaches being represented by individual data plots.
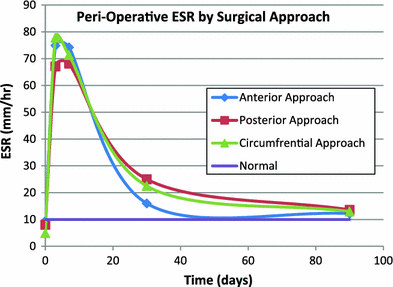
Peri-operative ESRs by surgical approach
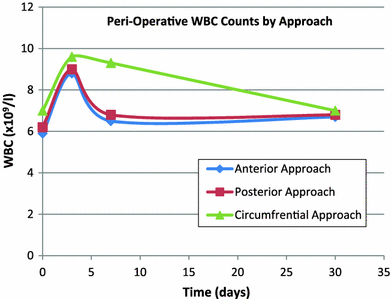
Peri-operative WBC counts by surgical approach
Discussion
SSIs represent a potentially devastating complication after the operative correction of spinal deformity. In addition to threatening patient outcomes, SSIs are estimated to double the healthcare costs for the individuals affected [21, 22]. Though its frequency remains low, SSI typically requires return to the operating room. In late-presenting infections when solid fusion is likely, infection is reliably cured with surgical implant removal, irrigation and debridement, and intravenous antibiotic therapy. Acute SSIs, however, are much more problematic. The destabilized and corrected spine has not developed a fusion mass to maintain the desired spinal alignment. Because of this, implant retention is often necessary and requires intravenous antibiotic therapy, followed by long-term oral suppressive antibiotics. Cases requiring implant removal will subsequently require reinstrumentation in order to maintain spinal correction [4]. In light of the seriousness of post-operative infection and the complexity of its treatment, physicians must maintain a high index of suspicion for SSI. In the case of post-operative spine infections, this is complicated by the non-specific presentation of infection following surgery. Signs or symptoms of infection following spinal fusion, including post-operative fever, chills, or malaise, present a diagnostic challenge to the pediatric spine surgeon, as the differential for the clinical presentation is broad.
In clinical practice, the ESR and WBC count are often obtained in an effort to elucidate whether or not infection is present. These parameters have been successfully utilized in the diagnosis of multiple infectious processes [11–14, 18]. In the peri-operative period, however, the utility of any acute-phase reactants is complicated, as elevation of the ESR is directly related to the degree of tissue destruction [23] and the presence of instrumentation [24].
Several studies have attempted to characterize the trend of inflammatory parameters following surgery.
Jönsson et al. [25] investigated the ESR and WBC count at fixed intervals after uncomplicated surgery of the lumbar spine and described a rapid increase of the ESR, with a peak value on the 4th post-operative day and normalization at 2 weeks. This study found no corresponding change in the post-operative WBC counts. The authors concluded that the ESR is useful in the diagnosis of post-operative infection at time points beyond 2 weeks from surgery. Studies from the total arthroplasty literature have documented this same trend of early ESR elevation following uncomplicated surgery. These, studies, however, have also noted that ESRs tend to remain elevated above normal levels up to a year following surgery [15, 16], making its utility questionable. Such studies, which demonstrate the slow and inconsistent return of the ESR to pre-operative levels, suggest that it is not helpful in heralding infection during the early peri-operative period.
Studies by both Clark and Shufflebarger [2] and Hahn et al. [3] have failed to identify any reliable laboratory parameters for infection in instrumented scoliosis surgeries and the authors of both studies concluded that normal ESR cannot rule out infection. Similarly, Mok et al. [26] prospectively observed the ESR in patients following spinal surgery. No significant difference, however, could be found in order to differentiate infected and non-infected patients with elevated peri-operative ESRs.
Despite this ambiguity, the ESR continues as a mainstay of clinical practice in evaluating post-operative fever. We are not aware of any previous studies that have described the trend of ESR and WBC counts in the peri-operative period. Similar to these quoted studies, we noted a predictable rapid increase in the ESR within the first week of surgery, followed by a return toward normal levels. This return, however, was slow in our non-infected population: the ESR remained elevated above normal levels in 78% of patients at 1 month post-operatively and in 53% of patients at 3 months. Elevated ESR in the peri-operative period is not a truly abnormal finding and, therefore, it may not be a useful laboratory parameter in the evaluation of peri-operative fever or in the work-up of early wound infection.
It is difficult to fully explain the few correlations which were evident in this study. The correlation between the number of vertebral levels fused and the measured ESR at 7 days post-operatively is likely a reflection of the degree of tissue damage associated with a more extensive exposure and fusion. Why such a correlation is only apparent at 7 days post-operatively remains unclear. Similarly, the anterior surgical approach correlated with a lower ESR at 1 month post-operatively may also be related to tissue injury sustained at the time of surgery, as anterior approaches generally facilitate curve correction with the fusion of fewer vertebral levels than posterior or circumferential procedures and minimize muscle injury. However, we cannot explain why such a correlation is apparent only at the 1-month post-operative time point.
Any study focused on the use of acute-phase reactants as indicators of infection must comment on the potential utility of C-reactive protein (CRP) values in this arena. CRP values were not obtained in our study as they were not easily obtained at our institution during the study period. Despite this, various studies throughout the orthopedic literature have demonstrated its usefulness in predicting infection in the post-operative period, as the CRP value peaks earlier and returns to peri-operative values sooner than the ESR following surgery [15–17, 24, 26–30]. In various musculoskeletal infectious processes, the CRP value can be elevated within 24 h of the onset of symptoms, whereas the ESR may take up to 72 h to become abnormal. Correspondingly, the decline in elevated values, due to improvement in or resolution of the infectious process, is more rapid in the CRP value than in the ESR. Hence, the more rapid response of the CRP value makes this measure more valuable in the early detection of an acute infection, such as in this particular study, in the post-operative patient. Without having systematically analyzed CRP values in this population, we can make no specific recommendations with respect to its utility. It stands to reason, however, that CRP values should play a role in this clinical scenario. At our institution, our present protocol in the evaluation of SSI is to obtain ESRs, CRP values, and WBC counts and to interpret these values in light of the complete clinical presentation. That acute-phase reactants are laboratory values reflective of multiple demographic and clinical factors cannot be overlooked. While it is tempting to use these as surrogates to clinical judgement, our study suggests that they should, rather, be seen as a small piece of a larger clinical puzzle.
The limitations of our study include its retrospective nature, the lack of comparative data from a cohort of patients who had post-operative courses complicated by wound infection, and its relatively small patient population. Its strengths, however, lie in its long follow-up period and its diversity of patients and surgical approaches included.
Summary
The use of post-operative WBC counts and ESR levels must be approached with caution. The failure of the ESR to return to a normal level in the early post-operative period cannot be interpreted as an indicator of infection, as a significant proportion of non-infected patients maintain an elevated ESR well into the first 3 months following surgery. The ESR remains in the abnormal range in 78% of patients at 1 month post-operatively, in comparison to only 6% of patients who have an elevated WBC count. In the work-up of a potential early SSI, the ESR is of limited value, but elevated WBC counts may be a better measure. Though the value of a single WBC count or ESR value can be limited, serial values may be beneficial if a trend in the values can be elucidated. An increase of the ESR or WBC count levels may also be helpful if they are able to be correlated with changes in the patients’ clinical picture.