
Abstract
Abstract
Purpose
X-rays are presented on CD-Rs in a digital format with increasing frequency. This technique is potentially more time-consuming for the clinician compared to conventional pictures.
Methods
Ten sets of six X-rays for each case were prepared in both the conventional way and in digital format on CD-R. The order was randomised. Time in seconds was measured for six experienced orthopaedic residents to present the most recent a.p. view out of a given set. As a precondition, the computer was turned on and the same viewing software was used for all digital sets. The results were compared using a non-linked Student's t-test (significance level P = 0.05).
Results
The presentation of conventional X-rays required 21 s (±7.5 s) and of digital X-rays 90 s (±27 s), respectively (P < 0.001).
Conclusion
In spite of ideal conditions, digital X-rays on CD-R need significantly more time in the orthopaedic clinic. In major centres, patients present with different software and software in other languages, which increase the required time even further. This latter problem will be assessed in another study. This increase of preparation time required by a highly qualified staff member has implications on the economics and logistics and has a negative impact on daily clinical practice. One of the solutions might be that the CD-Rs be given to the registration desk and the data being already prepared when the patient sees the doctor. This can also include it being implemented in the digital system used in the inpatient part of the hospital and, therefore, making any other consultations or second opinions easily accessible.
Introduction
In the last few years, the quantity of information presented in a digital format has increased greatly. Picture archiving and communication systems (PACSs) were introduced, hospitals went fully digital and the amount of data that has to be transferred between hospitals and radiology departments on CD-R has increased. This is a challenge especially in the environment of the outpatient clinic.
One of the main problems is how to view the data in an efficient time considering the dedicated viewers from different vendors, which come often in different languages and need different software packages in order to be operated [1].
There is a number of research articles on the comparison of digital radiography, computed radiography and conventional radiography in terms of workflow, technologist productivity, overall speed of service, potential cost justification, cost analysis, improved patient and quality of care, patient satisfaction, pros and cons of going digital and diagnostic accuracy [2–9]. Further research focusses on the problem of integrating external CD-Rs into the normal workflow [1], but an efficient method for the outpatient clinic has not yet been found.
For a physician to view the data of an external CD-R within the workflow of an outpatient clinic potentially requires more time than to view a conventional X-ray. Therefore, the purpose of this study is to measure and compare the time needed to present:
A conventional X-ray, compared to A digitalised X-ray
In this study, we test the hypothesis that the presentation time for the conventional X-ray is significantly shorter than that for the digital ones.
Materials and methods
Six orthopaedic residents (all close to board examination) were chosen as data collectors. There were 10 sets of conventional and 10 sets of digital (CD-R) X-rays, with each set containing six plain pictures.
The computer was turned on, no password was needed and the same viewing software was used for all digital sets. No installation program was needed and the CD-Rs’ language was German, which is the native language of all participants.
The X-ray viewing box was turned on as well.
Time (in seconds) was measured from the moment that the person received the data until the latest a.p. picture was presented. The data was given in a randomised order.
The results were compared using a non-linked Student's t-test with a significance level of P = 0.05.
A time difference of 30 s or more between the two groups was defined as clinically relevant.
Results
The results show a statistically significant difference in time between the presentation of conventional and digital X-rays (Table 1). The conventional group had an average of 21 s and the digital group had an average of 90 s with a P-value of 0.001.
Results (in seconds) of the time between the presentation of conventional versus digital X-rays
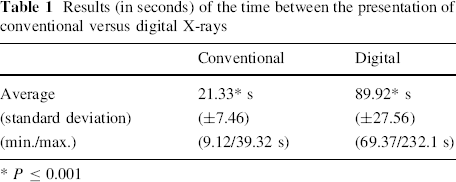
P ≤ 0.001
Discussion
The time needed for the presentation of digital imaging data depends on the computer system and software, as well as on the origin of the CD-Rs. Very often, hospitals have different software for burning and presenting digital data [1]. International CDs need installation programs and have introductions and explaining parts in the country language that the patient comes from.
To find a way for solving this problem, van Ooijen et al. [1] showed in their study that all “DICOM (digital imaging and communication in medicine) files from the CD-ROM are read, the DICOM header is changed to comply with the patient ID number in the actual hospital and then store the data either in the PACS or the web server.” In order to integrate such a handling system in the workflow of an outpatient clinic, it is necessary that the CD-Rs are sent by postal services before the appointment takes place. The procedure is time-consuming and needs a good logistics workout.
Andriole et al. [3] concluded in their study that “digital radiography can provide the most improved workflow and technologist productivity” over computed radiography and even more over screen-film. These findings were shown in a high-volume outpatient ambulatory setting in a department for radiology. X-ray technologists would rate the digital system as “much better” than the screen-film system. The patient throughput was increased when using the digital system. There are a number of articles with similar findings, but no research has yet been done on the workflow assessment in an orthopaedic outpatient department. Our findings show that the workflow is decreased by digital radiography, respectively, and needs more logistics work in order to keep the workflow efficient.
Other factors that play a role in the time consumption to present the data is the computer knowledge that each resident has and the manual abilities required to retrieve conventional X-rays.
As per definition, the resolution of the conventional X-rays, although in the DICOM format, does not allow conclusive assessment from the legal point of view. A format with easier access would be a good step forward: the JPEG format is easily accessible, conventional software can be used and there is no need to install a DICOM viewer on the computer. The great variety of DICOM viewers on the market and connected to the CD-R results is an additional major loss of time caused by trying to handle the software. There is no good reason for the DICOM format.
Mathie et al. [10] defined three important steps for processing an image: data acquisition, image display and image interpretation. These aspects can be discussed separately considering the introduction of a digital system and the influence that these aspects have on each other and also evaluating each aspect on the above mentioned factors, such as costs, effectiveness, satisfaction of staff, patients etc.
It is important to notice that this study intended to examine the image display part only in the environment of an orthopaedic outpatient clinic; it did not intend to examine and evaluate data acquisition, image interpretation or computer systems, but did intend to show what obstacles may occur when using a computer system to view digital images.
The standard deviation in the digital group was higher than in the conventional one. This is due to the fact that, even when using the same computer and same software every time, the computer would not always react in the same way. Sometimes, it took longer until the CD-R was accepted, it broke down in between and had to be restarted, the computer knowledge of the candidate was low or (s)he was unfamiliar with the viewing program, and once when using the wrong key, the whole procedure of starting the program had to be redone.
In comparison to the digital group, the standard deviation in the conventional group was much lower, since the presentation was only dependent on the resident's ability to find the latest picture and to have the manual ability to present it as fast as possible.
Although in this study the best conditions for presenting digital data were given, it still took an average of 69 s more to present the digital X-rays in comparison to the conventional ones.
Economics wise, it can be calculated that, considering 30 patients with digital data a week with 10 months of working each year requires two extra full doctor's working days of 10 h each alone for the extra time to present digital X-rays. This is not acceptable in an outpatient clinic setting.
Introducing digital data and technologies is commonly accepted, and was embraced at an early stage. Many articles show, often in a retrospective way, cost, efficiency and practicability analysis [4, 5, 8, 11]. Wade and Oliver [12] speak of, when looking back, “a complicated mix of failures, near successes, unconditional successes, failed promises, lack of standardised vocabularies and structures.”
It is regarded as a relief by most radiologists, but more or less as a nuisance by most orthopaedic surgeons. These different points of view need to be discussed in orthopaedic societies.
In an orthopaedic outpatient clinic, the workflow and efficiency of the consultant is based on an easy and quick access to the data.
There are many different aspects and points of view for comparing digital with conventional data.
Radiology department staff, X-ray technologists, radiologists and orthopaedic surgeons in in- and outpatient clinics have different experiences and opinions of digital imaging. The overall speed of service, patient care and patient satisfaction are factors that are improved by introducing digital imaging in a radiology department [3]. In the outpatient clinic, introducing digital imaging, as shown in our study, means more time for presenting the data and, therefore, less time for the patient, slower speed and decreased patient satisfaction.
Introducing a digital system in a hospital is linked with high costs [3–5], which resulted in studies about cost analysis, effectiveness of systems, productivity and other factors when considering the pros and cons. Maass et al. [5] showed in their study that a digital system increases the costs, but also mentioned that costs and savings “represent merely one aspect of the digital archiving project.” Patient satisfaction, speed of service and efficiency will not show immediate results when considering the costs, but will play an important role in the long term.
Another aspect of introducing digital imaging is the challenge for radiologists. Reiner et al. [13] analysed the productivity of radiologists in the interpretation of computed tomography (CT) scans comparing hard films with soft-copy pictures and found “substantial time savings with PACS.” Fleishon et al. [14] compared the radiologists’ reading times using PACS and using films. Here, PACS had no effect on the radiologists’ interpretation times, but it is important to consider other opportunities to realise savings, such as flexibility in manipulating images, reading more images per examination, decreasing the number of lost images, benefits to patient care, improvements in image interpretation etc.
Reiner et al. [9] examined radiologists and the accuracy of their interpretations of CT scans comparing hard- and soft-copy images. He found a significant improvement in sensitivity, specificity and accuracy of the interpretations in the soft-copy group. This is an important fact when considering the pros and cons of digital imaging.
The solution for using digital data cannot be to turn back the wheel of time and to use only conventional X-rays, but adjustments need to be made, and these might be individual solutions for each outpatient clinic. They include adjustments such as the standardisation of the software and the computer systems used in the hospitals. CD instructions need to be in the native language as well as in English.
It is also possible that the CDs could be given to the registration desk and the data being already prepared when the patient sees the doctor. This can also include it being implemented in the digital system used in the inpatient part of the hospital and, therefore, making any other consultations or second opinions readily available.