
Abstract
Abstract
Purpose
The objective of this study was to explore whether there were any differences between the theoretical recommendations for children's supracondylar humeral fractures (CSHF) according to the American Academy of Orthopaedic Surgeons (AAOS) guidelines and the treatments they actually received in our institution.
Methods
We retrospectively reviewed the medical charts and radiographs of all CSHFs at our hospital between January 2015 and December 2018. In all, 301 children meeting our inclusion criteria were identified and evaluated using the AAOS-Appropriate Use Criteria (AUC) application for supracondylar humerus fractures. Actual treatment was then compared with the treatment recommended by the AUC.
Results
Actual operative management was undertaken in 0/58 (0%) Gartland type I fractures, 61/108 (56.5%) type II fractures and 98/135 (72.6%) type III fractures. Actual nonoperative management was undertaken in 58/58 (100%) Gartland type I fractures, 47/108 (43.5%) type II fractures and 37/135 (27.4%) type III fractures. Surgeon decisions for nonoperative treatment were in agreement with the AUC recommendations 100% of the time, whereas surgeon decisions for surgery matched the AUC recommendations 65.4% of the time. Predictors of actual operative management were age (p =0.003), fracture classification (p =0.000), associated orthopaedic injury requiring surgery (p =0.025) and anterior humeral line (AHL) not intersecting the capitellum (p =0.008).
Conclusion
We found low agreement between actual treatments and the AUC-recommended ‘appropriate’ treatments. The AUC favoured operative intervention more frequently largely on the basis of fracture classification while we emphasized age, fracture classification, associated orthopaedic injury requiring surgery and alignment of the AHL with the capitellum in our operative decision-making process.
Level of evidence
Therapeutic Level II
Keywords
Introduction
In an effort to improve treatment of children's supracondylar humeral fractures (CSHF), the American Academy of Orthopaedic Surgeons (AAOS) published clinical practice guidelines in 2011 based on the best available evidence. 1 These guidelines consisted of 14 recommendations, with four graded weak, eight graded inconclusive and two graded moderate. More recently, the AAOS translated these recommendations into Appropriate Use Criteria (AUC) for the nonoperative and operative treatment of CSHF based on the recommendation of an expert panel,2,3 and made the AUC widely available to orthopaedic surgeons through a free web application. Some studies have concluded that with the introduction of electronic medical charts, an AUC application became attractive and easy for orthopaedic surgeons to utilize in clinical practice.4–6 The application also provided a genuine opportunity for study quality improvement. The AUC could potentially improve clinical practice by directing the surgeon to treatments that were agreed on, and might thus reduce variation in surgical treatment of these fractures. 4 However, other studies also raised some controversies about the AUC, including the vague definitions of urgent and emergent cases and the necessity of urgent treatment for all type III fractures.4–6
In real clinical practice, it was likely that decisions surrounding management of CSHF deviated from the official recommendations of the AUC. The objective of this study was to explore whether there were any differences between the theoretical recommendations for CSHF according to the AAOS guideline and the treatments they actually received in our institution. We also explored the factors affecting the decision for choosing operative intervention and saw whether they were consistent with the operative recommendations of the AUC.
Materials and methods
Study population and study design
After approval from the institutional review board of our hospital (No. L-2014-22,17 October 2014), we retrospectively reviewed the records of consecutive children with supracondylar humeral fractures between January 2015 and December 2018 at our clinic. The inclusion criteria were: 1) age from two to 12 years; 2) unilateral supracondylar humeral fractures; 3) with pre-treatment and post-treatment radiographs; 4) no history of elbow injuries and related operations. The following patients were excluded: 1) less than two or >12 years old; 2) polytrauma patients; 3) associated with vital organs damage; 4) pathological fractures and old fractures (not be operated on more than two to three weeks after initial injury); 5) the follow-up data were inadequate or absent. Finally, 301 children met our inclusion and exclusion criteria and were included in this study.
Demographic information recorded at the time of the original injury included patient age, sex, body mass index (BMI), injured side, mechanism of injury, fracture classification, initial fracture displacement, associated orthopaedic injury, position of the anterior humeral line (AHL) versus the capitellum at time of injury, vascular and neurological status and open or closed fractures. The mechanism of injury included traffic injury, ground fall and sports injury. Fracture was classified using the modified Gartland fracture classification system. 7 We also measured the initial fracture displacement. In the 301 patients with presentation radiographs, the maximum displacement of the distal fracture fragment was evaluated and calculated in millimetres. This number was then normalized by dividing the maximum displacement in millimetres by the width of the humerus just proximal to the fracture site. Position of the AHL versus the capitellum at time of injury fell into two categories: the AHL intersected the capitellum and the AHL did not intersect the capitellum. Moreover, binomial and multivariate logistic regression analysis were performed to assess which clinical and radiographic factors were most predictive of the decision for operative management. The humerus-elbow-wrist angle (HEWA) and Baumann angle (BA) on anteroposterior radiographs and lateral humerocapitellar angle (LHCA) on lateral radiographs were measured. All the radiographic measurements were performed in a uniform manner by two orthopaedic surgeons (NFT and YSW). The Flynn grading system 8 was used to assess functional results of treatment at the last follow-up. The outcome was rated excellent if there was <5° of movement lost in the plane of flexion and extension and the carrying angle was within 5° of the normal side; good if there was 5° to 10° of movement lost and the carrying angle was within 5° to 10° of the normal side; fair if there was 5° to 10° of movement and the carrying angle was within 10° to 15°of the normal side; and poor if there was>15° of movement lost and the carrying angle was >15° of the normal side.
Statistical analysis
Distributions of data in our study were checked. Percentages were used for categorical data, and means or medians were used for continuous data. Student's t-test was used for the comparison of continuous variables and the chi-square test for the comparison of categorical variables. A multivariate logistic model was fit predicting the decision for operative management. All variables were included as possible predictors and a final model was found using stepwise elimination. All analyses were performed using SPSS software, version 22.0 (SPSS Inc., Chicago, Illinois). The level of significance was set at p < 0.05.
Results
There were 301 patients who met the above inclusion and exclusion criteria. The average follow-up time of our group was 30.2 months (sd8.4; 24 to 39). Each variable such as patient age, sex, BMI, injured side, mechanism of injury, fracture classification, initial fracture displacement, associated orthopaedic injury, position of the AHL versus the capitellum at time of injury, vascular and neurological status and open or closed fractures were described in detail in Table 1.
Baseline characteristics of 301 patients with supracondylar humeral fractures
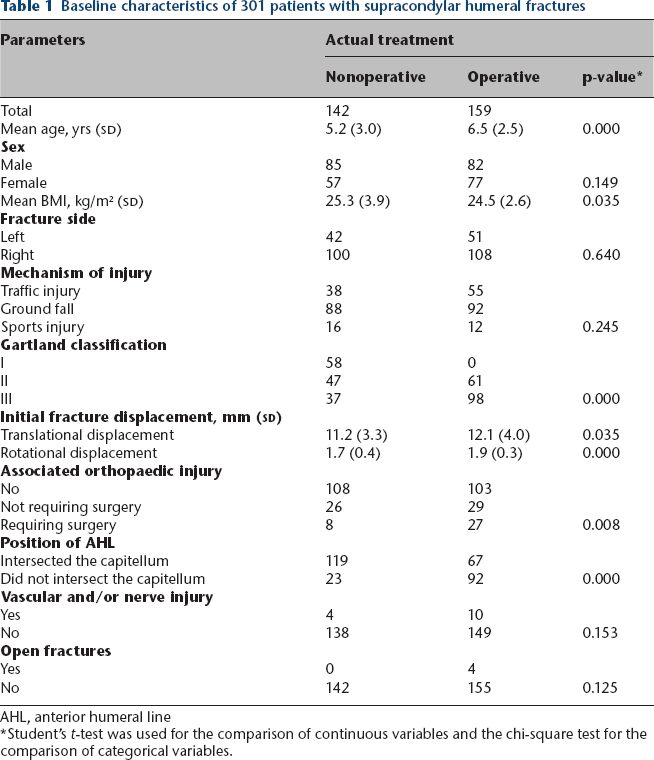
AHL, anterior humeral line
Student's t-test was used for the comparison of continuous variables and the chi-square test for the comparison of categorical variables.
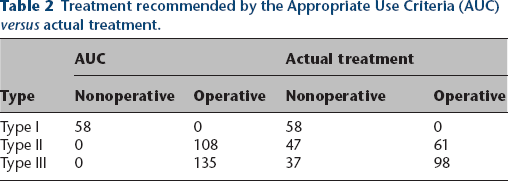
Actual operative management was undertaken in 0/58 (0%) type I fractures, 61/108 (56.5%) type II fractures and 98/135 (72.6%) type III fractures. Actual nonoperative management was undertaken in 58/58 (100%) type I fractures, 47/108 (43.5%) type II fractures and 37/135 (27.4%) type III fractures. Those type III fractures not operated on were firstly treated by closed reduction and cast immobilization in the emergency room. They were successfully reduced and maintained acceptable alignment during treatment. All these patients achieved excellent or good results assessed by the Flynn grading system. Among 301 patients, 84 were treated nonoperatively despite AUC recommendations for operative treatment. According to the data of our group of cases, surgeon decisions for nonoperative treatment were in agreement with the AUC recommendations 100% of the time, whereas surgeon decisions for surgery matched the AUC recommendations 65.4% of the time (Table 2).
Treatment recommended by the Appropriate Use Criteria (AUC) versus actual treatment.
On the first postoperative day, the mean BA was 69° (62° to 81°), the mean HEWA was 11° (2° to 15°) and the mean LHCA was 41° (33° to 52°). At last follow-up, the mean BA was 69° (62° to 81°), the mean HEWA was 11° (2° to 16°)and the mean LHCA was 41° (33° to 53°).The comparisons of the BA, HEWA and LHCA on the first postoperative day and at the final follow-up indicated that they were not different (p>0.05). According to the Flynn grading system, 236 (78.5%) patients had excellent, 40 (13.3%) patients had good, 21 (7.0%) patients had fair and four (1.2%) patients had poor results.
Binomial logistic regression revealed that the four factors predictive of operative intervention were age, fracture classification, initial fracture displacement, associated orthopaedic injury and AHL not intersecting the capitellum (Table 1). Other common considerations such as sex, BMI, injured side, mechanism of injury, open injury and nerve and vascular injury were not significant predictors of operative intervention. Results from the multivariate logistic modelling showed that predictors of actual operative management were increasing age (p =0.003), fracture classification (p =0.000), associated orthopaedic injury requiring surgery (p =0.025) and AHL not intersecting the capitellum (p =0.008) (Table 3).
Multivariate logistic regression analysis of predictors of received operative treatment for children supracondylar humeral fractures (n=301)

Discussion
The most significant recommendations of the AUC included nonoperative treatment of modified Gartland type I fractures, closed reduction and percutaneous pinning of modified Gartland type II, modified Gartland type III and flexion-type injuries. From our study, we found in real clinical practice that some decisions surrounding management of CSHF deviated from the official recommendations of the AUC. For Gartland type I fractures, our management was consistent with the AUC recommendations: both supporting non-surgical treatment. On the contrary, for Gartland type II and Gartland type III fractures, our actual clinical treatment was not consistent with the theoretical treatment recommended by the AUC. Our results indicated that there was a low agreement between actual treatment decisions and the AUC-recommended ‘appropriate’ treatments, especially for the type II and III fractures. Despite the lack of consistency with the AAOS recommendations, our series still achieved 91.8% good-excellent radiological and functional outcomes assessed by the Flynn grading system, which was consistent with the good-excellent results previously reported to be between 52% and 100%. 9
Although some recommendations of the AUC had some advantages, such as improving quality of care by informing surgeon decision-making and ultimately improving outcomes for a particular orthopaedic injury or condition, its shortcomings were also obvious. The AUC's most highly ranked treatment recommendation for type II fractures was operative management regardless of severity. However, the range of injury severity of type II fractures raised the question of whether some could be treated successfully nonoperatively. Moreover, the AUC recommended urgent treatment for all type III fractures, the necessity of which had also been questioned. Ibrahim et al 4 compared the AUC recommendations with actual clinical management of supracondylar fractures. Their study concluded agreement in the majority of cases, though they did disagree in 11% of operative cases. Another study found increased disagreement in 31% of cases with the AUC recommendations in some clinical scenarios. 5 Kazimoglu et al 6 found the AUC was appropriate for 100% of type I, only 25 (5.9%) of type II and 389 (96.0%) of type III fractures. Overall, the total appropriateness rate was 54.5%. Our study concluded disagreement in 34.6% of cases with the AUC recommendations, within the range of ratios of the above studies.4–6 The reasons for the inconsistency of the above findings might be as follows. First, surgical decisions entailed many factors beyond those included in any single set of AUC and as a result, any AUC would have limitations that might restrict application for some patients. Relying on expert panels would produce AUC that were specific in the local culture and practice of medicine of the panel and AUC require continuous updates. Moreover, difference in sample size would affect the accuracy of the final result. Finally, the overall treatment philosophy of surgeons in different countries and regions might have significant differences.
The results of binomial and multivariate logistic regression analysis showed that increasing age, fracture classification, associated orthopaedic injury requiring surgery and AHL not intersecting the capitellum played important roles in our operative decision-making process. Age and fracture classification had always been important factors influencing the decision of surgical intervention of children fractures.10,11 Previous studies on other fractures, such as femoral shaft fractures and the radius and ulna shaft fractures, also found age and fracture type were important factors in determining whether or not to undergo surgical intervention.12–15 Associated orthopaedic injury requiring surgery was also an important factor affecting the choice of surgery. One explanation was that these femoral shaft fractures were managed surgically to assist with mobilization and to facilitate rehabilitation of their other injuries. Moreover, surgeons were more likely to choose operative management of a supracondylar fracture when the patient was already in the operating suite, and the risks of anaesthesia had already been undertaken. AHL location was commonly used to evaluate sagittal alignment after fracture reduction in CSHF.16,17 Kao et al 16 found children with AHL anterior to the capitellum had less elbow flexion angle (125.8° versus 131.2°, p =0.046) and less total range of elbow movement (128.3° versus 135.7°, p =0.048) than children with AHL crossing the capitellum. The results of our series were also consistent with the outcomes of the above studies.
Several limitations existed in our study. First, the study enrolled only a small number of patients. Larger sample sizes were still needed to further convince these results. Secondly, the study design in which injury and results data were obtained retrospectively, therefore, the final outcomes depended on the accuracy of documentation. Thirdly, although we brought as many factors as possible into the research, there were still some factors that could not be fully incorporated, such as polytrauma, subspecialty of treating surgeon, insurance and socioeconomic status of the family. Moreover, effective statistical analysis could not be performed resulting from too few patients with open injury, nerve and/or vascular injury.
Conclusion
We found low agreement between actual treatments and the AUC-recommended ‘appropriate’ treatments, especially for the type II and III fractures. The AUC favoured operative intervention more frequently largely on the basis of fracture classification while we emphasized age, fracture classification, associated orthopaedic injury requiring surgery and alignment of the AHL with the capitellum in our operative decision-making process. The AUC guidelines need to be further improved.
Footnotes
NFT, XBY and HC participated in data collection.
YSW and LJS contributed to interpretation of the results.
TW and JY drafted the initial manuscript.
All authors critically revised the paper and approved the final manuscript as submitted.