
Abstract
Abstract
Purpose
To suggest different procedures tailored for hip reconstruction in type II late sequelae of septic arthritis.
Methods
The severely deformed subluxated or dislocated femoral head is reshaped in accordance to radiographic and on-table assessment (osteochondroplasty). Sixteen hips in 13 patients (three bilateral) were the subject of this study. They were all affected during incubation in the first few weeks after birth. Age at operation was in the range 2–12 years (average 5.3). The main complaint was instability, stiffness during walking and the inability to sit comfortably, limb length discrepancy, and mild pain on walking. Preoperatively, the range of motion was limited to a certain degree in different directions in all cases. Plain radiography, computed tomography (CT), or multi-slice CT with reconstruction 3D views were of benefit in analyzing the problem preoperatively. Magnetic resonance imaging (MRI) was performed for selected cases after 2 years to test for the viability of the femoral head.
Surgical technique
A modified approach was used to adequately expose the iliac bone, the hip, and the upper third of the femur. Meticulous dissection to preserve the amalgamated capsule and a well-planned capsulotomy for later adequate capsulorrhaphy is essential. Debridement to clear the acetabulum from intra-articular fibrosis is attempted prior to acetabular reconstruction (Salter, Dega, or triple pelvic osteotomy). Head and neck reconstruction (osteochondroplasty) is performed according to the nominated topography of the deformed head (beard, collared, staghorn, etc.). A carefully planned reshaping in a manner not disturbing the superior weight bearing articulating surface with the acetabulum will allow easy containment in the reconstructed acetabulum. Associated subluxation or dislocation will dictate adequate shorting with femoral cuts inclined in a manner bringing the impinging overgrown greater trochanter down, achieving a near to normal neck shaft angle.
Results
According to the criteria proposed by Hunka et al. (Clin Orthop Relat Res 171:30–36, 1982), a satisfactory result is considered when a stable pain-free hip is achieved with flexion arc >70° and flexion contracture <20°. This was true in 13 hips. It appears that better results are achieved in younger children with minimal intra-articular adhesions limiting hip movements, and with less destruction of the articular cartilage. A final improvement in the range of movement should not be expected before 6–12 months. Intensive physiotherapy to improve postoperative stiffness is required.
Conclusion
The proposed reconstruction procedure for reshaping the deformed femoral head (osteochondroplasty) is a salvage attempt that achieved a more or less mobile painless stable hip joint besides restoring the normal anatomical relationship, should total hip replacement (THR) be needed in the future.
Keywords
Introduction
Despite recent advances in many aspects of orthopedic care, pyogenic arthritis of the hip remains a serious problem. Delay in diagnosis and aggressive therapy could end with a disastrous sequelae [1].
The aim of this study is to suggest different surgical procedures tailored according to the intraoperative findings for type II late sequelae of septic arthritis. Osteochondroplasty is the term most suitable for reshaping procedures attempted for the severely deformed femoral head.
Materials and methods
Cases were collected from the health insurance hospital for newborns and school children in Alexandria (a tertiary-care hospital treating cases from the Western delta governorates). From 1997 until 2005, 16 hips in 13 patients were the subject of this study (three were bilateral). There were ten males and three females; the left hip was involved in 11 instances. All of them had a frank history of septic arthritis during incubation in the first few weeks of life.
Only three cases gave a history of attempted drainage at the governorate hospital, while the rest received medical treatment only. The problem was recognized by the parents on starting walking or on medical examination at school admission. The main complaint was instability in 16, stiffness during walking and inability to sit comfortably in 13, limb length discrepancy in six, and mild pain on walking in five. Plain radiography on referral showed delayed ossification or deformation of the femoral head. The age at operation ranged from 2 to 12 years (average 5.3 years). The period of follow up ranged from 2 to 5 years (average 3.4 years).
Preoperative examination revealed hip flexion contracture in 14 instances (range 5–30°) and adduction deformity in 11 instances (range 5–20°). The range of motion was limited to a certain degree in different directions in all cases. Flexion arc ranged from 40 to 90°, abduction was possible in five cases (range 10–15°). Limb length discrepancy ranged from 0.5 to 3 cm in the ten unilateral cases (Table 1).
Details of the 16 hips in 13 patients examined in this study
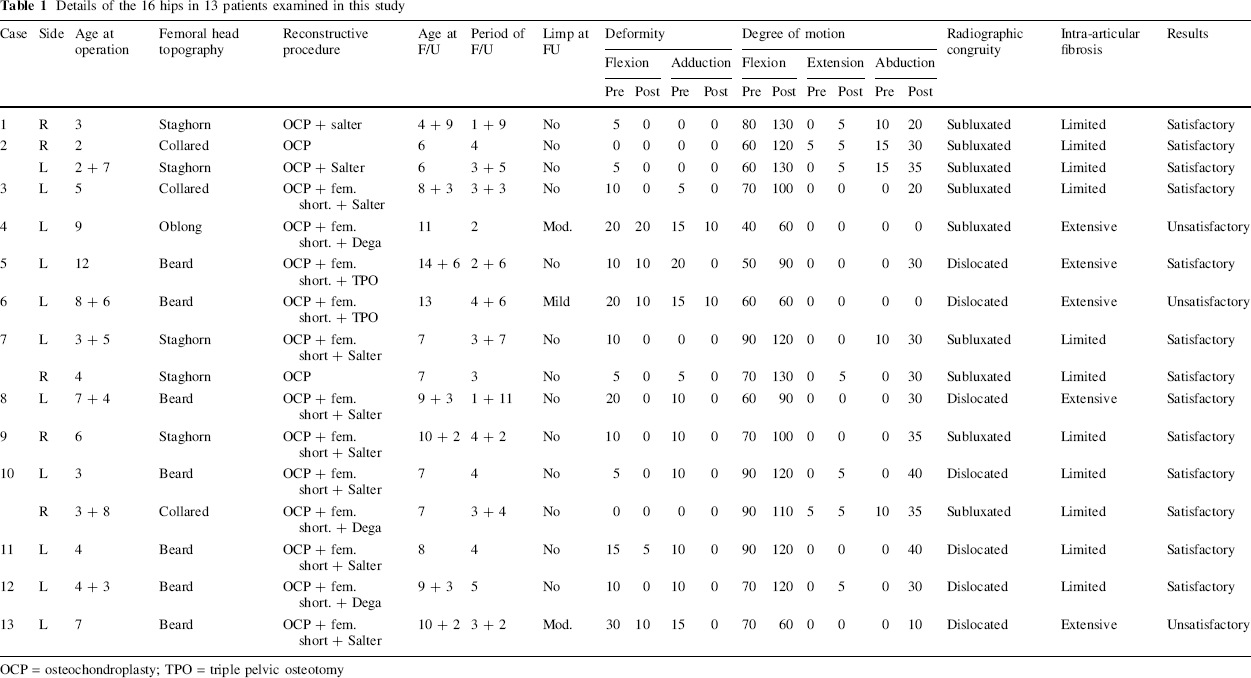
OCP = osteochondroplasty; TPO = triple pelvic osteotomy
Imaging studies
The following imaging methods were used in this study:
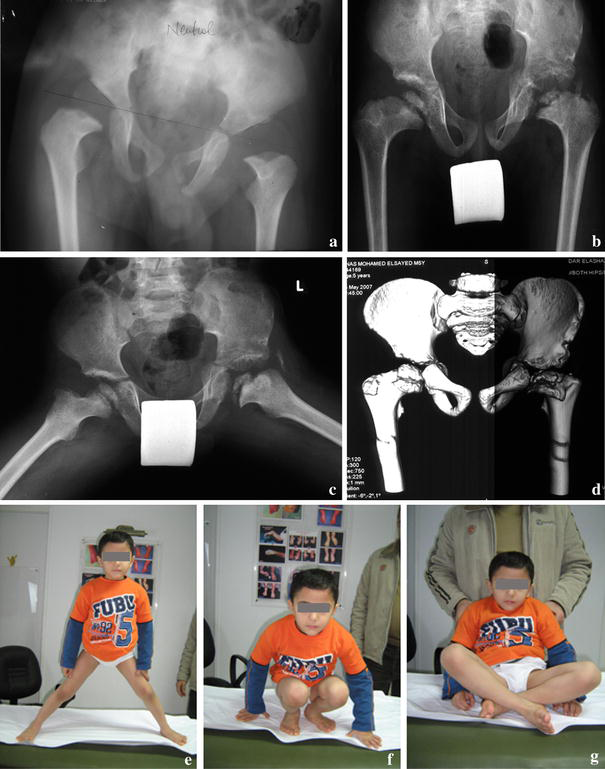
Plain radiography Antero-posterior (A-P) views in neutral and in abduction with extension were performed to reveal the magnitude of acetabulo-femoral impingement, femoral head deformation, and acetabular dysplasia. Lateral views and standing A-P views were also performed. Pre- and postoperative Multislice computed tomography (CT) with 3D reconstruction views were done in the last operated six cases only in this series and were found to be helpful in providing a panorama of the femoral head (Fig. 1).
Case number 6. Postoperative magnetic resonance imaging (MRI) was performed in only four cases to study the viability of the femoral head at 2 years follow up.
Surgical reconstruction was indicated in all type II cases showing radiographic acetabulo-femoral impingement with femoral head deformation and acetabular dysplasia. Associated subluxation was shown as broken Shenton's line (with delayed ossification of the femoral head in young children) or decreased center-edge (CE) angle of Wiberg (in older children), or total hip dislocation was a usual finding.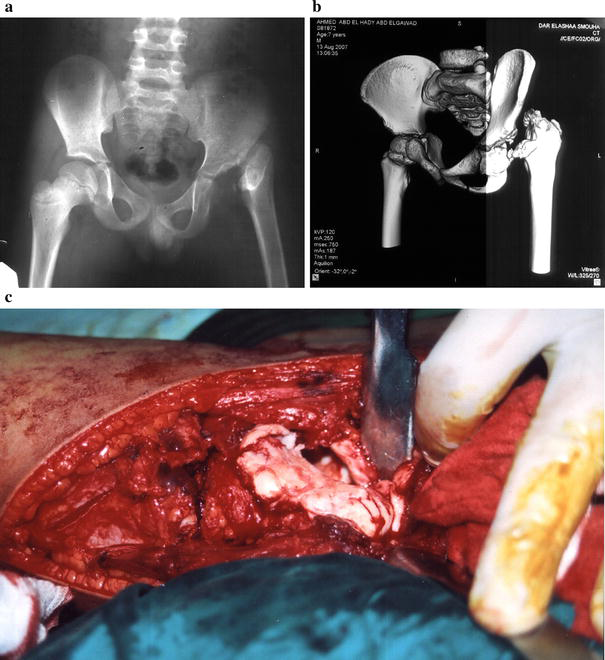
Surgical exposure
A modified anterior iliofemoral surgical approach is planned to give access to the hip joint and upper femur, together with adequate exposure of the pelvic bone. This allows a clear view and better understanding of the magnitude of the problem and easy handling and management. To begin, an extensive adduction tenotomy is performed through a vertical incision beginning from the adductor tubercle down to the ischial tuberosity. Pubic and ischial osteotomies in the case of triple pelvic osteotomy can be performed if needed.
To expose the hip, an incision is tailored extending from the iliac crest to a mid-inguinal point (i.e., a bikini incision). The incision is then turned distally and posteriorly to run parallel to the femoral shaft (Fig. 2). Develop the interval between the sartorius and tensor fascia lata, the latter is peeled off the iliac bone, hook and tenotomize the iliopsoas tendon. The iliac bone is, thus, exposed. Turn distally to expose and release the tendon of the rectus femoris, this will show the underlying fibrosed hip capsule, which is usually amalgamated to the glutei muscle. Careful meticulous, sharp dissection is required to free the capsule all round superiorly and inferiorly before attempting capsulotomy. The cuts should be well planned according to the topographic study of the head and the expected bony cuts. Next, develop the plan between the rectus femoris and vastus lateralis and then distally cut along the vicinity of the latter to expose the upper half of the femoral shaft. The whole view of the iliac bone, hip joint, and upper femur is, thus, clear (Fig. 2).
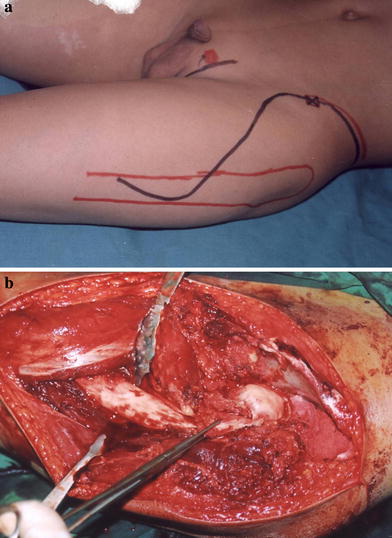
The modified iliofemoral approach.
Surgical technique
Capsulotomy
The incision starts 1 cm lateral to the labrum and extends from superior to inferior in order to widely open the joint, except in a few cases where the topography of the femoral head will dictate a different plan.
Debridement
Intra-articular fibrosis limiting femoral head movement is characteristic in all cases. The acetabular fossa is usually occupied by fibrous bands or covered by a fibrous membrane that should be sharply dissected to show the underling articular cartilage. The intra-articular fibrosis is described as “extensive” (five cases) when the posterior aspect of the subluxed deformed femoral head and neck is stuck to the acetabular rim, limiting any attempt of external rotation to reveal the actual topography of the femoral head. Sharp dissection is crucial to free the head and to clear the acetabular fossa before deciding the appropriate reconstruction. Intra-articular fibrosis is usually more pronounced with dislocated femoral head (beard heads) and was described as “limited” (11 cases) when the femoral head was easily manipulated with less dissection, which was usually the case in the subluxated heads (collared and staghorn).
Osteochondroplasty (femoral head reconstruction)
Different topographies of the enlarged deformed femoral head were observed. Care should be taken not to disturb the superior articulating surface. Trimming or shaving of the deformed head should be limited to the periphery.
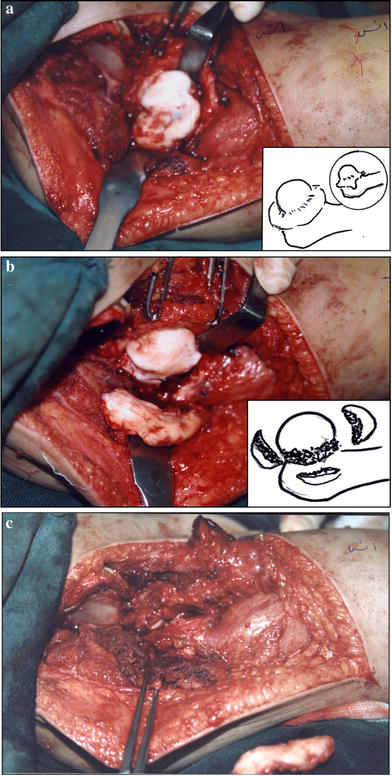
The beard head
The femoral head is of almost a normal size or larger with a secondary smaller beard extending downwards. The neck is abnormally broad, including the lesser trochanter, which may be hardly differentiated. This configuration is due to dislocation of the femoral head hanging over the superior acetabular rim. The stuck head is, thus, split into a usually larger upper dislocated sector and a smaller lower beard. The corresponding acetabulum rim (superior or anterolateral) is shallow. The child presents in flexion adduction deformity, a few degrees of flexion movement, and showing evident limb shortening. Extensive intra-articular fibrosis was a usual finding in these cases (Fig. 3).
The beard head.
Osteochondroplasty here is a tailored osteotomy resecting the lower part of the femoral head (the beard) and part of the shaft, which may sum to 5 cm of shortening. This will help slacken the surrounding soft tissues, bringing the head level with the acetabulum. The resulting reshaped small head is, thus, contained in the reconstructed acetabulum (seven cases).
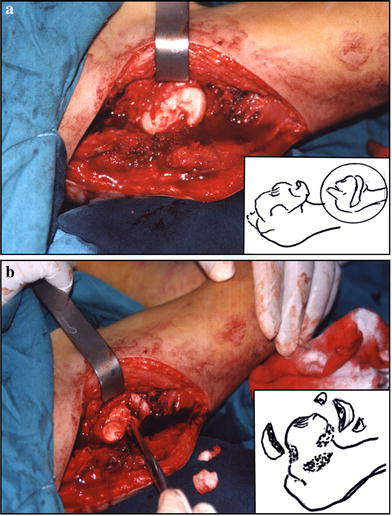
The collared head
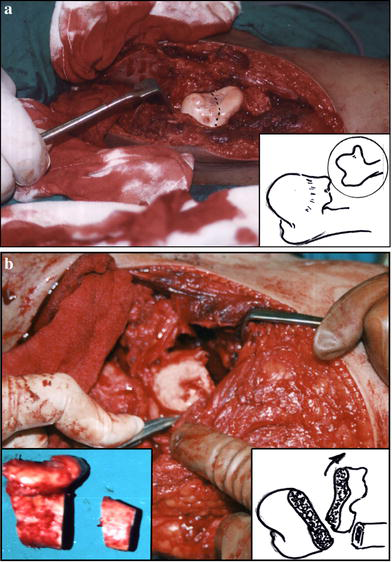
The femoral head is surrounded by a collar all around the neck with astonishingly maintained smooth superior weight-bearing cartilage. This collar is after the femoro-acetabular impingement preventing femoral head containment into the acetabulum on attempted internal rotation. Excision of the collar all round, carefully respecting the superior weight-bearing cartilage, will allow easy containment (three cases) (Fig. 4).
The collared head.
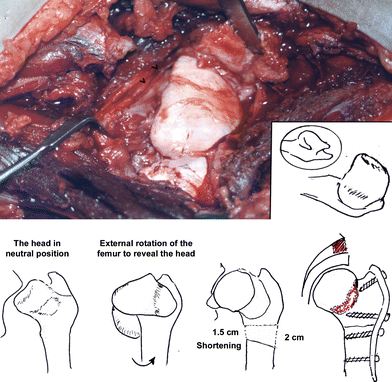
The staghorn head (Fig. 5)
The staghorn head is a description given to a head showing an irregular superior articular surface with several protrusions. One should try to preserve the superior main part of the head, estimating arbitrarily that corresponding to the acetabular weight-bearing surface, even if it appears partially irregular. Shaving the uneven peripheral protrusions will resize the head for easy containment (five cases).
The staghorn head.
Unclassified
The head may attain any shape. In only one case was the head unclassified. It appeared oblong and abnormally large in size (rugby ball) in a 9-year-old boy. Reshaping the head was difficult. The head was trimmed as shown in Fig. 6.
Oblong head (rugby ball). Osteochondroplasty was done by excising medial and lateral edges, together with shortening
For associated subluxation or dislocation
Adequate, generous femoral shortening with or without derotation is needed to bring down the femoral head. In doing so, the planned femoral cuts should be obliquely inclined as shown in Fig. 7 to correct the neck shaft (which is usually in varus), bringing down the overgrown, impinging greater trochanter, thus, improving the range of abduction. Additional shortening should be estimated to compensate for the pressure exerted on the femoral head following an acetabular reconstructive procedure.
Capsulorrhaphy in beard head cases.
Acetabular reconstruction
Following adequate debridement of the acetabular fossa, acetabular reconstruction is decided according to the deficiency present. Following containment, stability of the head is examined. If the defect is global, a Dega acetabuloplasty is selected (three cases); if it is anterolateral, Salter osteotomy is more effective (nine cases). Triple pelvic osteotomy (two cases) is reserved for the older children (8.6 and 12 years of age), allowing better caping and stability of the femoral head. In two hips (aged 2 and 4 years), acetabular reconstruction was not needed.
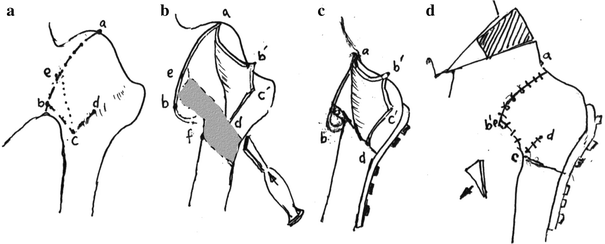
Capsular reconstruction
Preoperatively, the bone procedure will dictate the capsular cuts beforehand. This will allow clear fashioning of the flaps for later capsulorrhaphy. In the collared and staghorn heads, an ellipse is resected from the anterior capsule as usual for open reduction of developmental dysplasia of the hip (DDH). Capsular cuts in the beard head is different, since the whole lower half of the neck and head will be resected. The capsule should be fashioned in a way to preserve it being free, as shown in Fig. 7. The undersurface raw area of the head and neck will be easily covered by the capsular flaps. Following wound closure, a hip spica is applied for 6–8 weeks, after which intensive physiotherapy is required for as long as 1 year.
Results
The results of treatment was classified simply as satisfactory or unsatisfactory, on the basis of criteria that were proposed by Hunka et al. [2]. The result was considered as satisfactory when the following criteria were fulfilled: (1) the joint was stable; (2) with arc of flexion 70° or more, a flexion contracture no greater than 20°; and (3) the patient was free of pain and was able to perform activities of daily living.
On this basis, satisfactory results were achieved in 13 hips. They were all stable, painless, mobile joints with a flexion arc exceeding 70° and surprisingly good range of abduction and adduction. This final result was achieved after at least 1 year of intensive physiotherapy (Figs. 8, 9, and 10).
Case 2 (2-year-old boy with right collared and left staghorn heads). Operation: right osteochondroplasty only and left osteochondroplasty with Salter osteotomy.

Case 11 (4-year-old boy with a beard left femoral head). Operation: osteochondroplasty with femoral shortening and Salter osteotomy.

Case 5 (12-year-old boy with beard femoral head). Operation: osteochondroplasty with femoral shortening and triple pelvic osteotomy.
Analysis of unsatisfactory results (three cases)
The age at operation of the three cases with unsatisfactory results was 7, 8.6, and 9 years. They all presented with flexion–adduction deformity ranging from 10 to 30° and a limited range of flexion arc (40–70°). In two patients (cases 6 and 13), the head was beard, with radiographic dislocation and intraoperative extensive adhesions requiring sharp dissection to free the stuck femoral head, and up to 5 cm of femoral shortening to bring the femoral head level with the acetabulum. Salter osteotomy was performed in one and a triple pelvic osteotomy in the other. The articulating cartilage was markedly eburnated in both (Fig. 1c). The third hip (case 4) had an oblong head; the plain radiograph showed limited subluxation, yet reshaping of the head ended with a large encircling raw bone that could be blamed for the resulting stiffness (Table 1). Hips with limited intra-articular fibrosis (11 cases) had a better preoperative range of motion, with radiographic subluxation in eight of them reflecting less aggressive sequelae (Fig. 4a). Most of them presented for consultation at an early age.
It appears that the severe intra-articular adhesions with a badly degenerated articulating cartilage in older children were the cause of unsatisfactory results. In no case was avascular necrosis a complication to be blamed for the unsatisfactory outcome after a follow up period of 2–5 years.
Radiographic assessment
In the beard head cases, the head following reconstruction appeared smaller in size, with small residual epiphysis well contained in the reconstructed acetabulum. A-P views in abduction revealed the well-contained mobile femoral head. Femoral osteotomy showed union at about 3–4 months.
Multislice CT with reconstruction views was helpful to show the degree of achieved containment. MRI revealed a viable head in the four examined cases.
In the collared and staghorn head cases, preoperative associated subluxation was minimal in comparison to the beard head, with a better range of hip movements reflecting less aggressive sequelae. In young children with delayed ossification of the femoral head, successful containment was evident as a well-developed intra-articular epiphysis. MRI was not needed in these cases.
Discussion
Late sequelae of septic epiphysitis of the hip remain as one of the challenging problems in pediatric orthopedics. The recent study aims at a better understanding of type II sequelae, with special focus on the usually associated subluxation or dislocation, which add to the difficulty of reconstruction. On reviewing the literature, Hunka et al. [2] were the ones who gave a precise accepted classification that lead to a better understanding of the process. This was further modified by Choi et al. [3], yet none of these researchers focused on the associated dislocation secondary to the severely deformed and hypertrophied femoral head compounding the problem. According to them, the epiphysis, physis and metaphysis are involved with the resulting coxa brava (IIA) or progressive coxa vara or coxa valga (IIB). These hips usually have radiographic evidence of delay in ossification, flattening, and irregularity of the femoral head and coxa magna. The femoral head is short and wide, and there is a relative overgrowth of the greater trochanter because of the premature closure of the capital physis [3]. The absence of physiologic load bearing for bone growth and progressive soft-tissue contracture will increase the deformity and make further treatment more difficult [4–6].
In this study, the author proposes a reconstructive procedure of the deformed femoral head (osteochondroplasty) based on their topography revealed at surgery and the preoperative imaging study (plain radiography and possible multislice CT), which helps understanding the magnitude of the problem and the expected capsular and bony cuts required. The main cornerstone to a successful outcome is to preserve the superior articulating surface by all means.
In a beard head, the superior sector of the head is never touched; shortening of the femur will include the inferior sector (the beard). The bony cuts are inclined to restore near-normal neck shaft angle, bringing down the greater trochanter, thus, relieving acetabulo-trochanteric impingement and improving the range of abduction and femoral head containment. However, in the collared and staghorn heads, the cartilaginous protrusions at the periphery causing acetabulo-femoral impingement are shaved off with no ill effect on the range of movement.
Although the remodeling potential of the hip with septic sequelae is less than that in developmental hip dislocation [7], Freeland et al.[5] believed that any physeal cartilage found on exploration of the hip should not be sacrificed, however severe the damage, because there is potential for growth and development. The author observed that, in young children, the femoral articular cartilage may appear to be healthy compared to older children with eburnated cartilage. Still, the expected ironing of the congruent surfaces following containment will achieve a more or less painless mobile stable joint.
It should be mentioned that residual hip dysplasia secondary to septic hip arthritis is different from that seen in DDH. First, the associated intra-articular fibrosis limits to a great extent the degree of dislocation, yet it limits the range of movement of the hip to the same degree. This will need sharp dissection to free the stuck deformed head and to clear the acetabular fossa adequately before deciding what sort of acetabular reconstruction is needed. Intra-articular adhesions were more pronounced in the beard head cases reflecting less favorable results regarding the range of movement regained. Also, femoral shortening should be adequate in the sense of bringing the femoral head level with the acetabulum. The aim should be easy containment of the reshaped femoral head, regardless of the shortening required. Limb length discrepancy did not comprise a problem and was compensated in most of the cases.
Second, the acetabulum, which is usually normal at birth, will turn to be dysplastic in older children due to the long-standing absence of the femoral head, which, in turn, is no more smooth or congruent due to ischemic necrosis associated with infection. An acetabular defect is usually superior or anterolateral according to the site of impingement of the deformed femoral head. Reconstruction is selected accordingly. A Dega acetabuloplasty was performed in three cases with global defect, while Salter osteotomy was carried out in nine cases when the defect was more anterolateral. Triple pelvic osteotomy was required in two older patients.
Third, the capsule is thick, fibrotic, and adherent, or even amalgamated with the overlying muscles. Meticulous sharp dissection is essential to preserve the outlines of the capsule for later capsulorrhaphy, as dictated by the topography of the head. In the beard head, the capsular cuts should be as such to cover the underlying raw surface of the neck.
Fourth, although extensive dissection was needed to clear the acetabular fossa and to free the stuck deformed femoral head all round for adequate reshaping, avascular necrosis was not met in the current study, even in hips with extensive intra-articular fibrosis. This was attributed to care given to preserve the posterior capsule of the hip carrying the main blood supply to the femoral head.
Plain radiography has shown limited value in classification and, accordingly, decision-making. This was due to a delay in ossification of the dislocated deformed femoral head in young children, besides the restricted rotation that concealed the actual profile of the femoral head and neck in older children. Chang and Huang [8] believed that MRI can reveal the real shape and size of a cartilaginous epiphysis, and suggested a new classification based on MRI findings for better comprehension and comparisons of results. In the current study, MRI investigation was limited to following up the viability of the beard femoral head in four cases.
Multislice CT with 3D reconstruction views were performed in only six cases, yet, it was valuable in providing a panoramic view of the deformed femoral head and, thus, on the expected reconstruction required before the final on-table decision-making.
The proposed reconstruction procedure for reshaping the deformed femoral head (osteochondroplasty) is a salvage attempt that achieved a more or less mobile painless stable hip joint besides restoring the normal anatomical relationship, should total hip replacement (THR) be needed in the future. It appears that better results are achieved in younger children with minimal intra-articular adhesions limiting hip movements, and with less destruction of the articular cartilage.
Footnotes
Acknowledgement
Thanks to Ali Mohamed Massoud M.D., my main assistant in the operating theatre.