
Abstract
Abstract
Aim of the study
We asked whether the ipsilateral knee of patients treated by closed reduction for developmental hip dislocation (DDH) is affected by osteoarthritis (OA) more than 40 years later.
Materials and methods
In total, 61 patients (71 hips) with the diagnosis of DDH were included in the study. The average age at the time of closed reduction was 17.9 months. The follow-up after closed reduction averaged 44.4 years. We determined the following parameters on radiographs, taken in the standing position: minimal joint space width in the medial and lateral compartments of the knee, minimal joint space width of the hip joint, radiological signs of osteoarthritis of the knee and the hip joints (Kellgren and Lawrence), knee alignment, acetabular roof obliquity (AC angle), depth of the acetabulum (ACM angle) and center–edge angle (CE angle) according to Wiberg. All radiographs were measured twice manually with ruler and goniometer by two independent investigators. Interobserver and intraobserver reliability (test–retest) was calculated for all parameters.
Results
We observed that patients with bilateral DDH had significantly more joint space narrowing in the medial compartment of the knee joints than those with unilateral DDH. The length of follow-up correlated with radiological signs of OA in the hip, but not in the knee.
Conclusion
We found a significant difference in medial compartment joint space narrowing between patients with unilateral DDH and those with bilateral DDH. The Kellgren–Lawrence classification, however, showed no significant differences between uni- and bilateral DDH. The knee alignment was always at the threshold of physiological values.
Introduction
It is well known that changes in the mechanical axis around the hip joint influence the alignment and local load distribution of the knee joint [1, 2]. If a deviation of the axis at the hip joint already existed in childhood, lateral compression forces can influence bone growth according to the rule of Hueter and Volkmann, leading to a valgus deviation in the knee joint [1, 3–5]. Former studies demonstrated the influence of a fixed adduction contracture to the physes of the distal femur and proximal tibia [6–8].
Unilateral developmental hip dislocation (DDH) was reported to result in a valgus deformity more often than bilateral DDH [2, 8, 9]. Despite a valgus deformity, more degenerative changes were found in the medial than in the lateral compartment [8].
Deviations of the axis around the knee are likely to be correlated with the degree of hip dysplasia. We therefore conducted the present study to evaluate whether radiological angles and signs of degeneration of the hip correlate with the corresponding parameters of the knee in a long-term follow-up.
Materials and methods
In total, 61 patients (71 hips) with the diagnosis of DDH were included in the study; in 10, both hip joints had been treated. All patients were treated by closed reduction alone [10, 11]. There were 51 females and 10 males. All patients were treated at the University of Iowa Hospitals and Clinics. The treatment consisted of casting for at least 3 months. There had been no difference in treatment regime, casting and after-treatment with respect to unilateral or bilateral affection.
We used the hard copies of radiographs of long-leg axis and of the pelvis in the standing position to determine the following parameters: minimal joint space width in the medial and lateral compartments of the knee, minimal joint space width of the hip joint, development of osteoarthritis [Kellgren and Lawrence classification [12] (Table 1)], knee alignment (tibio-femoral angle), acetabular roof obliquity [AC-angle [13] (Fig. 1)], depth of the acetabulum [ACM-angle [14] (Fig. 2)] and the center–edge angle [CE-angle [15–17] (Fig. 3)] according to Wiberg. The radiographs of both the pelvis and the long-leg X-rays of the treated hip were taken at the same time. All radiographs were measured twice manually with a goniometer by two independent investigators; neither observer was the treating physician. One investigator was an experienced orthopaedic surgeon (S.F.), and the other was a final-year medical student (C.P.). The average age at the time of closed reduction was 17.9 months (SD 14.3, range, 1–96 months). The average age at the time of the first follow-up evaluation was 27.6 years (SD 8.5, range 15–48 years), and at the second evaluation was 45.9 years (SD 8.7, range 33–66 years). The follow-up after closed reduction averaged 27.6 years (SD 8.49, range 15–46.3 years) at the first evaluation and 44.4 years (SD 8.7, range 15–64.3 years) at the second evaluation.
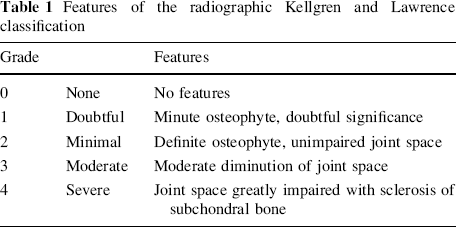
Features of the radiographic Kellgren and Lawrence classification

This radiograph documents the measurement of the acetabular roof obliquity (AC angle) in adults
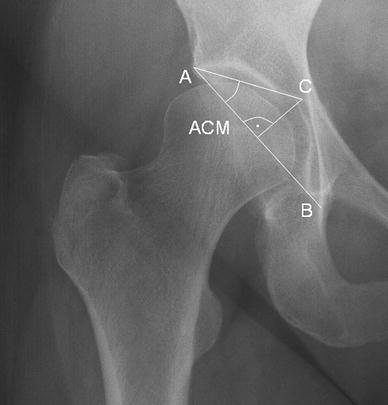
The acetabulum (ACM) angle determines the depth of the acetabulum
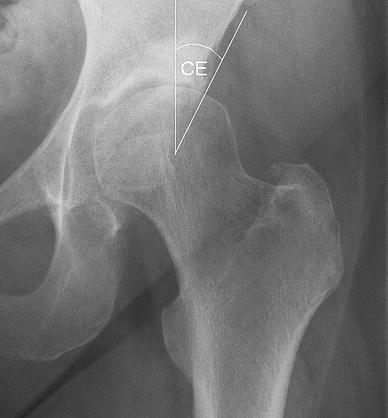
This radiograph demonstrates the measurement of the center–edge angle (CE angle) according to Wiberg
Interobserver and intraobserver reliability (test–retest) was calculated for all parameters. Statistical analysis was performed using the Statistical Package for Social Sciences for Windows, release 11.0 (SPSS GmbH, Munich, Germany). A student's t test for paired samples was done for comparison of the parameters in the same patient at different times and one for unpaired samples was done to compare parameters between groups of patients at the same time. Pearson's coefficient was calculated for determination of correlations.
Results
Intraobserver reliability (test–retest) was calculated for all parameters. Pearson's correlation coefficients between the two measurements were always higher than r = 0.9 (P < 0.001) for examiner 1 (S.F.) and higher than r = 0.86 (P < 0.001) for examiner 2 (C.P.) in all parameters. Thus, we decided to use the average from both measurements of one examiner for further statistics.
Interobserver reliability also was calculated for all parameters. Pearson's correlation coefficients between the two examiners were always higher than r = 0.78 (P < 0.001) in all parameters. Thus, we used the average from both examiners for further statistics. The correlation coefficients of the overall average of each parameter with each single measurement was always higher than r = 0.9 (P < 0.001).
Statistical comparison between patients with bilateral DDH and those with unilateral DDH revealed that the former had significantly more joint space narrowing in the medial compartment of the knee joints (Table 2).
Mean results of the measurements with respect to the knee joint

Comparison of genders showed that female patients had significantly more joint space narrowing in the lateral compartment than males (females 4.2 mm, SD 1.2, n = 42; males 5.7 mm, SD 0.9, n = 8, P = 0.001).
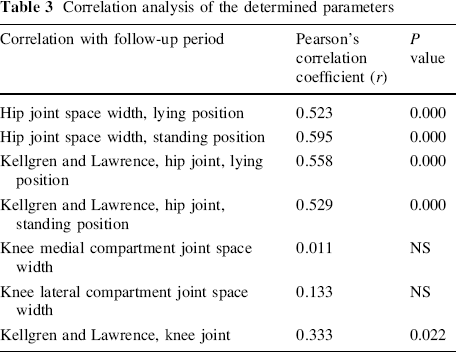
Correlation analysis of follow-up period with radiological signs of osteoarthritis revealed significant correlations in the hip joint, but not in the knee joint (Table 3).
Correlation analysis of the determined parameters
Correlation analysis of hip angles could not show significant correlations to the knee angles and degeneration.
Discussion
In this study we have shown a significant difference in medial compartment joint space narrowing between patients with unilateral and those with bilateral DDH. The latter developed an increased joint space narrowing. The medial compartment was always significantly narrower than the lateral. The Kellgren–Lawrence classification showed no significant differences between uni- and bilateral DDH. The knee alignment was always at the threshold of physiological values. However, it was not pathological and did not differ between uni- and bilateral DDH. In tendency, the tibio-femoral angle was larger in patients with unilateral DDH.
Thus, the tibio-femoral angle and the fact that the medial joint gap was narrower than the lateral are considered physiological. As expected from these results, no correlation of the medial and lateral joint gaps and the tibio-femoral angle with the angles around the hip was found.
The findings of previous studies, that a unilateral DDH results in a valgus deformity of the knee, are supported by our data only in tendency, but not significantly [8, 9]. Also, we cannot significantly confirm more degenerative changes in the lateral compartment, as described by Wedge [7, 8].
Obviously, the mechanical axis of the leg could be restored by early closed reduction in infancy. Therefore, at follow-up, the patients showed no changes in the mechanical axis of the leg or degenerative changes of the knee joint that go beyond an age-compared population.