
Abstract
Abstract
Purpose
The purpose of this study is to define the clinical presentation of adolescent patellofemoral pain.
Methods
A review was completed of all patients with patellofemoral pain at a children's hospital sports clinic over a 3-year period.
Results
One hundred and one patients (91 female) with 136 symptomatic knees were identified. Mean age was 14.4 years. Knee pain was localized to the anteromedial or anterior region of the knee in 96% of patients and was typically produced with running (94%), jumping (92%) and stair use (69%). On physical examination there was usually a non antalgic gait (99%), no patellofemoral crepitation (98%), normal lower extremity angular (84%) and rotational alignment (94%), with no foot malalignment (>97%). The medial patellofemoral ligament (MPFL) was the most palpably tender area of the knee in 98% of patients. During “lateral apprehension” testing, 89% had pain at the MPFL, but not true apprehension. A “J-sign” was present at terminal knee extension in 65%. Mean Q-angle was 18.7°. Means of all radiographic measures were within normal ranges.
Conclusion
The prototypical patient had anterior/anteromedial knee pain of insidious onset during running and jumping. The most consistent physical findings were focal tenderness at the MPFL, positive terminal J-sign, and an elevated Q-angle. Most patients required only nonsurgical treatments, but 18% underwent surgical interventions for persistent pain.
Introduction
Knee pain is a common complaint in the adolescent who presents for evaluation in the outpatient setting. A wide range of possible etiologies of the knee pain exists, ranging from the acute pain of a patellar dislocation or a meniscal tear to the more chronic, indolent pain of Osgood-Schlatter's disease. One of the more common causes in the adolescent female population is “anterior knee pain” or adolescent patellofemoral pain, which has also been referred to in the literature as patellofemoral maltracking, lateral patellar compression syndrome, patellar instability, retinaculitis, excessive lateral pressure syndrome, and chondromalacia patellae [1–6]. When compared to other intra-articular knee problems, such as anterior cruciate ligament or meniscal tears, little novel information exists to aid the clinician in the diagnosis and treatment of this enigmatic problem. Many of the published reports on anterior knee pain have included adolescent and adult patients, which diminishes the application of each studies’ findings to the diagnosis and treatment of patellofemoral pain in adolescents.
Unlike many diagnoses of the knee, there is no classic, distinguishing physical or radiographic finding which can be used to identify the problem. The absence of a unique physical finding makes the firm diagnosis of patellofemoral pain extremely challenging, and renders it essentially a diagnosis of exclusion [7–9]. Most of these patients have pain which is localized to the peripatellar or retropatellar areas and is usually vague in nature [10]. As Dye states “patients with patellofemoral pain often have no identifiable objective abnormality” [11]. Several well-written clinical and literature reviews have aided in establishing a framework on this subject, but the precise presentation of the adolescent with “anterior knee pain” has not been described [8–10, 12]. The etiology remains unknown. The purpose of this manuscript is to more precisely define the clinical history, physical examination, and radiographic findings of medial patellofemoral pain (MPFL).
Materials and methods
A review was completed of all patients (0–18 years of age) with patellofemoral pain presenting for outpatient evaluation to a pediatric sports clinic at a tertiary-care children's hospital over a 3-year period. Patients were excluded if their knee pain was from a non patellofemoral source, there was a history of patellar dislocation or subluxation episodes, previous knee surgery, or patellar osteochondritis dissecans (OCD). In addition peripatellar or other anterior knee diagnoses, such as patellar tendonitis, Jumper's knee (Sinding–Larsen–Johannsen disease), Osgood–Schlatter's disease, saphenous neuritis, fat pad syndrome, collateral ligament pathology, bipartite patellae, Hoffa's disease [13] and patellar fractures/nonunions were not included in this analysis. There was no minimum follow-up for this descriptive study as its purpose was to describe the presentation of patellofemoral pain. Hence surgical treatment for patellofemoral pain is not the focus of this manuscript. Outpatient records and radiographs were reviewed for all patients. Data collected included: age, gender, side of involvement, length of symptoms, analgesic use, knee brace use, history of antecedent trauma, subjective location of knee pain, provocative activities (walking, running, jumping, stair climbing, sitting/squatting), mechanical and instability symptoms, and history of knee swelling or effusions. Previous therapeutic interventions were documented, specifically use of patellar braces, physical therapy sessions, at-home exercises, and medication use. When available, International Knee Documentation Committee (IKDC) subjective scores were obtained and recorded.
Physical examination of the lower extremity included analysis of gait for antalgia, foot progression angle and dynamic lower extremity rotational attitude. Standing evaluation documented gross rotational and angular alignment, limb length discrepancy by block testing, and foot alignment. In addition, lower extremity rotational alignment of the tibia and femur was assessed in the prone position with the hip in extension and the knee flexed at 90° [14]. Radiographic imaging studies to document rotational alignment (i.e., CT scans) were not obtained. Patients were examined in the prone position Knee examination data included assessment of patellofemoral crepitation, terminal J-sign, quadriceps angle, location of palpable tenderness (maximal and any tenderness), effusion, lateral apprehension sign, ligament/meniscal testing, and muscle contractures (hamstrings, quadriceps, iliotibial band). Terminal J-sign is a dynamic test performed with the patient in the seated position. As the patient actively extends the knee, the patella has a lateral coronal shift of the patella when the patella disengages from the femoral trochlea. The classic patellar compression test is routinely performed for detection of patellofemoral crepitation only. During performance of this test the examiner applies pressure to multiple potential pain generators, hence it is not useful in the precise identification of pain generators. The quadriceps or “Q” angle was measured with the patient in the supine position with the knee flexed between 20 and 30° in order to engage the patella in the femoral sulcus. A large goniometer was centered over the patella with one limb over the tibial tubercle and the other in line with the anterior superior iliac spine. Medial and lateral patellar glide were assessed at 20°–30° of knee flexion. On medial patellar glide the lateral restraint was classified as “tight” if there was ≤1 quadrant of mobility and “hypermobile” if ≥3 quadrants of mobility. On lateral glide, normal level of restraint was defined as 0.5–2 quadrants of mobility, and “incompetent” defined as ≥3 quadrants. Lateral patellar apprehension testing was performed at 20° of knee flexion, with special note made to patient's report of apprehension, pain or both.
Routine radiographic analysis for all patients consisted of standing anteroposterior (AP), lateral, notch and Merchant's view radiographs [15]. Measurements were measured directly from the radiographs: Insall/Salvati ratio, Blackburne–Peel ratio, sulcus angle, congruence angle, lateral patellofemoral angle and lateral patellar deviation. Normal ratios for the Insall–Salvati (IS) ratios have been previously reported for boys to be 1.03 ± 0.11, and for girls 1.06 ± 0.11 [16]. IS ratios for normals (boys and girls) has also been reported to be 1.17 ± 0.16 [17]. Blackburne–Peel ratios in normal knees are a mean 0.97 ±0.23 with 95% confidence limits of 0.87–1.06 [17]. Normal sulcus angles have been reported to be 138 ± 6°, and congruence angles to be −6 ± 11° [18]. Normal lateral patellofemoral angle and lateral patellar deviation have been reported as 12.0 ± 5° and −1.0 ± 2.5 mm, respectively [17].
After ruling out other etiologies of knee pain and establishing a working diagnosis of MPFL pain, the initial management of the adolescent is nonsurgical. Treatment goals are to relieve pain, stretch contractures, strengthen weak musculature (core and lower extremity), and to attain function balance of the quad musculature. Activity modification was recommended to all patients to decrease supraphysiologic loading, minimize aggravating activities of daily living and pain, and to increase likelihood the exercises would be able to be performed painlessly [19]. Over-the-counter analgesics were recommended only for symptom control, no scheduled dosing of analgesics was advised routinely. At the first outpatient visit, an at-home physiotherapy program is started after 1–2 visits to a physical therapist in order to teach the correct exercise mechanics. The protocol consists of a strengthening and stretching program while maintaining a pain-free state during the exercises. Strengthening exercises emphasized closed-chain exercises of steps and mini-squats, in addition to straight-leg raises, short-arc quads (maximal flexion of 30°), and quad isometrics. Stretching of contracted musculotendinous groups consisted of the hamstrings, quadriceps, and iliotibial band. All patients were instructed on the necessity of performing exercises for a minimum of 6 months, and more than three times per week, as long as the individual is athletically active. Patients were instructed to follow-up in the outpatient clinic if their knee symptoms were unsatisfactory at a minimum of 2 months after the first visit (Fig. 1).
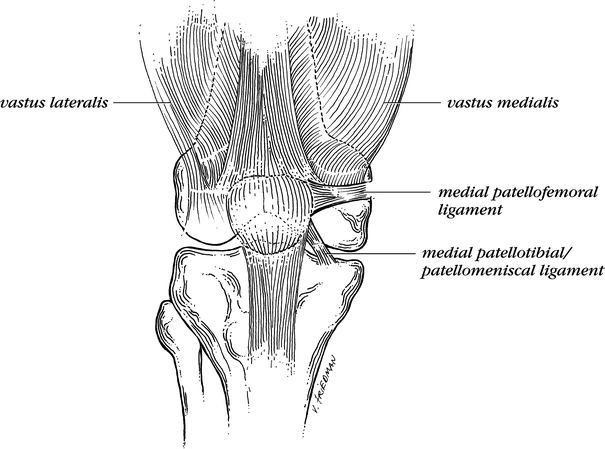
Drawing of the medial patellar restraints. The MPFL is usually localized at the mid-point of the patella and can be traced to the medial epicondyle
The failure of the knee symptoms to improve adequately prompted patient return for follow-up evaluation to confirm the diagnosis MPFL pain, and to document any changes in the physical examination. After failure of the at-home program, a formal program of physiotherapy was recommended for a minimum of 6 weeks (two visits per week) at a physical therapy facility. A structured program was instituted with supplementation of McConnell taping, retinacular stretching, foot orthotics, electrical stimulation, ice therapy, phonophoresis and iontophoresis as directed by the physical therapist. The physiotherapy is individualized to assure stretching of all contracted or tight structures and to balance the kinetic chain by strengthening. If the MPFL pain continued despite following the above-mentioned protocol, the patient was instructed to return for a third outpatient evaluation at a minimum of 2 months after the second evaluation. If MPFL pain was reconfirmed (after a total of three separate outpatient evaluations) with pain centered at the MPFL, discussions about the patient's therapeutic options typically included arthroscopic lateral retinacular release. The failure of nonsurgical techniques to adequately relieve the MPFL pain, by patient assessment, is a relative indication for surgical intervention. Arthroscopic lateral retinacular release (ALRR) was performed only for recalcitrant pain centered at the MPFL. This is the only indication for ALRR, if the patient's history or physical examination was atypical then further imaging (magnetic resonance imaging) was performed to rule any identifiable intra-articular pathology which may be the pain generator. Patients and families were, and always should be, instructed the ALRR did not obviate the need for continued physiotherapy, but rather was an adjunctive procedure to permit the individual the ability to perform more effective physiotherapy by decreasing the intensity and/or frequency of anterior knee pain.
Results
Medical records search identified 101 patients (91 female, 10 male) with 136 symptomatic knees whose mean age was 14.4 years (9.0–19.1 years). Median length of symptoms was 16.9 months (1 week to 5 years). The mean subjective IKDC score at the time of the initial evaluation was 42.6 (18–82). The right knee was involved in 32 patients, left in 34 and both in 35. Prior to the first outpatient evaluation, 29% (29/101) of patients had used a knee brace and 51% (52/101) used analgesics for pain control. Only 20% (20/101) recalled an acute onset of their patellofemoral pain. The anterior knee pain was typically produced with running (94%, 128/136 knees), jumping (92%, 125/136), and stair use (69%, 94/136). Only 32% (44/136) of the knees had pain with prolonged knee flexion or the classic “theater sign”. Overall, 32% (44/136) of knees had mechanical symptoms. Patients localized their knee pain to the anterior or anteromedial aspect of the knee in 96% (131/136) of the knees.
On physical examination the prototypical patient had a nonantalgic gait (99%, 100/101), no patellofemoral crepitation (98%, 133/136), normal lower extremity angular (84%, 114/136) and rotational alignment (94%, 128/136), with no excessive hindfoot valgus (99%, 135/136) or flatfoot posture (97%, 132/136). The classic “J-sign” was present at terminal knee extension in 65% (88/136), and mild lateral retinacular tightness with a mean medial patellar glide of 1.2 quadrants (≤1 = tight, ≥3 = hypermobile). The location of maximal tenderness was: medial patellofemoral ligament (MPFL) only in 62%, MPFL and medial retinaculum in 23%, medial retinaculum only in 7%, MPFL and medial patellotibial ligament in 6% and medial patellotibial ligament only in 2%. Overall, the MPFL was the most palpable tender area, either in isolation or with other structures, in 98% (133/136) of all patients. Palpable tenderness over the lateral retinaculum was identified in 13% of patients and was never the most palpably tender area. Performance of the laterally directed apprehension testing elicited pain at the MPFL, but not apprehension, in 89% (121/136) of knees. The mean Q-angle was 18.7° (10–26°), with 95% having Q-angles greater than 15°. Mean popliteal angle (hamstring tightness) was 28.2° (range, 5–80°) for the 85 knees in which the measurement was recorded.
Analysis of radiographs demonstrated 50% (68/136) of all knees had open physes. The mean Blackburn–Peel ratio was 0.93 (range, 0.59–1.36) and the mean Insall–Salvati ratio was 1.17 (0.82–1.49). Measurements of the patellofemoral joint documented the mean sulcus angle to be 134° (116°–146°), mean congruence angle −2.2° (−28° to 18°), mean lateral patellofemoral angle 11.7° (−7° to 25°), and mean lateral patellar deviation of −2.3 mm (−11 to 10 mm). All of these measurements were within the previously mentioned normal ranges.
Management of this study cohort was nonsurgical in 82% of patients. Surgical procedures were performed in 18 patients (18%) with 26 knees (19%), which consisted of 26 first-stage ALRR, and 2 second-stage tibial tubercle osteotomies. At the time of arthroscopic evaluation of the 26 knees, no other pathologic process was identified to explain their pain (i.e., meniscal tear, patellofemoral chondrosis, patellar OCD lesions, etc.…). No pathologic medial plicas were documented during arthroscopies and no plicas were resected. In addition, during the study period and the data collection period no patient, regardless of treatment type, was determined to have another cause of their anterior knee pain beyond the MPFL-derived pain. As the focus of this study is on the presentation of MPFL pain, the outcomes of ALRR are not presented but are being investigated in a continuing study to be completed in the near future.
Discussion
Over the last 10 years a significant number of studies have been published on anterior knee pain in the pediatric and adult population. Unfortunately for our patients this problem still remains an enigmatic problem to diagnose and treat. Based on the current literature, we are not any closer today to having a cohesive concept on diagnosis and treatment than we were 10 years ago. Because a precise definition of patellofemoral pain has not been accepted, it has become a “catch-all” diagnosis with many published reports having included patients with patellar instability (subluxations and dislocations), patellar chondromalacia (osteochondritis desiccans) and other pathologies. In addition, this diagnosis carries many different labels: patellofemoral maltracking, lateral patellar compression syndrome, patellar instability, retinaculitis, excessive lateral pressure syndrome, and chondromalacia patellae [1–6]. This is, in part, due the lack of a unique distinguishing clinical or radiographic feature that can be tested or quantified to differentiate it from other intra-articular processes. Despite the volumes of literature on this topic, the presence of heterogenous patient cohorts with many different diagnostic descriptors has confused this diagnostic entity more than clarifying it. By using the previously published literature reviews on this subject, the current manuscript hopes to use this base of knowledge to introduce a new concept that is that the MPFL is the main pain generator in adolescents with anterior patellofemoral knee pain.
When one scrutinizes the published literature on patellofemoral pain, there is some obvious overlap with the findings presented in this study. Patellofemoral pain, and MPFL pain, is more common in females, and a history of a direct injury to the knee is present in the minority of patients [4, 20, 21]. Spontaneous or insidious onset of pain can be related to underlying malalignment or an overuse of retinacular structures in the anterior knee [8]. Two classic findings for anterior knee pain have been the “theater sign” or pain with prolonged knee flexion and pain with stair climbing, both of which has been reported to be present in up to 92% of individuals [5]. In the present study we documented the “theater sign” in 32% of knees and pain with stair climbing in 69% of knees. This difference may be attributable to our cohort being exclusively adolescents. Interestingly, the most consistent provocative activity for our patients was pain with running (94%) and jumping (92%) in physical education class and/or sporting activities, with little pain during normal walking activities. The absence of patellofemoral crepitation on physical exam is corroborated by the lack of patellofemoral chondrosis documented at the time of arthroscopy in the 26 knees with severe, recalcitrant MPFL pain. As documented in this study there was a relative absence of any articular cartilage damage or clinical patellofemoral crepitation, making the “chondromalacia patellae” diagnosis inappropriate. Is the actual diagnosis for our patient cohort OCD of the patella (POCD)? The answer is no. Schwarz reported the outcome of operative treatment in 31 patients with POCD [22]. There was a male:female predominance of 9:1, preoperative patellofemoral crepitation in 74% and effusion in 45%. All patients had identifiable lesions on the patella (52% midline, 22% inferior and 15% superior) on preoperative radiographs and documented at the time of surgery. In addition, loose bodies were removed in 42% of patients. Additionally, Royle reported on 500 knee arthroscopies and documented patients with patellofemoral pain had only a slightly higher incidence of macroscopic chondromalacia than to those with no patellofemoral symptoms [23]. He also documented chondromalacic changes on the patella occur in a significant proportion of normal knees, probably approaching 40%, even in young patients, and the presence of retropatellar changes has a poor correlation with clinical picture. Based on the author's experience, patients with patellofemoral crepitation most commonly have patellofemoral chondrosis due to patellar OCD lesions, patellar subluxation or dislocation or trauma.
Several previously published studies have demonstrated the association of patella alta, shallow sulcus and lateral subluxation with anterior knee pain [17, 24, 25]. However, as shown by this study and other studies, due to the lack of any significant radiographic findings, patellofemoral pain is mainly a clinical diagnosis dependent upon an accurate physical examination [6, 10, 26]. Historically a major problem with developing a “prototypical” patient profile for patellofemoral pain is the confusion around the clinical examination, specifically the precise location of the knee pain. Some authors describe diffuse anterior knee pain [3, 27], while others describe anterolateral pain [21, 28], anteromedial pain [4, 29–31], or both [2, 5, 32]. A common maneuver performed during patellofemoral joint evaluation is the patellar compression test, whose conceptual purpose is to identify patellar pain by manually compressing the patellofemoral joint [4, 30–33]. It should be emphasized the lack of uniformity on the performance of the test makes it less than ideal as a stand-alone test since this applies diffuse pressure to a wide area of the anterior knee and to multiple peripatellar structures, all of which are well-innervated and capable of being pain generators of the knee [19]. In this study, all the patients had a very consistent physical finding, pain centered at the MPFL at the anteromedial knee, either in combination with other structures or in isolation. It should be emphasized that identification of the MPFL on physical examination requires fingertip palpation of the anteromedial knee. The MPFL is located 2 cm proximal and parallel to the medial tibiofemoral joint line, and is often mistaken as a medial plica or a possible medial meniscal tear.
The MPFL has been demonstrated to be an important medial stabilizer of the patellofemoral joint [34]. Cadaveric dissection studies of the patellofemoral ligaments have documented 90–100% of cadavers have an identifiable MPFL, which lies in the middle fascial layer with an average width of 1.3 cm [35–39]. Two ligament cutting studies reported the MPFL is responsible for 50–53% of the medial patellar restraints, with the patellomeniscal and patellotibial ligaments contributing another 25–27% of the overall restraint [35, 37]. These two medial restraints are most important in the first 30° of knee flexion, after which the bony anatomy (lateral femoral trochlea) plays an increased role in patellar stability [40]. Furthermore, MPFL reconstruction has demonstrated the restoration of normal patellar stability after its transaction in cadavers [41]. The importance of the MPFL as an main stabilizer on the medial side of the patella is in distinct contrast to the lateral patellofemoral restraints, of which the vastus lateralis obliquus is the main stabilizer in 47% of knees, the anterior fibers of iliotibial tract in 16%, lateral retinaculum in 5% and all three in 32% [5]. A lateral patellofemoral ligament has been described, however its importance biomechanically is unknown [42].
In 1982, Fulkerson was one of the first to draw attention to the retinaculum as the painful tissue in patellofemoral patients, with later studies supporting this view [3, 26]. He further described, as have others, the early patellofemoral pain in many young people appears before evidence of patellar chondromalacia [32]. Insall and Falvo pointed out the pain was along the medial joint line, which frequently caused confusion with potential meniscal lesions [4]. They assumed pain was secondary to synovial inflammation; however, at the time of surgery, the synovium was found to be normal both grossly and histologically. Fulkerson in a subsequent study published in 1983 commented, “early patellofemoral pain appears in many young patients before there is gross evidence of chondromalacia on clinical examination of arthroscopy. This pain appears to be primary retinacular, from overuse, whereas pain that occurs in other, usually older, patients in conjunction with obvious chondromalacia may be entirely different.” [2].
The etiology for anterior knee pain has been well-described, but our hypothesis is the most likely cause of MPFL-derived pain described in this study is due to a mild degree of patellofemoral malalignment [43]. Ideal function of the patellofemoral joint is predicated on the presence of balanced medial and lateral patellar restraints [44–46]. In that MPFL pain is uncommon until the adolescent growth spurt, rapid growth likely causes a mild imbalance in these restraints, and the relationship of the quadriceps to the hamstrings and the vastus medialis to the vastus lateralis [5, 20, 21, 47, 48]. As stated by Fulkerson “While opinions vary, there is little question that imbalance (malalignment) of the extensor mechanism can lead to overload of the retinaculum and subchondral bone. The result of patellofemoral imbalance or injury is activation of nociceptive (pain) fibers in the bone, synovium, or retinaculum, which results in pain” [8]. Our cohort had a mean medial patellar slide was 1.2 quadrants, which is a mild tightness/contracture of the lateral retinaculum. The asynchronous forces across the patellofemoral joint increases the stresses at the patellofemoral joint in the young, active individuals, thereby causing retinacular pain. These restraints can undergo significant strains with increasing knee flexion, at 30° of knee flexion the force required to stabilize the knee increases to 210% of body weight [47]. It has also been speculated that, in addition to their biomechanical properties, the ligamentous structures provide proprioceptive signals to the surrounding musculature, which can help explain the symptoms of “buckling” or “giving way” of the knee joint in the form of a negative reflex arc [4, 19, 49, 50]. The innervation of the anterior knee joint has demonstrated a rich neural supply consisting of substance-P nerve fibers, Ruffini-type receptors and free nerve endings in the medial and lateral retinaculum [26, 50–53]. In addition, Sanchis-Alfonso et al. [54] reported the proliferation of nociceptive axons in the perivascular retinacular tissues in patients undergoing patellar realignment surgery for anterior knee pain. These findings have lead to the hypothesis development that chronic retinacular injury and ischemia due to tension overload may induce pain and pathologic neural development [7]. This may also explain why patients with long-standing patellofemoral pain respond less to physiotherapy than those with symptoms of shorter duration.
Devereaux et al. reported an elegant thermographic study on the patellofemoral joint in patients with activity-induced retropatellar pain without radiographic abnormalities or chondromalacia patellae on arthroscopy [28]. In their cohort 28 of the 30 patients had increase in heat on the medial side of the patella, corresponding to the site of tenderness with radiation into the vastus medialis muscle. Interestingly 6 individuals showed contralateral increase in heat in the asymptomatic side, which was less than symptomatic side. They hypothesized the patellofemoral arthralgia was due the vastus medialis becoming over stretched by overdevelopment of the vastus lateralis. With physiotherapy and muscle stimulation all patients became asymptomatic at 3 month follow-up, and thermographic findings disappeared. The aforementioned patellofemoral studies describing ligamentous anatomy, biomechanics, and innervation all lend support to the clinical presentation of patellofemoral pain presented in this patient series and the role of the MPFL as a pain generator. It is important to note we are not describing lateral impingement pain at the patellofemoral joint. As demonstrated in this cohort 98% had anteromedial pain with palpable tenderness over the lateral retinaculum was identified in only 13% of patients and was never the most palpably tender area. It is theoretically possible that the initial presentation of patellofemoral pain, that is medially derived pain at the MPFL, later transitions to more diffuse anterior or possibly lateral-based pain which has been described for those patients with “lateral patellar compression syndrome”.
The natural history of MPFL pain is unknown, but there is a commonly held belief by clinicians that anterior knee pain of adolescents “does not necessarily or even routinely lead to a lifetime of pain or arthritis.” [12]. One report frequently cited as proof that patellofemoral pain is a benign, self-limited condition that can be treated nihistically was published by Sandow and Goodfellow [55]. Their report documented the natural history (mean follow-up of 3 years 8 months, range of 2–8 years) of a group of 54 untreated girls with patellofemoral pain without obvious pathology. Closer examination of their results does not seem to support their findings, which are specifically “the policy of non-intervention which we had followed is justified and that surgical treatment need seldom be considered”. They demonstrate 94% of patients still had anterior knee pain, at final evaluation, which was of the same severity or worse in 54%. Fifty percent of patients had at least weekly pain with occasionally or severely restricted sporting activities and over 50% of patients had persistent problems with stair climbing and walking. Fujimoto reported on 98 girls with patellofemoral pain whose mean age at diagnosis was 13 years with 7-year mean follow-up [56]. All had a diagnostic arthroscopy which confirmed a normal patellofemoral joint or only slight chondromalacia. At final follow-up 76 of 98 (78%) patients reported still having pain with 67.4% (66/98) had improvement in pain, but 30.6% (30/98) still had pain, though only 2% (2/76) were worse. Blond and Hansen reported on 250 athletes with patellofemoral pain with 73% (182/250 patients) still suffering anterior knee pain at an average 5.7 years follow-up [57]. Of those with persistent pain 95 (52%) had a decrease in their pain, while 64 (35%) were unchanged and 23 (13%) experienced an increase in pain. 68 (37%) described the pain as mild, 88 (48%) as moderate, and 26 (15%) as severe. Athletic activity was affected in 184 (74%). These papers are often quoted to support the benign nature of patellofemoral pain over time, however, as stated in these 3 papers, 33–95% still had pain which was severe enough for them to seek medical care (and even arthroscopy). If the outcome of other surgical procedures of the knee, such as total knee arthroplasty or anterior cruciate ligament reconstruction, had such poor results it is unlikely these procedures would be advocated by many orthopaedic surgeons or accepted by our patients. Should the clinician be satisfied with these numbers?
The treatment regimen utilized at our institution for MPFL pain was developed incorporating the concepts forwarded in earlier studies [2, 3, 58–60]. The effectiveness of nonoperative treatment regimens have been reported to be up to 80%, which is supported by our findings [2, 3, 58–62]. It is well known the use of quadriceps exercised improves strength, however, the mechanism for the positive effects is not clear (47–49, Crossley). The focus of the therapy is to restore the “patellofemoral load acceptance capacity” by the elimination of supraphysiologic loads and aggravating activities, anti-inflammatory modalities (NSAIDs and cold therapy), and rehabilitation [10, 11]. It is important to note that not all patients in this series, and in the studies reported by Sandow and Stathopulu, fared well with nonoperative interventions (18% eventually underwent arthroscopic lateral release). The mechanism for pain relief after lateral retinacular release remains an unanswered question [26, 63, 64]. Though beyond the scope of the present study, there is support in the literature for the use of lateral release for patients with anterior knee pain who have failed nonoperative treatment [2, 3, 5, 15, 26, 32, 63, 65–76, 77].
Conclusion
To develop a comprehensive approach to the treatment of anterior knee pain it is essential to establish an accurate diagnosis. The aim of this study was to lay the groundwork for establishing the diagnosis of MPFL pain by reporting a reproducible and distinguishing clinical characteristic, specifically pain over the MPFL. The description of the prototypical patient, specifically anterior or anteromedial knee pain of insidious onset, pain with running and jumping, focal tenderness at the MPFL with palpation and with lateral “apprehension” testing, an elevated Q-angle and positive terminal J-sign with normal knee radiographs, will ideally help not only in the treatment of our patients but also to further research in this area by creating more homogenous patient cohorts.