
Abstract
Purpose:
The purpose of this study was to assess the ability of radiographic measures to predict displacement on computed tomography (CT) for transitional ankle fractures.
Methods:
This study is a retrospective review of pediatric patients who presented with Tillaux (Salter–Harris III) and triplane (Salter–Harris IV) fractures at a single institution. Radiographs and CT measurements were performed by three independent evaluators. Intraclass correlation coefficients (ICCs) were calculated to determine interrater reliability. Spearman correlations were performed to assess the correlations between each radiographic parameter and CT measurements.
Results:
A total of 61 patients were included in this study. The average age of patients was 12.3, and 65.6% of patients were male. There was an almost even split of triplane (55.7%) and Tillaux (44.3%) fractures. Overall, measurements showed at least good interobserver agreement (ICC >0.6). Radiographic anteroposterior view showed the least reliable measurements compared to the mortise and lateral views. There was significant correlation between CT displacement and the following measures on radiographs: tibiofibular clear space on the mortise view (ρ = 0.27, p < 0.05), articular displacement on the mortise view (ρ = 0.35, p < 0.01), articular displacement on the lateral view (ρ = 0.28, p < 0.05), and epiphyseal displacement on the lateral view (ρ = 0.55, p < 0.001).
Conclusions:
There are several radiographic parameters that significantly correlate with increased displacement of transitional ankle fractures on CT. Increased articular displacement on the mortise and lateral view, as well as increased tibiofibular clear space on the mortise view, correlates with increased displacement. These radiographic parameters may be good indicators for the selective use of CT scans for transitional ankle fractures.
Level of Evidence:
Level III, retrospective comparative study.
Introduction
Ankle fractures are the most common lower extremity physeal injury in pediatric patients, accounting for 15%–20% of all physeal injuries in children.1,2 Tillaux (Salter–Harris III) and triplane (Salter–Harris IV) fractures are transitional ankle fractures that occur in adolescents and are commonly caused by supination with external rotation. 3 Given their articular nature, these injuries may predispose patients to post-traumatic arthritis at younger ages.3 –5 Due to the severity of this significant long-term complication, much focus has been devoted to refining the diagnostic criteria for surgical intervention.3,6,7
While radiographs are used to diagnose triplane and Tillaux ankle fractures, computed tomography (CT) scans are also commonly added to delineate the fracture pattern and degree of displacement, especially at the articular surface. 8 Current guidelines recommend operative intervention for fractures with >2 mm of articular displacement.3,9,10 Preoperative CT imaging assesses the degree of articular surface displacement, fracture pattern, and number of fracture fragments at a higher level of accuracy than conventional radiographs.1,11 However, CT imaging in pediatric patients has been associated with an increased lifetime radiation and cancer mortality risk when compared to CT scans performed in adults.12,13 Moreover, CT imaging incurs a significantly greater financial burden on hospitals and patients compared to radiographs, thus highlighting the critical need for prudent diagnostic decision-making in assessing these fractures.14,15
Despite the risks and concerns of CT, numerous studies have argued for its necessity in addition to plain radiographs to manage triplane and Tillaux fractures.16 –18 Yet, other studies have shown that the addition of CT scans only minimally affected treatment decisions.19,20 Further, Greenhill et al. 8 recently demonstrated that although radiographs alone underestimated articular displacement, metaphyseal displacement >1 mm on lateral radiographs served as a useful predictor for operative levels of articular displacement on CT for triplane ankle fractures. These studies emphasize that due to the rarity and small sample sizes of triplane and Tillaux fractures, the criteria for adding CT versus only utilizing radiographs in these fractures remain clinically ambiguous and controversial. 21 Reliable radiographic predictors of displacement may allow surgeons to selectively utilize CT imaging in pediatric patients.
In this study, we sought to assess the ability of various radiographic measures to predict displacement on CT for transitional ankle fractures. We hypothesized that there would be multiple radiographic measures that reliably and significantly correlate with the articular displacement measured on CT imaging for triplane and Tillaux fractures.
Methods
Study design
This was a retrospective review of pediatric patients who presented with distal tibial Salter–Harris III and IV fractures at a single institution between October 2015 and November 2022. Patients aged 18 or younger with both radiographic and CT imaging at the time of presentation were included. We excluded patients with concomitant lower extremity fractures. Corresponding International Classification of Diseases-10 diagnosis codes were utilized to select all possible patients with Tillaux or triplane fractures (Supplemental Appendix 1). This initial set of patients was screened to confirm the diagnosis of Tillaux or triplane fracture via chart review (Figure 1). A chart review was also performed to collect demographic data such as age, sex, and payor, as well as the mechanism of injury and management. This study was reviewed and approved by our institutional review board.
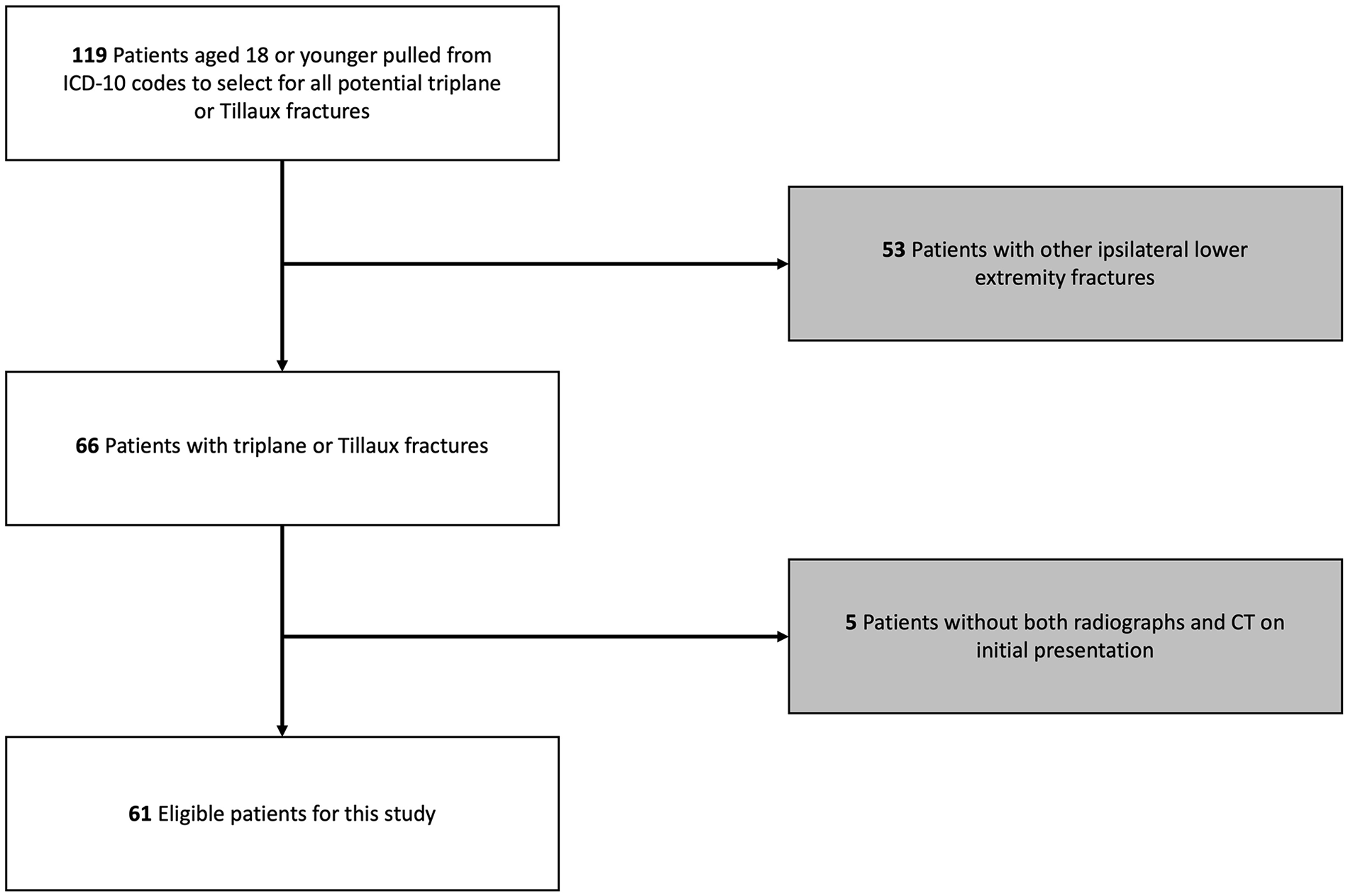
Flow diagram of inclusion and exclusion criteria for final patient cohort.
Radiographic and CT measurements
Measurements were performed by three independent observers (LS, AY, and KB) with various levels of training. Before data collection, each observer performed representative CT and radiographic measurements under the guidance of a fellowship-trained pediatric orthopaedic surgeon (IS) to improve accuracy. The full set of measurements was performed independently by each observer, and they were blinded to the measurements performed by others. All measurements were performed on imaging obtained at the presentation. Measurements were made on the ankle radiographs (mortise, anteroposterior (AP), and lateral views) obtained before CT imaging. These images were calibrated, and measurements were made in millimeters. The specific radiographic measurements included medial clear space, superior clear space, tibiofibular clear space, tibiofibular overlap, articular step-off/displacement, and epiphyseal displacement (Figure 2). CT measurements were performed in millimeters and included maximum diastasis at the articular surface and articular step-off/displacement. Axial, coronal, and sagittal CT views were utilized to identify the maximum measurement. A cut-off of ≥2 and <2 mm was also noted on CT measurements based on current guidelines indications suggesting surgical intervention for fractures with displacement of at least 2 mm.3,22,23 Mean radiograph and CT measurements were calculated from the three sets of measurements and utilized for the analyses.

Representative radiographic and CT measurements.
Statistical analysis
Descriptive statistics were used to summarize patient demographics and imaging measurements. Intraclass correlation coefficients (ICCs) as a two-way random-effects model for absolute agreement were calculated to determine the amount of interrater reliability for each measurement parameter. As previously described, ICCs were categorized as: poor (<0.4), fair (0.40–0.59), good (0.60–0.74), and excellent agreement (>0.75). 24 Spearman correlations were performed to determine the correlations between each radiographic parameter and CT measurements. Significance was considered when p < 0.05. All analyses were performed using Stata 18 (StataCorp. LP, College Station, TX, USA).
Results
A total of 61 patients were included in this study who had either triplane or Tillaux fractures and both radiographic and CT imaging at the time of presentation. The average age of our population was 12.3 years old (SD: 2.2), with the majority being male (65.6%; Table 1). The most common mechanism of injury was fall (68.9%), followed by sport-related injuries (27.9%). There was a close to even split of triplane (55.7%) and Tillaux (44.3%) fractures, with more patients receiving surgical intervention (59.0%) than not (41.0%). Twenty-six (42.6%) patients had closed reductions attempted before their CT scan.
Demographics.
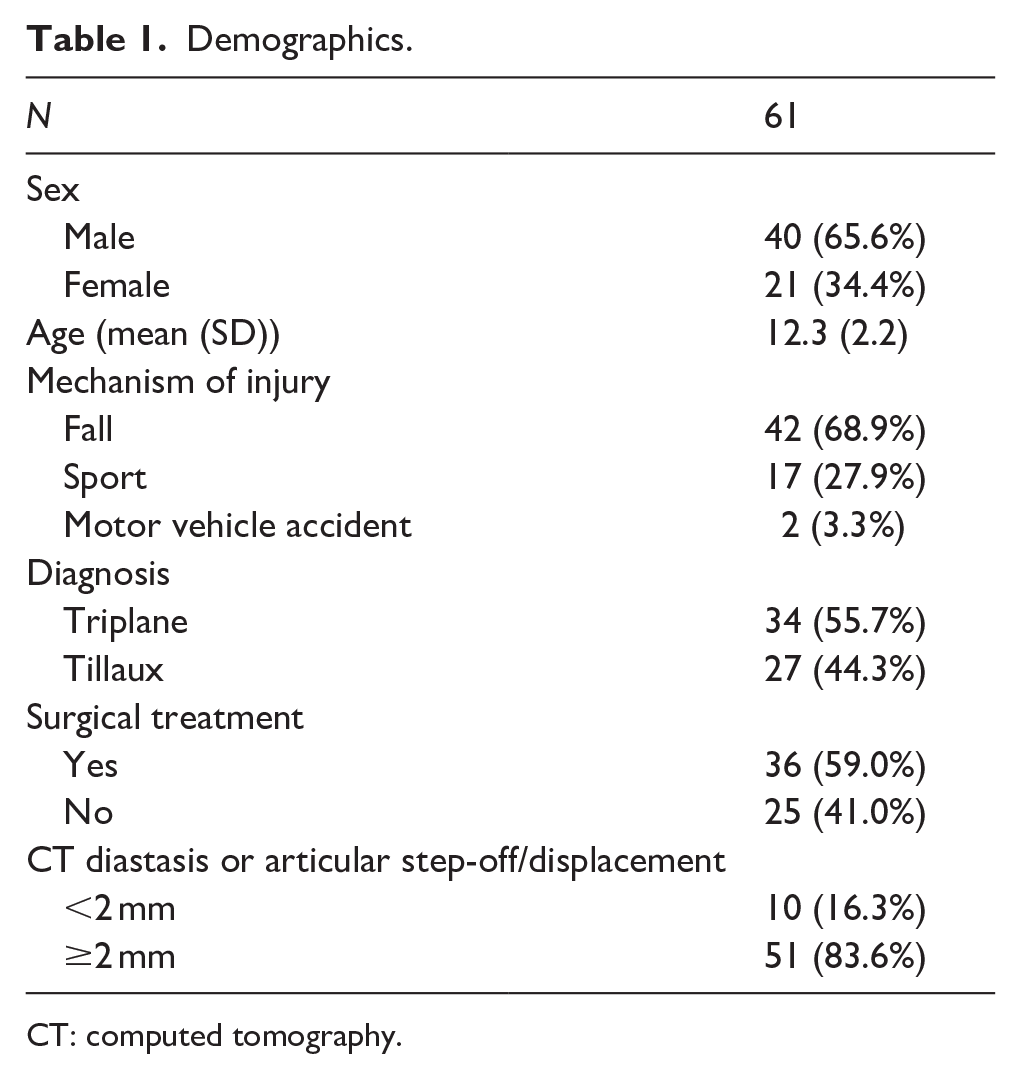
CT: computed tomography.
Interrater reliability
Overall interrater reliability, calculated by ICC, showed mainly good and excellent agreement. Of the 15 radiographic and CT parameters gathered, 12 of them showed at least good agreement with an ICC >0.6 (Table 2). Mortise view had multiple parameters with excellent agreement, such as superior clear space (0.81) and tibiofibular overlap (0.83). There were two measurements with poor agreement, which were both on the AP view (medial clear space: 0.33; superior space: 0.24).
Interrater reliability.
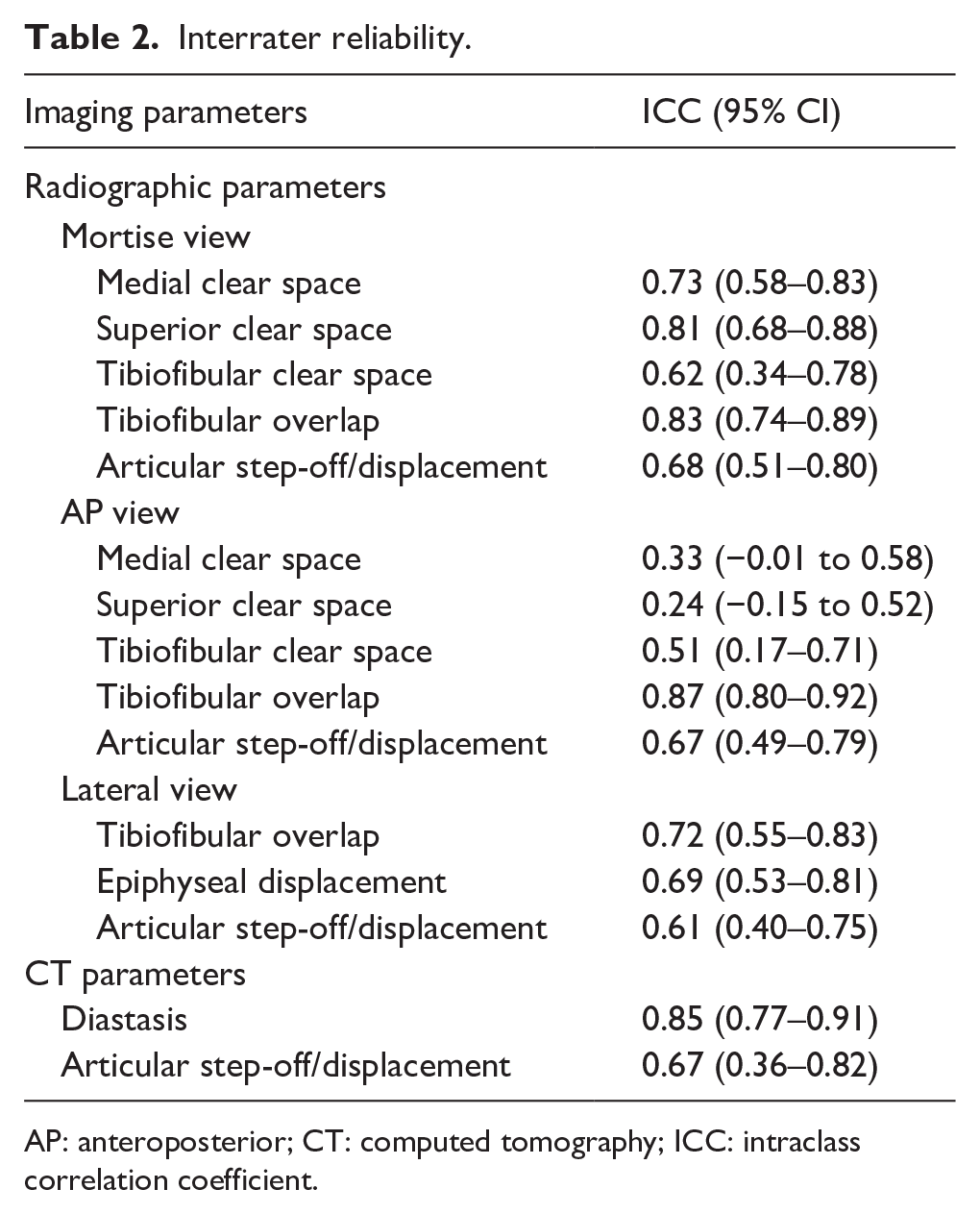
AP: anteroposterior; CT: computed tomography; ICC: intraclass correlation coefficient.
Radiograph and CT mean measurements
Mean measurements for each radiographic and CT parameter are listed in Table 3. In the mortise view, the average articular step-off/displacement was 0.91 mm (SD: 0.90). AP view mean articular step-off/displacement was 1.05 mm (SD: 0.96), while in the lateral view it was 0.33 mm (SD: 0.73). For CT, there was a mean diastasis of 4.37 mm (SD: 2.53) and an articular step-off/displacement of 2.30 mm (SD: 1.50).
Radiographic and CT measurement means.
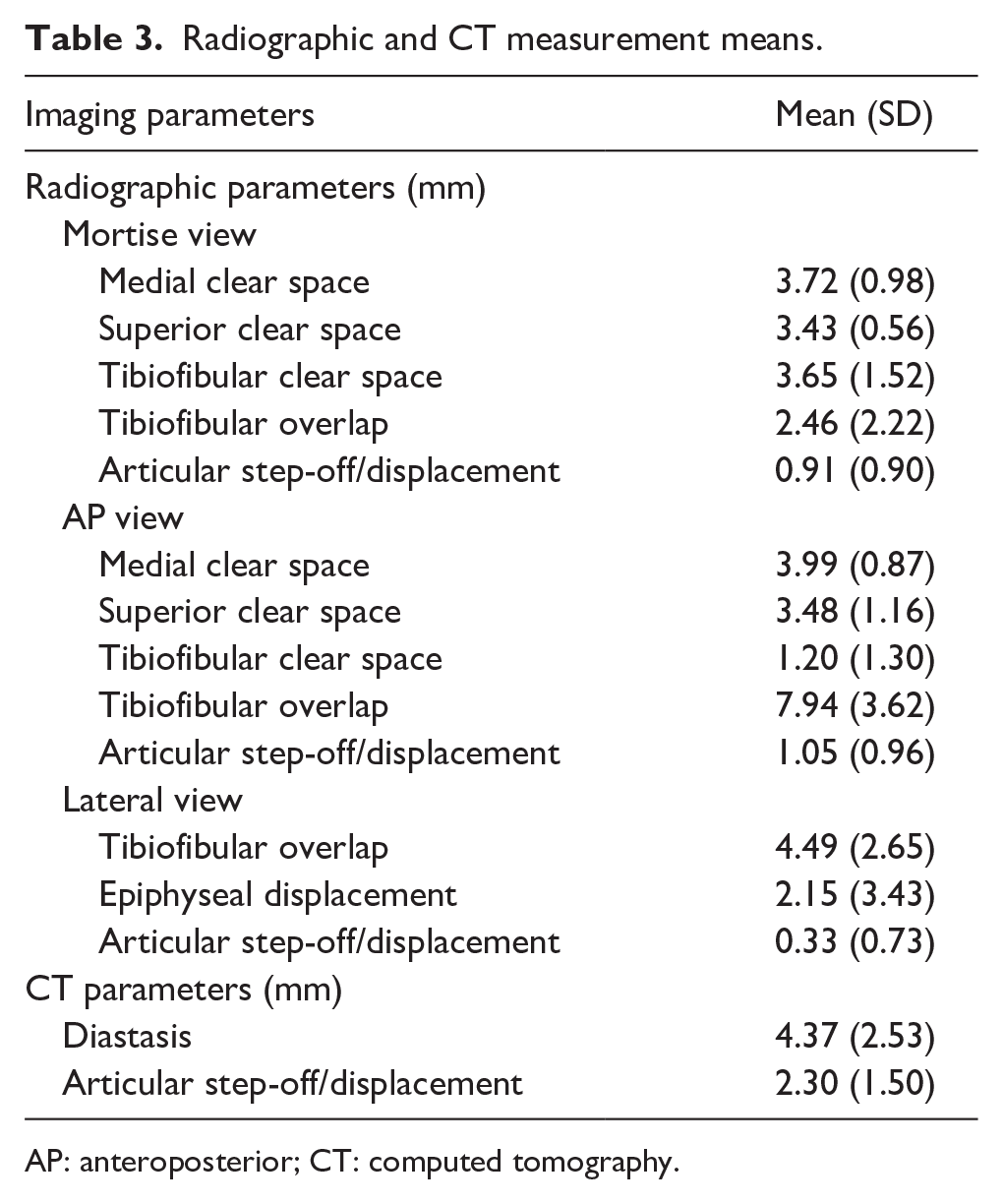
AP: anteroposterior; CT: computed tomography.
Correlations between radiograph and CT parameters
There were multiple significant correlations between radiographic and CT parameters. Mortise view tibiofibular clear space significantly correlated with CT diastasis (ρ = 0.27, p = 0.041; Table 4). In addition, mortise view articular step-off/displacement significantly correlated with CT articular step-off/displacement (ρ = 0.35, p = 0.006). Lateral view radiograph parameters of epiphyseal displacement and articular step-off/displacement both significantly correlated with CT diastasis (ρ = 0.55, p < 0.001; ρ = 0.28, p = 0.032). The correlation between lateral view epiphyseal displacement and CT diastasis was the strongest among all radiographic and CT parameters. All other radiographic parameters showed nonsignificant correlations with CT diastasis and articular step-off/displacement.
Radiograph and CT correlations.
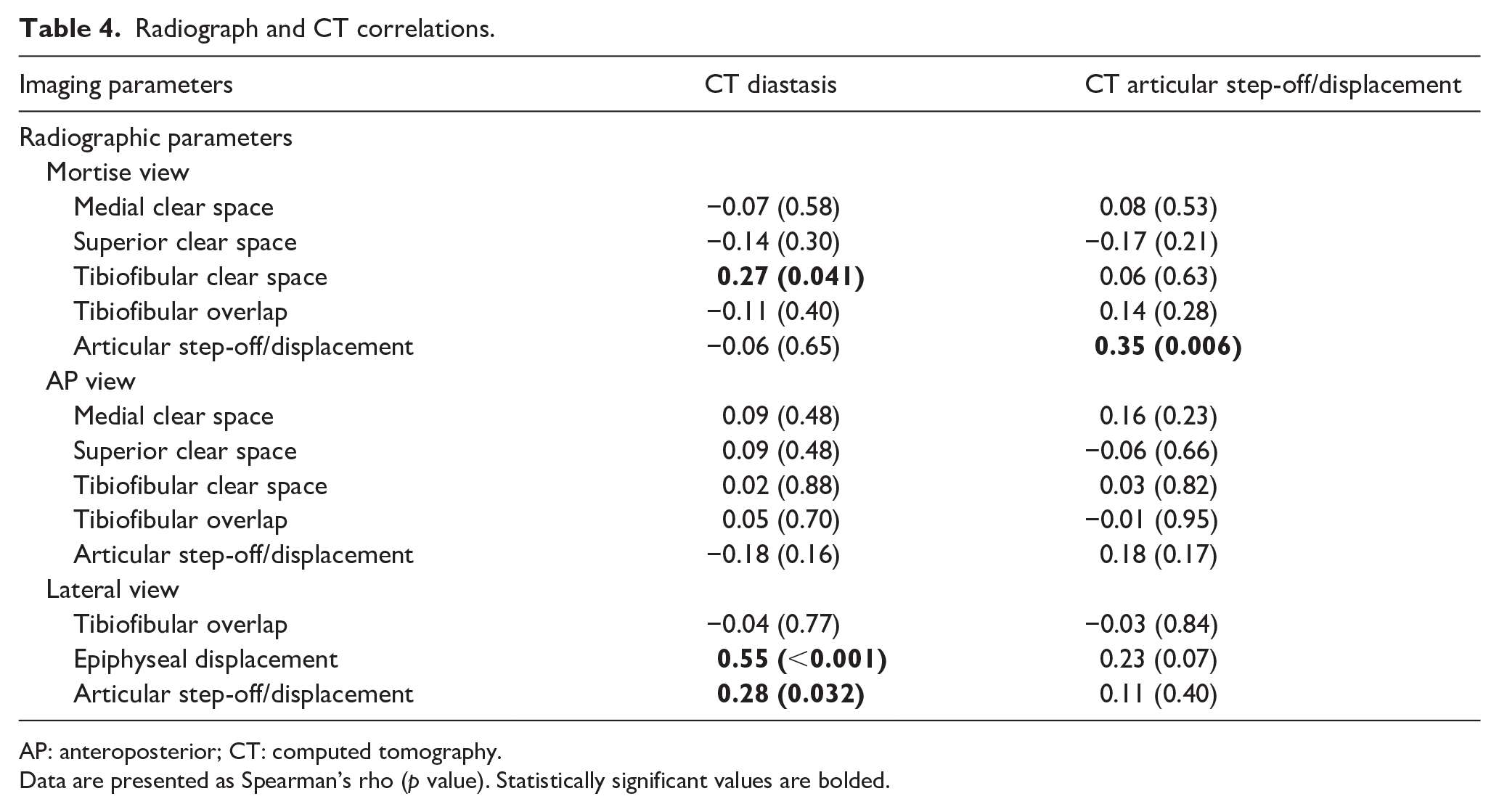
AP: anteroposterior; CT: computed tomography.
Data are presented as Spearman’s rho (p value). Statistically significant values are bolded.
Discussion
Surgical management of transitional ankle fractures is based on articular displacement or diastasis. This is often difficult to determine with radiographs alone, and it is common practice to obtain a CT scan for these injuries. It would be beneficial to identify fractures with a higher risk of displacement and selectively employ the use of CT, given its associated radiation and cost. Previous studies have attempted to compare radiographic and CT imaging for these injuries; however, they have been limited by small sample sizes.17,25 In this study, we found that several radiographic parameters, such as tibiofibular clear space on the mortise view and epiphyseal displacement on the lateral view, significantly correlate with increased displacement on CT. These specific parameters may be reliable indicators for the selective use of CT scans in patients with this injury.
The use of CT, in addition to radiographs, provides increased accuracy for articular fracture displacement.25,26 Given current guidelines supporting surgical intervention for triplane and Tillaux with an articular displacement of >2 mm, precision in this regard is vital to aid medical decision-making.3,22,23 While some studies have shown that CT is more sensitive than radiographs in assessing displacement,16,17 others have demonstrated that adding CT to radiographic measurements did not actually significantly change the amount of displacement documented or alter management.19,20 In addition, it has been shown that only 50% of surgeons actually used CT to evaluate triplane fracture patterns and only 38% of those surgeons always used CT preoperatively. 27 Overall, these discrepancies highlight the need for further investigation of the relationship between CT and radiographs for triplane and Tillaux fracture management.
In this study, we found that multiple radiographic parameters significantly correlated with the displacement of Salter–Harris III and IV fractures on CT. On the mortise view, increased articular step-off/displacement and tibiofibular clear space both correlated with increased CT displacement. Similarly, epiphyseal displacement and articular step-off/displacement on the lateral view also significantly correlated with increased CT displacement. These results suggest that specific radiographic measurements can identify fractures that are more likely to have articular displacement. However, it is important to note that we found correlation coefficients <0.7, 28 meaning radiographic measurements likely still underestimate the actual displacement visualized on CT as reported by several studies.8,17 This underestimation was reflected in comparing our mean radiographic and CT articular step-off/displacements, such as the radiograph AP (1.05 mm, SD: 0.96) and CT coronal (2.30 mm, SD: 1.50) articular displacement. However, it is possible that even though radiographs underestimate articular displacement seen on CT, separate cut-offs could be set for significantly correlating radiographic parameters to guide management plans. Future studies are needed to determine the exact measurement values on these radiographic parameters that are most effective in predicting operative displacement on CT.
Notably, lateral view epiphyseal displacement showed the strongest correlation out of all radiographic parameters to CT displacement. This is likely related to the avulsion of the anterolateral epiphysis fragment by the anterior inferior tibiofibular ligament. A recent study by Greenhill et al. 8 demonstrated that another lateral view radiographic parameter, metaphyseal displacement, can serve as a predictor for CT articular diastasis cut-offs in triplane fractures. Thus, instead of utilizing radiographic articular displacement, which may underestimate actual CT displacement, other radiographic parameters typically not considered for displacement or operative prediction, such as lateral view epiphyseal displacement, could be used instead. Further studies are needed to determine the operative cut-off value for lateral view epiphyseal displacement and the clinical impacts of solely using these specific radiographic parameters to guide the management of Tillaux and triplane fractures.
Our study also highlights the specific importance of both mortise and lateral view radiographs for these fractures and suggests that parameters in these views should be utilized when determining the need for CT scans in pediatric patients with transitional ankle fractures. If there is no articular displacement or increased tibiofibular clear space noted on these views, a CT scan may not be indicated. Further, for fractures with significantly increased measures in these parameters, it may also be appropriate to forgo a CT scan and proceed directly to surgery, as they are more likely to have displacement exceeding 2 mm on CT. However, it is important to note that CT scans may offer other details of the injury, such as additional fracture lines or comminution, that could impact surgical decision-making.29,30 CT may also be useful for preoperative planning, such as determining the approach or calculating the trajectory of epiphyseal screws. The mortise and lateral view measurements showed greater agreement and consistency across all raters compared to the AP when evaluating fractures of this nature. Recent studies have suggested the importance of understanding the axial fracture patterns in transitional ankle fractures for surgical planning, supporting the importance of mortise and lateral radiograph views for this process.8,18,31
This study has several limitations. First, although our study utilizes a large sample size of Salter–Harris III and IV fractures, there were only 10 patients with fractures <2 mm of displacement on CT. Although this prevented us from performing univariate analysis to determine radiographic parameters’ operative cut-offs, our analysis did show statistical and clinical significance. Future studies on patients who have less severe transitional ankle fractures and CT displacement <2 mm are needed to create predictive models for these radiographic measures. In addition, we selected certain radiographic factors for analysis, which may leave off novel measurements that could be utilized for predicting CT displacement. However, the measures we selected are commonly studied and measured factors for pediatric ankle radiographs.32,33 Measurement error between raters is possible, but the overall interrater reliability for almost all measures was at least good to excellent, including all the parameters with significant correlations. Due to the retrospective nature of our study, we were unable to determine if the use of a CT scan was the main factor for surgical intervention in a patient. Similarly, as our study focus was on imaging measurements, we did not stratify our analysis based on the patient’s mechanism of injury, which could also play a role in determining operative status. Additional factors, outside of imaging, related to the patient injury mechanism and trauma that may impact the decision for surgical intervention, warrant further research. Lastly, we included patients who had an attempted closed reduction before their CT imaging. While we obtained measurements on their radiographs after reduction and before their CT scans, this could have impacted comparisons to patients who only received splinting or casting. However, other studies for triplane fractures have included patients with closed reductions before CT to have a larger sample size for measurement comparisons. 8
Conclusion
This study demonstrates that several radiographic measures on the mortise and lateral views significantly correlate with articular displacement as measured on CT for transitional ankle fractures. Increased lateral view epiphyseal displacement showed the strongest correlation with CT displacement. These specific parameters should be evaluated when determining the need for CT scans in pediatric patients with these injuries and utilized in future studies to determine operative cut-off values.
Supplemental Material
sj-docx-2-cho-10.1177_18632521251338537 – Supplemental material for Three radiographic parameters correlate with computed tomography displacement in transitional ankle fractures
Supplemental material, sj-docx-2-cho-10.1177_18632521251338537 for Three radiographic parameters correlate with computed tomography displacement in transitional ankle fractures by Luke Sang, Steven M Garcia, Alex Youn, Katherine Bach and Ishaan Swarup in Journal of Children’s Orthopaedics
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251338537 – Supplemental material for Three radiographic parameters correlate with computed tomography displacement in transitional ankle fractures
Supplemental material, sj-pdf-1-cho-10.1177_18632521251338537 for Three radiographic parameters correlate with computed tomography displacement in transitional ankle fractures by Luke Sang, Steven M Garcia, Alex Youn, Katherine Bach and Ishaan Swarup in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Luke Sang: study design, patient chart review, performed measurements, statistical analysis, article preparation. Steven M Garcia: study design, statistical analysis, article preparation. Alex Youn: performed measurements, article preparation. Katherine Bach: performed measurements, article preparation. Ishaan Swarup: study design, measurement instruction, statistical analysis, project supervision, article preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of UCSF (no. 22-37700), with the need for written informed consent waived.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.