
Abstract
Purpose
We aimed to identify the long-term rate of relapse of deformity in a cohort of children with talipes equinovarus and to correlate it with pre-operative grading.
Methods
Between 1988 and 1995, 120 club feet in 86 patients were surgically treated. A review at an average follow-up of 11.5 years (range 9–16 years) was performed. Of 59 of the children, 69 feet were assessed clinically and data for the remaining 20 children (30 feet) were obtained from the records. The patients were assessed using the method of Bensahel and Dimeglio but radiological analysis was omitted. Functional and morphological evaluation was recorded.
Results
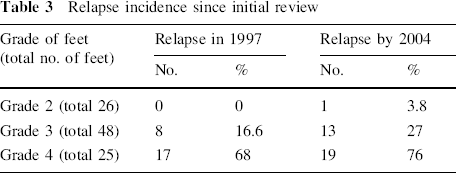
Initial grades were grade 2 in 26 feet (26%), grade 3 in 48 feet (49%) and grade 4 in 25 feet (25%). Relapse occurred in one case in grade 2 (3.8%), 13 feet in grade 3 (27%) and in 19 in grade 4 (76%). Since an initial review in 1997, a further 12.5% of grade 3 and 25% of grade 4 feet have relapsed. Overall function did not correlate with severity of deformity.
Conclusion
Relapse continues to occur after surgery during the first decade. There is a high rate of relapse (76%) in grade 4 feet.
Introduction
The aim of this study was to analyse the relapse rate following staged surgery for congenital talipes equinovarus. During the period 1988–1995, a cohort of 86 children with 120 club feet required surgery for recalcitrant deformity. All children underwent initial physiotherapy with serial plaster casts, and those with recalcitrant deformities underwent a two-stage surgical release. Due to severe multiple congenital problems, 6 children (total 10 feet) were excluded from the study. The early results of the remaining 110 feet have been published previously [1, 2]. This same cohort of patients have been reviewed at an average follow-up of 11 years (9–16 years) and assessed with regard to rate of relapse and functional outcome.
Materials and methods
Patients with talipes are reviewed regularly in the clinic and the medical records provide a prospective record of their treatment. Since the last review, 9 children with 11 feet have been lost to follow-up, leaving a study group of 71 children with 99 feet available for review at an average of 11.5 years follow-up (9–16 years). A total of 69 feet in 51 children were available for clinical and functional review in a dedicated research clinic. For the remaining 20 children and 30 feet, information was gathered from medical notes.
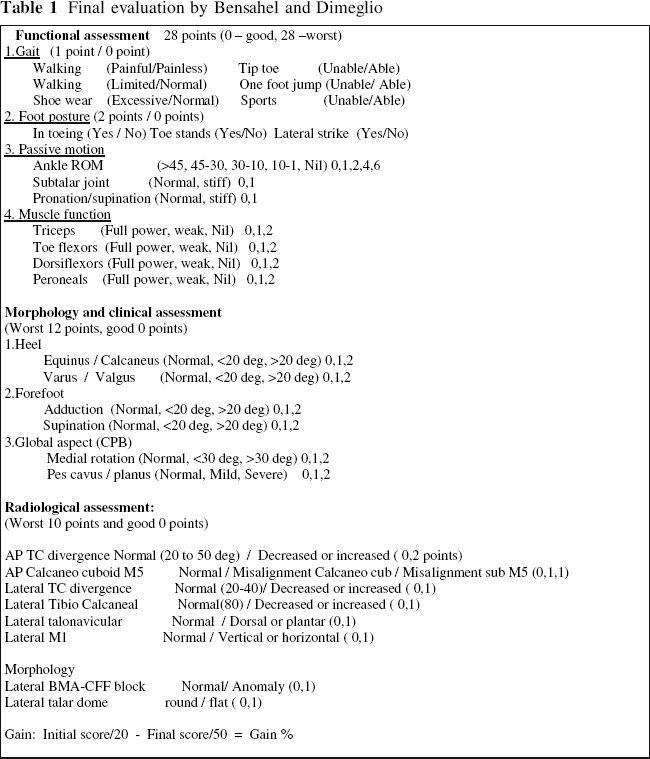
The patients were assessed using a method recommended by Bensahel and Dimeglio [3] (Table 1). The criteria for the functional and morphological evaluation were used, but radiological analysis was omitted. A relapse was defined as a requirement for any further surgery.
Final evaluation by Bensahel and Dimeglio
Statistical analysis was performed using the Cochrane–Armitage trend test.
The initial treatment schedule
As previously reported, all patients were classified prospectively into four grades, as shown in Table 2 [4]. Surgical release was performed as described by Carroll et al. [5] between 7 and 11 months of age, but the medial and lateral incisions were staged at an interval of 2 weeks. The patients spent 3 months in plaster, which was changed at 6 weeks. Night splints were then used until 2 years of age. Piedro boots were prescribed once walking commenced.
Dimeglio: classification of clubfoot

The surgical procedures involved release of the following structures:
Plantarmedial incision: abductor hallucis, deep fascia, plantar fascia, flexor digitorum brevis, abductor digiti quinti, the long and short plantar ligaments, the talonavicular joint capsule and the medial and plantar capsule of the calcaneocuboid joint. Posterolateral incision: lengthening of tendo-achilles, lengthening of tibialis posterior, division of calcaneofibular ligament, division of the posterior talofibular ligament, posterior capsular release of the ankle and subtalar joints and release of the anterior portion of the deltoid ligament.
Revision surgery
Surgery was performed “a la carte” but usually involved revision plantarmedial or posterolateral releases (as above), with or without lateral column shortening by excision of the distal calcanium. No frames were employed.
Results
Pre-operative grading
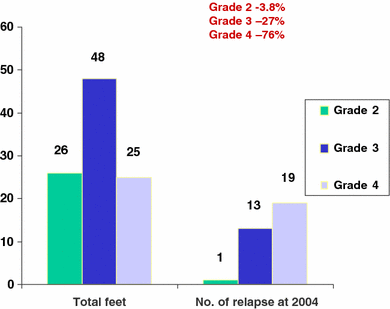
From the cohort of patients reviewed, initial classifications were grade 2 in 26 feet (26%), grade 3 in 48 feet (49%) and grade 4 in 25 feet (25%). The follow-up period was 11.5 years (range 9–16 years) and there were 50 boys and 21 girls.
Rate of relapse
Any further surgical procedures following the initial staged surgery were considered to constitute relapse. The number of relapses for each initial grade were a single case in grade 2 (3.8%), 13 feet in grade 3 (27%) and 19 in grade 4 (76%). Since the initial review in 1997 [2], a further 12.5% of grade 3 and 25% of grade 4 feet have relapsed as well as the single grade 2 foot. (Table 3; Fig. 1). The increased proportion of relapses with increasing severity of pre-operative grade was found to be statistically significant (P = 0.001).
Relapse incidence since initial review
Final relapse
Relapse related to gender
Relapse was noted in 48% of girls and 32% of boys. Statistically there is an increased trend for girls to relapse more than boys, but this was not significant.
Age at relapse
In grade 4 feet with relapse, 58% had relapsed by 2 years of age and 84% by 4 years. In grade 3 feet 8% relapsed by 2 years of age and 62% relapsed by 4 years (Fig. 2).
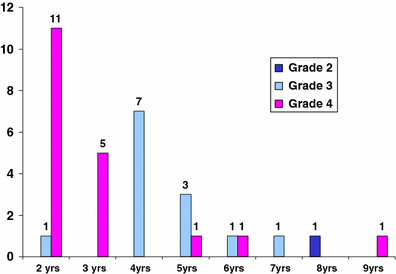
Age at relapse
Multiple procedures
In grade 4 feet with relapse, 48% required more than two procedures and in grade 3 feet multiple surgery was required in 10%.
Functional assessment
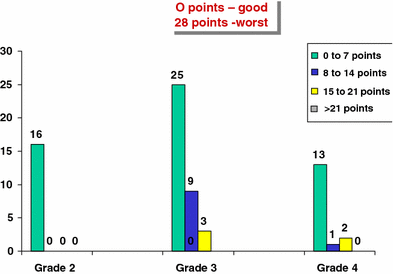
There were 69 feet (from 51 patients) available for clinical follow-up [grade 2 feet 16 (23%), grade 3 feet 37 (54%) and grade 4 feet 16 (23%)]. The functional assessment included gait, foot posture, and range of movement and muscle function. The scoring system uses a range from 0 (best) to 28 (worst) (Table 1).
The patients were arbitrarily separated into four groups for the study purposes (0–7 points, 8–14 points, 15–21 points and >21 points). Overall, 78.2% of feet scored 0–7 points (100% of grade 2, 68% of grade 3 and 81% of grade 4) (Fig. 3). Some degree of pain was present in 10% of feet.
Functional assessment
Morphological assessment
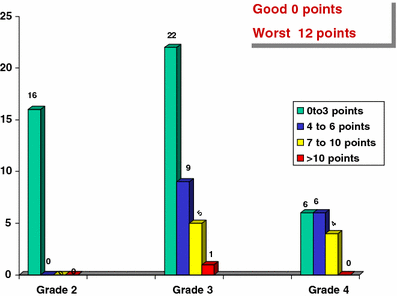
The morphological assessment included assessment of the heel, forefoot and the global aspect of the foot. The scoring system ranged from 0 (good) to 12 points (worst) (Table 1). The patients were arbitrarily separated into four groups for the study purposes (0–3 points, 4–6 points, 7–10 points and >10 points).
Overall 64% of feet scored 0–3 points (100% of grade 2, 59% of grade 3, 37.5% of grade 4). In grade 3 feet 24% scored 4–6 points and in grade 4 feet 37.5% scored 4–6 points. In grade 3 feet 14% scored 7–10 points and in grade 4 feet 25% scored 7–10 points (Fig. 4).
Clinical and morphological assessment
Total final evaluation
This was the combination of functional and morphological assessment. X-ray examination was not included in this study and therefore the maximum score was 40 points.
The median value was calculated for the different grades with varying ranges. The median value for grade 2 was 3 (range 2–22), grade 3 was 6 (range 0–28) and grade 4 was 5 (range 1–25).
Discussion
From this analysis, we report that there is an increasing rate of relapse over time in all grades of clubfeet, with the highest occurring in grade 4. Since our last review [1, 2], relapse has been noted in an additional 25% of grade 4 feet, making a total relapse rate of 76%. These feet have required multiple procedures relative to those with lesser grades of severity. Relapse was observed in a significant proportion (58%) of patients with grade 4 feet in this series by 2 years of age when compared with those with grade 3 feet, in whom only 8% relapsed by 2 years of age. It is also noted that 48% of grade 4 feet needed more than two operative procedures. Sobel et al. [6] reported of more than one operation in 56% of cases and concluded that repeat operations reflect the dynamic muscle imbalance that defines the natural history of clubfoot.
Hutchins et al. [7] reported further surgery in 26.6% of cases and Hudson and Catterall [8] described 32% of cases requiring re-operation. Esser [9], in his account of 15 years’ experience, has noted excellent or good results in 90% of cases. In addition to the posterolateral release, a medial release and tibialis anterior transfer to the lateral border of the foot were performed. Porter [10] described initial hind foot release in all patients followed by forefoot medial correction at a later date in certain cases. The patients were compared with results from the pre-operative assessment. Favourable outcomes occurred with only 19% hindfoot relapse and 9% forefoot relapse. Magone et al. [11] reported poor results in 23% and fair in 29% of cases; Kranicz et al. [12], reporting a 20-year review following posteromedial release, has shown “satisfying foot form and function”.
The comparison of results with other series is difficult, as most do not include pre-operative classification of the deformity. Reported rates of relapse are therefore shown as an average of all feet treated rather than relative to the initial severity, which would be more relevant. This series, however, has clearly shown that the worse the grade of deformity at the outset, the higher the chance of relapse and of requiring multiple surgeries. The results also demonstrated that relapses can occur within the first decade of life, and appropriate follow-up is therefore required to identify relapses as early as possible. From the reported analysis, it is clear that foot morphology predictably varies with the degree of severity of initial grading. The functional assessment shows that the overall function of many of these feet is very acceptable despite the severity. Of the children, 10% had pain in their feet, and this is directly related to the morphology.
In the reported series, only 7% of children were unable to be involved successfully in school sports. Bjonness [13], in his study of 95 patients with respect to social adaptation and subjective symptoms from the foot, showed that patients managed themselves well and despite physical and psychological handicaps they deviated relatively little from the normal population with regard to work, sports and other social adaptability.
Contemporary children's orthopaedic practice favours the use of serial casting, as described by Laaveg and Ponseti [14]. Many would argue that the discussion regarding the use of surgery for talipes is somewhat obsolete in light of the success of the Ponseti method. Certainly the global advance of this minimally invasive technique has revolutionised the treatment of club feet and provided safe treatment where previously there was none. However, for certain children and their families, concurrent illnesses or social and cultural factors may preclude the non-operative approach. The technique is time consuming for families, and for those living long distances from treatment centres there is inevitably some appeal in a “quick fix” which can be achieved with surgery (David Clews, Waikato Hospital, New Zealand, Personal Communication).
The Ponseti method relies on the use of an abduction foot orthosis to maintain the correction achieved with serial casting. This device needs to be fitted properly and changed to accommodate growth. More importantly it is essential to be retained for up to 4 years to reduce the rate of relapse, which may still occur. Closer analysis of the outcomes, relative to the initial classification of feet treated using the Ponseti method, will also provide useful information in predicting difficulty with treatment and relapse rates. In some cases there remains a realistic opportunity to consider surgery as a definitive solution rather than adopt the non-operative approach.
The results reported in this paper suggest that the use of surgery for the stiffest group of feet is destined to require multiple operations to achieve any lasting correction, and this is a heavy price to pay for any family. Therefore, it would seem reasonable that if surgery is being considered for the treatment of talipes then it should be reserved for the milder and more flexible deformities found in grade 2 and possibly grade 3 feet but resisted at almost any price for grade 4 feet.
Conclusion
Staged soft tissue surgery for the treatment of club feet results in an unacceptably high rate of relapse for grade 4 feet (76%) and multiple procedures were required to achieve correction. A more favourable outcome was encountered for the less severe deformities found in grades 2 and 3. Relapse after surgical correction continues to occur during the first decade and appropriate follow-up is recommended.