
Abstract
Personality traits are important predictors of health behaviors, healthcare utilization, and health outcomes. However, we know little about the role of personality traits for emergency department outcomes. The present study used data from 200 patients (effective Ns range from 84 to 191), who were being discharged from the emergency department at an urban hospital, to investigate whether the Big Five personality traits were associated with post-discharge outcomes (i.e., filling prescriptions, following up with primary care physician, making an unscheduled return to the emergency department). Using logistic regression, we found few associations among the broad Big Five domains and post-discharge outcomes. However, results showed statistically significant associations between specific Big Five items (e.g., “responsible”) and the three post-discharge outcomes. This study demonstrates the feasibility of assessing personality traits in an emergency medicine setting and highlights the utility of having information about patients’ personality tendencies for predicting post-discharge compliance.
Relevance Statement
Researchers and physicians may be able to use information about patients’ personality to identify those most at risk for unfavorable post-discharge outcomes and tailor their treatment plans to suit their personality tendencies to improve health.
Key Insights
Personality traits can be reliably assessed in emergency department setting. No associations among broad Big Five traits and post-discharge compliance. Several associations among specific Big Five items and post-discharge compliance.
Keywords
Emergency departments can be chaotic places. Blunt force trauma, stomach pain, mysterious bumps and rashes, alcohol poisoning, hypothermia – the ailments that bring people to emergency departments are infinite in scope, yet physicians and nurses are tasked with the same broader goals: 1) identify the source of the problem, and 2) create a treatment plan. Oftentimes, these treatment plans require patients to follow post-discharge instructions after they leave the emergency department such as filling prescriptions and/or making an appointment to follow-up with their primary care physician. Outside of the controlled hospital setting, we know very little about the factors that predict
We define personality traits as falling into five broad domains: Extraversion (the tendency to be sociable, assertive, and lively); Agreeableness (the tendency to be warm, kind, and cooperative); Conscientiousness (the tendency to be self-controlled, organized, and responsible); Neuroticism (the tendency to worry, be moody, and lack self-confidence); and Openness to Experience (the tendency to be creative, adventurous, and open-minded; John & Soto, 2021). The Big Five personality traits predict important health outcomes such as health behaviors and healthcare utilization (Friedman, 2008; Hakulinen et al., 2015a; Hakulinen et al., 2015b; Jokela et al., 2018; Sutin et al., 2016), disease onset and progression (Friedman, 2008; Sutin et al., 2013; Weston et al., 2015), and mortality risk (Graham et al., 2017; Jokela et al., 2013; Mroczek et al., 2009; Turiano et al., 2015). However, little work has been conducted at the intersection of personality science and emergency medicine.
Of the work that has been done, most studies have examined the personality profiles of emergency medicine personnel (i.e., are the personality profiles of emergency medicine personnel different from those of personnel who work in other medical specialties?; Jordan et al., 2018). The remaining studies often focused on the personality characteristics of people who use (versus do not use) emergency healthcare services (Chapman et al., 2009; Friedman et al., 2013; Hajek et al., 2017), suggesting there are self-selection effects of
To our knowledge, no prior work has examined whether patients’ personality tendencies are associated with their
Because the Big Five domains are broad, multi-faceted characterizations of personality tendencies, the present study also explored whether specific Big Five items, otherwise known as “nuances” (McCrae, 2015; Mõttus et al., 2017; Mõttus et al., 2020), were associated with each of the post-discharge outcomes. Prior work has suggested that facets and items within domains have divergent associations with health outcomes, sometimes nullifying the effect at the Big Five domain level (Hagger-Johnson & Whiteman, 2007; Weiss & Costa, 2005). In addition to capturing these divergent associations, exploring the associations between Big Five
The Present Study
The present exploratory study uses data collected in an emergency department, with a short-term longitudinal follow-up (1-2 weeks later) to examine how personality traits predict post-discharge outcomes. This research makes several unique contributions to the literature. First, the present study examined the feasibility of measuring personality traits in an emergency medicine context. Psychosocial data collection in emergency department settings poses numerous challenges, given that the people who are in the emergency department are likely to have fewer cognitive and emotional capacities for engaging in a research study with abstract psychological questions than the typical participant. Second, the present study incorporates a short-term longitudinal design, with a follow-up assessment of the patients 1-2 weeks after discharge. This permits an investigation of the outcomes that individuals experience even after they leave the emergency department and provides a better understanding of how we might predict the likelihood of individuals making unscheduled returns to the emergency department. Third, we administered a reliable and well-validated personality measure commensurate with those used in large national probability samples such as the Health and Retirement Study (Sonnega et al., 2014) and the Midlife in the United States Survey (Brim et al., 2004). Further, we examine the broad Big Five domains and specific Big Five items in relation to emergency department post-discharge outcomes. Last, to our knowledge this is the first study that aims to understand whether patients’ personality traits predict emergency department post-discharge outcomes. Thus, the present work not only has important theoretical implications for the predictive power of personality characteristics on health outcomes, but it also has many practical implications for how we might use information about patients’ personality tendencies to improve their individual health while also reducing the public health costs associated with individuals making repeated visits to emergency departments. We do not have any hypotheses; the present research was not pre-registered and is exploratory.
Method
Participants and Procedures
The present study used data collected from patients at a 57-bed Emergency Department (a verified Level 1 Trauma Center) at a major urban university hospital in the United States. The present study was granted approval by the Northwestern University Institutional Review Board (Protocol # STU00094889; Behavior Profiling in the Emergency Department [ED]), and data were subsequently collected from August 2014 to January 2015. To recruit participants, patients who were close to being discharged from the emergency department were asked to participate (the nurses on staff provided guidance to the interviewers about which patients would be best to approach). The patients who agreed to participate were administered a brief mental awareness and cognitive impairment inventory: the Short Portable Mental Status Questionnaire (SPMSQ; Pfeiffer, 1975). Sixty-five percent of those who were approached agreed to participate and had intact intellectual functioning or only mild intellectual impairment (0-4 errors out of 10 possible errors on the SPMSQ), resulting in a sample of 200 patients (58% female) that were diverse with respect to age, race, ethnicity, and education level.
1
There are no prior publications with this dataset to report.
Approximately 1-2 weeks after being discharged from the emergency department, patients were contacted via telephone and queried on several aspects of their emergency department visit(s) including the reason for their visit(s), mode(s) of transport, and whether they made an unscheduled return to the emergency department since their initial visit. Additionally, participants reported on the extent to which they adhered to their initial post-discharge instructions (i.e., followed-up with their primary care physician, filled prescriptions), as well as their satisfaction with their emergency department experience(s). For a full list of items administered in the study protocol, please see the study codebook in Supplementary Materials. Of the 197 people included in the present analyses, 160 completed the follow-up telephone survey (81%). The effective Ns range from 84 to 191. The majority of participants indicated that they went to the emergency department on their initial visit because of symptoms such as pain, dizziness/fainting, headaches/migraines, dehydration, high blood pressure, or kidney stones/urinary problems (44% of sample). The remaining participants went to the emergency department because of an accident (24%), an infection, virus, or allergy (12%), women's health issues related to pregnancy or miscarriage (6%), post-operative complications or doctor referrals (4%), a chronic condition (3%), psychiatric problems (3%), or something else (4%).
Measures
Big Five Personality Traits
At Time 1, participants completed the Midlife Development Inventory (MIDI) personality scales (Lachman & Weaver, 1997), a 26-item measure of the Big Five personality traits that has been shown to be a reliable and well-validated tool to measure personality (Brim et al., 2004; Sonnega et al., 2014). Based on prior research (Hill & Roberts, 2011), seven additional Conscientiousness items (i.e., industrious, traditional, self-controlled, persistent, orderly, reliable, impulsive) were also administered to participants because it was hypothesized at study conception that Conscientiousness had the most theoretical relevance for predicting post-discharge outcomes. Participants responded to the 33 items on a 4-point Likert scale ranging from 1 (
Post-Discharge Outcomes
At follow-up (1-2 weeks post-discharge), participants reported on three outcomes. Specifically, participants responded to dichotomous (0 =
Results
All analyses were conducted using R (R Core Team, 2021). Please see code for all analyses provided in Supplementary Materials. The data cannot be made publicly available on the OSF because: a) we did not receive IRB approval to share patients’ data, and b) the patients did not consent to having their deidentified data shared. Qualified researchers can email the corresponding author for access to a limited dataset to reproduce analyses. Analyses were not pre-registered; we report effect sizes, 95% confidence intervals, and exact
To investigate the potential impact of attrition, we compared individuals who did and did not participate in the follow-up survey on study variables assessed at Time 1 (i.e., Big Five personality traits, gender, age, income). Individuals who provided follow-up data were lower on Neuroticism at Time 1 than those who did not provide follow-up data (
To test whether there were selection effects, participants were asked at baseline: “
Table 1 shows descriptive statistics and a bivariate intercorrelation matrix for all study variables. When queried about their post-discharge experiences, 60% of the sample (
Means, Standard Deviations, and Correlations Among Study Variables
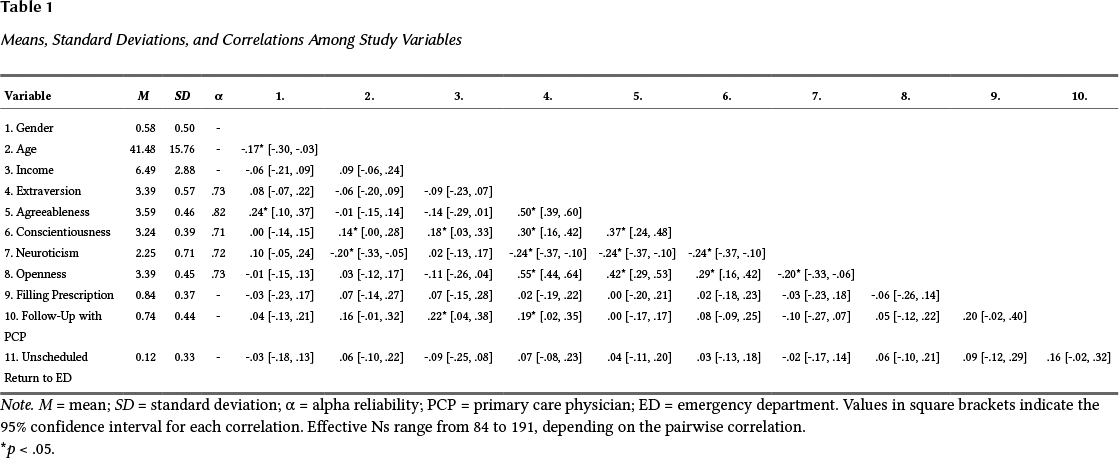
*
We also conducted follow-up analyses to determine whether there were any systematic differences among participants who did vs. did not receive instructions to fill a prescription or follow up with their primary care physician. 69 out of 161 people (43%) did not receive instructions to fill a prescription at discharge, whereas 92 out of 161 people (57%) did receive instructions to do so. 30 out of 161 people (19%) did not receive instructions to follow up with their primary care physician, whereas 131 out of 161 people (81%) did receive instructions to do so. There were no statistically significant differences between instruction vs. non-instruction groups on the Big Five personality traits or sociodemographic variables for either outcome, with the exception of income differences in those who received instructions to follow up with their primary care doctor. Participants who received instructions to follow up with their primary care physician had lower incomes than participants who did
Table 2 shows odds ratios and 95% confidence intervals for binary logistic regressions (with and without covariates) for the three post-discharge outcomes: filled prescription, followed-up with primary care physician, and made an unscheduled return to the emergency department. In the first set of analyses, we entered gender, age, income, and the Big Five domain scores as predictors of post-discharge outcomes. We included gender, age, and income as covariates because these factors have shown associations with both the independent (i.e., Big Five personality domains) and dependent variables (e.g., adherence, healthcare utilization) in prior research (e.g., Chapman et al., 2009); and thus, could confound the relationship between personality traits and post-discharge outcomes. In these analyses, we found that the demographic factors and the broad Big Five personality domains were not related to post-discharge outcomes, with one exception. Individuals with higher incomes were 1.18 times more likely to follow up with their primary care physician after being discharged from the emergency department than individuals who were less affluent. In unadjusted models without covariates, the aforementioned results hold and one additional effect emerged: Individuals higher in Extraversion were 2.76 times more likely to follow up with their primary care physician post-discharge.
Odds Ratios from Binary Logistic Regressions Between the Big Five and Post-Discharge Outcomes With and Without Covariates

*
We also conducted exploratory follow-up analyses to examine whether specific Big Five

Big Five Items Predicting Post-Discharge Outcomes
Discussion
How Are Personality Traits Associated With Post-Discharge Outcomes?
When we examined whether the broad Big Five personality domains predicted post-discharge outcomes, we found no statistically significant associations. These results are somewhat surprising because prior work has shown that personality traits are related to medication and doctor adherence (Friedman et al., 2013; Hajek et al., 2017; Hill & Roberts, 2011; Jerant et al., 2011; Molloy et al., 2014), and we expected adherence to post-discharge instructions from the emergency department to be no exception. Although it is quite possible that the true associations are, in fact, null, there are several alternative explanations for why we may have observed this pattern of findings.
First, the sample size in the present study was small and thus, we are underpowered for observing what are likely to be small effects between broad personality traits and post-discharge outcomes. This is particularly true because not all participants indicated that the attending emergency medicine physician gave them post-discharge instructions to fill a prescription or follow up with their primary care physician, reducing sample sizes further (effective Ns ranging from 84 to 191).
Second, although there were no systematic personality differences between participants who did versus did not receive instructions to fill a prescription or follow up with their primary care physician, there are likely other selection biases at play that influence the effect size estimates. For example, when study participants were asked if they had been to the emergency department in the past 12 months (apart from their current visit), we found that there were systematic differences between individuals who
Third, the Big Five domains are very broad and multi-faceted characterizations of personality; and thus, it is possible that components
Considerations for Future Personality Research in the Emergency Medicine Setting
Sample Size
Although unique in its study design and population, the present study is limited by its rather small sample size (effective Ns range from 84 to 191). The intent of the present study was to be a proof-of-concept to serve as the basis for future federal grant applications at the intersection of personality science and emergency medicine. Due to the expense of conducting research in an emergency department setting, the present study is likely underpowered for detecting what are likely to be small associations among personality traits and compliance with post-discharge outcomes. Because of the small sample size, exploratory data analytic approach, and wide confidence intervals of effect sizes, all of the findings reported in this manuscript should be interpreted with caution until they are directly replicated with a larger sample. This is especially true for the item-level analyses where all 33 items are entered as predictors into the model. It will be necessary for future well-powered research to replicate the present findings, ideally with pre-registered analytic plans, to ascertain that the direction, magnitude, and importance of effect sizes are robust enough to warrant future application in medical settings.
Feasibility
A basic question that we were interested in addressing was the extent to which we could assess psychosocial constructs in the often chaotic emergency department setting. Patients visit the emergency department for a variety of reasons, but the immediacy of those reasons likely contributes to patients being more distracted and more burdened with cognitive, emotional, and physical fatigue than is typically seen in other research contexts. When we examined data quality in the present study, we found surprisingly few issues to contend with. Two-thirds of the patients who were approached in the emergency department agreed to participate and passed the brief cognitive status inventory. Moreover, out of the 200 people included in the sample, we only had to exclude two participants for poor data quality (as reported by the interviewers conducting the assessments) and one participant for non-differentiation of the personality item responses (i.e., straight-lining). In fact, the vast majority of the sample (85%) were rated as having good data quality by the interviewers.
Based on reliability analyses, we also found that the Big Five personality traits had high internal consistencies, with alpha reliabilities ranging from .70 (Conscientiousness) to .82 (Agreeableness). These reliability coefficients are comparable to, or even higher than, the alphas observed in other large-scale nationally-representative studies that used the same personality inventory, such as the Midlife in the United States Study (Brim et al., 2004), which shows alphas ranging from .58 (Conscientiousness) to .80 (Agreeableness). In sum, despite the fact that the patients in the present sample are likely experiencing more stress and cognitive, emotional, and physical load than the typical research participant, we found that we were able to obtain reliable signals of individual differences in personality even in this high-intensity setting, demonstrating the feasibility of collecting psychosocial patient data in this setting.
Representativeness of Sampling
Given the sensitive nature of collecting patient data in an emergency department setting, the interviewers for the present study worked in tandem with the nurses on staff, who provided advice about which patients might be amenable to approach, and alternately, which patients were in distress and likely would be unable to participate. Although this approach was a major boon to data collection, it is likely that this guidance from the nurses inadvertently biased the sample because perceived mood and illness burden are systematically related to personality traits, namely Conscientiousness and Neuroticism. Likewise, because many of the patients were close to being discharged from the emergency department, this is not necessarily a representative sample of all emergency department patients, given that the patients who came in with the most severe problems or least lucidity would not be represented in the participant pool. That being said, the conditions that bring people to the emergency department cut across important sociodemographic characteristics, bolstering sample heterogeneity. This is particularly true for the present study because the emergency department where patient data were collected was at a major, urban hospital that draws people from affluent neighborhoods in the immediate proximity as well as from low-income neighborhoods several miles away.
Nevertheless, data collection in this setting is complex because there needs to be a balance of respecting patients who are already under a significant amount of stress versus minimizing sample bias. We see two ways of dealing with this issue in future research: 1) half of the sample is recruited via tight collaboration between the research team and healthcare providers, whereas the other half of the sample is not recruited based on advice from the nurses, to allow for direct tests of sampling bias based on the key constructs of interest; and 2) collect data from someone other than the patient. In many cases, a close family member or friend accompanies a patient to the emergency department, and this close other may be a reliable source of information about the patient's personality, are presumably under less distress than the patient themselves, and are less likely to feel burdened by study participation. Moreover, collecting informant-reports in the emergency department setting would help to reduce inflated effect sizes due to shared method variance, particularly if the patient provides self-reports at the follow-up visit(s).
Study Protocol
We have several recommendations for future research study protocols. First, we found it useful to look at both broad personality domains as well as specific personality nuances. Because both domain- and item-level approaches have advantages and disadvantages (in terms of reliability and the capacity to provide mechanistic explanations), reporting both in the same paper provides the fullest understanding of a particular phenomenon. This approach also has practical utility for future research and application. If future well-powered research replicates the predictive utility of
Second, we recommend future researchers add several variables to the study protocol: insurance (i.e., private, public, underinsured, uninsured); more context for the reason of the visit (e.g., chronic condition) and probability of reoccurrence (i.e., how many times the patient has been to the emergency department for the same reason(s)); a wider range of post-discharge instructions beyond prescriptions and following up with one's primary care physician; additional outcomes of an emergency department visit (e.g., symptom remission); the extent to which patients had difficulties complying with administered instructions (e.g., “to what extent did you experience difficulties carrying out the instructions given to you at discharge?”) and
Third, the time lag between the initial assessment and follow-up was short, with participants queried approximately 1-2 weeks after their initial visit to the emergency department. Thus, it is possible that some participants filled their prescriptions, followed up with their primary care physician, and/or made an unscheduled return to the emergency department 15+ days after their initial visit, though these outcomes are not considered in the data collected in the present study. Future research would benefit from conducting multiple assessments of varying time lengths post-discharge, in order to better understand the long-term influence of personality traits on post-discharge outcomes. Similarly, assessing personality traits and health at multiple timepoints would help researchers to draw stronger,
Conclusion
Upon further examinations of the replicability and generalizability of the present findings with highly-powered replication studies, it may become clear that individual differences in personality are one way to identify patients who are most at risk for not adhering to post-discharge instructions and making repeated visits to the emergency department. If personality traits can help us to identify the patients most at risk for these unfavorable outcomes, then future researchers and emergency medicine personnel can work together to develop systems that utilize knowledge about patients’ personality to improve individual health and reduce public health costs associated with repeated visits to the emergency department.
Footnotes
Supplementary Materials
For this article the following Supplementary Materials are available via the PsychArchives repository (for access see Index of Supplementary Materials below):
Ethics Statement
The present study was granted approval by the Northwestern University Institutional Review Board (Protocol # STU00094889; Behavior Profiling in the Emergency Department).
This research was supported by a pilot grant awarded to Daniel K. Mroczek and Mitesh B. Rao from the Feinberg School of Medicine at Northwestern University, as well as grants from the National Institute of Aging awarded to Daniel K. Mroczek (AG018436; AG064006).
The authors have declared that no competing interests exist.
We would like to thank Scott Dresden MD, Mark Courtney MD, and Jorge Villareal for their supportive roles throughout this project.
Related Versions
No other previously published versions of this manuscript exist in part or in whole.