
Abstract
The vessels are twisted in a longitudinal 3D space in the lower limbs of humans. Thus, it is difficult to perform an ultrasound scanning examination in this area. In this paper, a new medical parallel robot is introduced to effectively diagnose vessel disease in the lower limbs. The robot's position repeatability and accuracy are evaluated. Furthermore, the robot's accuracy is improved through a calibration process in which the kinematic parameters are identified through a simple identification approach.
Introduction
Ultrasound (US) scanning examination is one of the major diagnostic modalities in daily medicine. It shows advantages in low cost and non-radiation to the human body. However, a survey reveals that the repetitive strain of daily US examination over many hours causes musculoskeletal disorders to sonographers [1]. Thus, much research is engaged towards the design of medical robots to perform the US scanning examination. Furthermore, the US medical robot can collect position data during the examination process, which provides the essential information for 3D reconstruction of the scanned area.
Several works on US medical robots have been performed. A portable US medical robot was proposed in a telescanning robot project [2]. It has four degrees of freedom (DOF) and assists a doctor in controlling a US probe remotely. The robot prototype is extended to 6 DOF in the OTELO project [3]. It is agile and able to cover the large scan area. Nevertheless, the US scanning examination requires an assistant to hold the robot during the examination process. In general, the portable medical US robot does not reduce the workload of sonographers. Many US medical robot systems are developed based on industrial robots. The Hippocrate system employs a PA-10 robot arm from Mitsubishi Heavy Industry to scan the carotid artery [4]. An F3 industrial robot from CRS Robotics was used in [5] to diagnose breast cancer. A lightweight robot LWR from KUKA was used in [6] to assist the sonographer. However, the industrial robots are mostly designed for general use, and medical applications are limited due to the closed architecture of the controllers. Thus, some serial robots are designed for US medical implement, such as an abdominal US scanning robot in [7], and a self-balanced robot from the University of British Columbia [8, 9]. Serial robots, however, have relatively low stiffness and their position errors are accumulated and amplified from link to link. Besides, the motors are generally mounted on links successively. Thus, each link has to support the weight of all the subsequent links and actuators. Several medical US robots were designed with parallel structures. A parallel robot was developed to hold the US probe in [10]. It consists of three legs displaced on both sides of the patient and a probe gripper hanging over the scanned area. A cable robot was developed in the TER project [11]. A sliding mechanism was used in a parallel robot to perform echo-graphic diagnosis [12, 13]. The patient has to support the weight of the robot since the mechanism is placed on the scanning area. WTA-2R was designed to hold the US probe and perform an automated scanning based on US image feedback in [14].
The medical robots mentioned above are mainly designed for carotid or abdominal US scanning, and are not appropriate for examination in the lower limbs due to their limited workspace, dexterity, etc. MedRUE (for
The calibration of a US medical robot involves probe calibration and kinematic calibration. The probe calibration identifies the constant transformation between the probe body and US image [17, 18]. However, in this article we focus only on the kinematic calibration of the robot. The kinematic calibration methods for serial robots are mostly on identifying the Denavit-Hartenberg parameters [19, 20]. These parameters are widely used to develop the kinematic model of serial robots. However, they are not always the simplest way to model parallel robots. The calibration methods of parallel robots vary depending on the different geometric structures of parallel robots. There are many calibration studies regarding planar robots, the Gough-Stewart platform and the Delta robot [21–25].
In this paper, we present a new medical robot with its repeatability and accuracy assessment. The position accuracy is improved by a calibration method based on direct position measurements with a laser tracker. The method is easy to implement on the robot without elaborate knowledge of the advanced kinematic calibration. In addition, the proposed calibration method identifies kinematic parameters individually, and the nonlinear interferences between kinematic parameters are significantly reduced. Therefore, the identified kinematic parameters are more accurate, and are important for further research, such as temporal stiffness calibration. By contrast, other calibration methods using optimization identify all kinematic parameters simultaneously [26–28]. The optimization approach may achieve better end-effector position accuracy, but it sacrifices precision for individual parameters. The MedRUE robot is briefly described in section 2 and its kinematic model and calibrated parameters are presented. Section 3 discusses the assessment of repeatability and accuracy. Then, the proposed calibration method and the result are demonstrated in section 4. At the end, a conclusion is addressed in section 5.
Robot description and kinematics
In this section, the new medical robot is introduced and its intuitive kinematic model is discussed. The kinematic model considers the errors of link lengths and offsets which need to be calibrated, and thereafter the calibrated parameters are listed. The robot base reference frame (
Introduction of MedRUE
MedRUE (Medical Robot for vascular Ultrasound Examination) is a prototype of medical parallel robot designed for the diagnosis of the peripheral arterial disease in the lower limbs.

MedRUE: a new prototype of medical US robot
As shown in Figure 1, MedRUE is a 6-DOF parallel robot consisting of a robot base with a linear guide, two five-bar mechanisms and the tool part to carry the US probe. The U-shaped robot base is mounted on a linear guide (driven by actuator Q1). The two five-bar mechanisms are assembled symmetrically on the robot's base, and are driven by actuators Q2, Q3, Q4 and Q5. Considering the first five-bar mechanism as an example, the two links driven by actuators are called proximal links, and the two links farther from the robot base are called distal links. The distal links connect at the shaft of the tool part. The tool part consists of a force/torque sensor and a dummy probe at the end. It is driven to rotate along the shaft by a small actuator Q6 mounted on a distal link.
Since most actuators of MedRUE are located on the robot's base, the links of the five-bar mechanisms do not need to bear the heavy load of motors. Thus, the robot is relatively lightweight and agile. The linear guide extends the workspace along the length of the patient's leg and the curved distal links avoid mechanical interferences between the robot arms and the patient leg during the examination.
Frame
The kinematic model of MedRUE and its kinematic parameters are illustrated in Figure 2. The two five-bar mechanisms are symmetrically assembled on the robot's base, and can therefore be modelled in the same way. As shown in Figure 2(a), the links of the ith five-bar mechanism are named L
ij
, where i = 1, 2 and j = 0, …, 4. The corresponding link lengths are denoted by l
ij
. Link Li0 is fixed on the robot's base with an angle θ
i
offset. Four actuators Q2i and Q2i+1 are mounted on the robot's base, and the corresponding active joint variables are q2i and q2i+1 at A
i
and C
i
respectively. The other joints q
Bi
, q
Di
and q
DEi
are passive. The two five-bar mechanisms are parallel to the y0z0 plane. In Figure 2(b), the tool part connects the two five-bar mechanisms at E
i
(with an offset d
ei
). Two universal joints are located at F
i
(with an offset d
fi
) to provide orientation of the probe-support. The synchronized motion (i.e., same speed and direction) of two five-bar mechanisms provide translation motions to the tool part, while the unsynchronized motion provides rotation motions. During the rotational motion, the distance variation between the two universal joints F
i
is compensated by a passive translation joint located between the probe-support and F2. Actuator Q6 is attached on L14 to provide a rotation motion of the tool part along x0. The probe-support is considered as the wrist of MedRUE, and a reference frame
Given the joint values (q1 …, q b ), the forward kinematic solution of MedRUE can be obtained as follows:
Since A
i
and C
i
are static w.r.t.


where O i is the midpoint of Li0 with

and


where
With the coordinates of

where
and

where
Assuming the orientation of the wrist reference frame

where

where q DE 1 = atan2(−(y E 1 − y D 1 ), z E 1 − z D 1 ). The other two Euler angles are obtained by substituting Eq. (11) into Eq. (10):


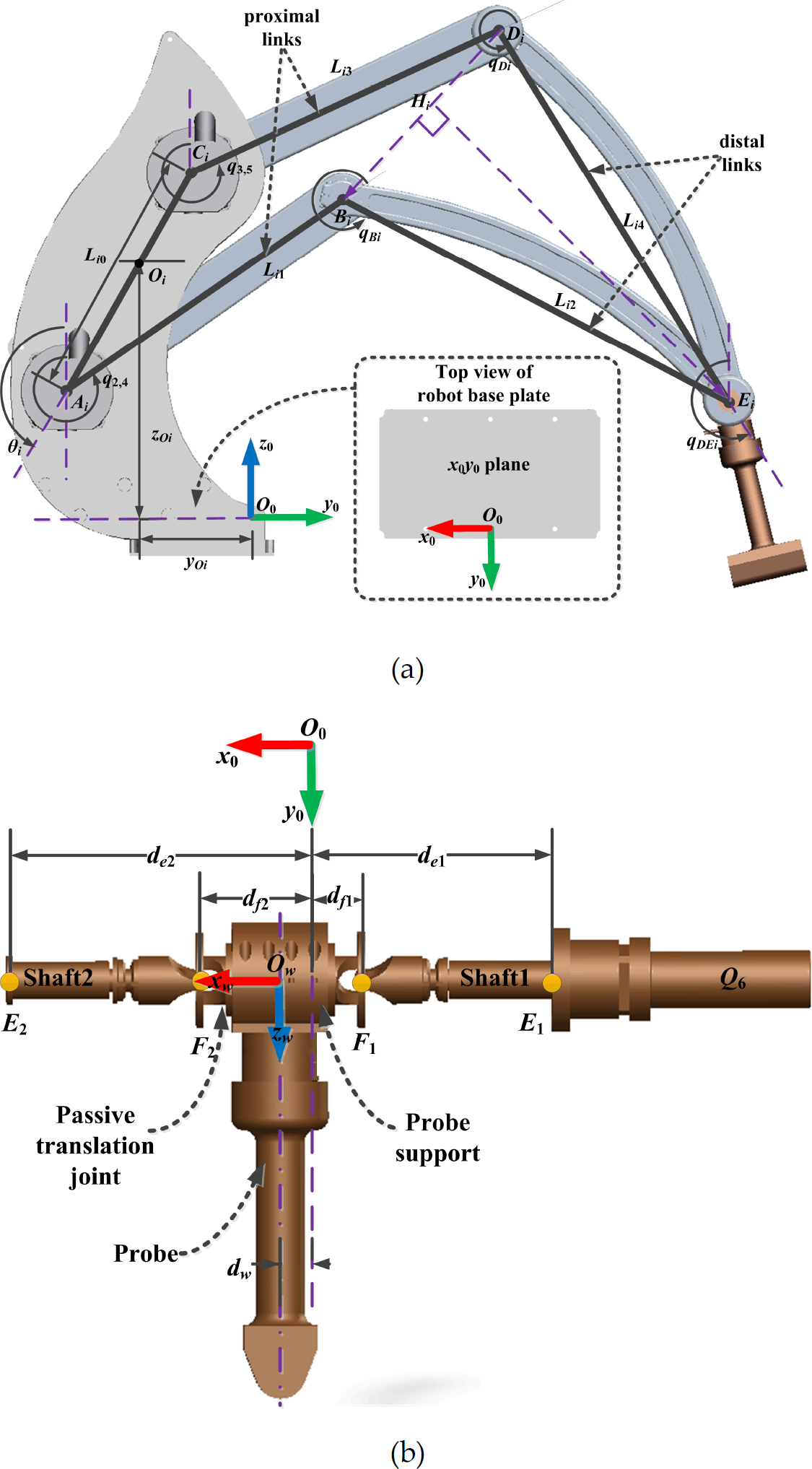
Kinematic model and parameters of MedRUE: (a) five-bar mechanism and robot base; (b) the tool part
Thus, the coordinates of O
w
w.r.t.

In our calibration process, a spherically mounted retrore-flector (SMR) is attached to the probe. The coordinates of the SMR centre w.r.t.

Assuming the transformation matrix from the world reference frame
where
In this section, robot repeatability and accuracy are assessed before calibration. Our assessment method is an adaptation of the international standard on robot performance and test method (ISO-9283) [29]. The nominal kinematic model (i.e., the model before calibration) is assessed in this section, and the calibrated kinematic model is validated in section 4.
In the nominal kinematic model [16], the corresponding parameters of the two five-bar mechanisms in Figure 2 are identical (e.g., l2j, = l2j, j = 0, …, 4). Moreover, each five-bar mechanism is symmetrically designed. In other words, the proximal links are identical (li1 = li3, i = 1, 2), and so are the distal links (li2 = li4, i = 1, 2). The offset joint values are considered to be equal to zero.
Robot path design and measurement points
In our implementation, the position accuracy has the priority since it is required both for safety reasons and 3D reconstruction. Orientation errors can be compensated in the 3D reconstruction with well-developed techniques, such as scale-invariant feature transform. In this article, only the position repeatability and accuracy are studied, while the orientation is kept constant during the measurement procedure. Before taking measurements, it is necessary to define the robot trajectory and the measured positions during data acquisition.

The measurement points in the workspace of MedRUE: (a) measurement points definition, (b) measurement path
Knowing that the robot is dedicated to lower limb scans, the effective robot's workspace is considered to be a half-cylinder, which covers the top surface area of a patient's leg. As shown in Figure 3(a), nine measurement points P
i
(i = 1, …, 9) are considered in this target workspace. Namely, eight corners C
j
(j = 1, …, 8) are created on both sides of the target workspace and form two planes C1C2C7 C8 as well as C3C4C
5
C6. Point P1 is located at the barycentre of all eight corners. Point P2 is defined on the vector
The used measurement path is an extension of the path design proposed in [30]. The robot end-effector is initially located at P1 and trajectory of the robot end-effector is demonstrated in Figure 3(b). When the process started, the robot end-effector followed the trajectory on the plane C3C4C5 C6, which is composed of the sequence P9 → P1 → P8 → P1 → P7 → P1 → P6 → P1.Then, the robot trajectory continues on the plane C1C2C7 C8, and follows the sequence P5 → P1 → P4 → P1 → P3 → P1 → P2 → P1 to finish a measurement cycle. In our experiment, 30 measurement cycles are taken.
In this method, P1 is visited from eight different directions, while all other measurement points are visited in a unidirectional approach (direction from P1). Thus, the experiment design is used to estimate multidirectional repeatability at position P1 and unidirectional repeatability at positions P2 to P8.
At each measurement point P
i
(i = 1, …, 9), the position of the end-effector is measured n times, where n = 8 directions × 30 cycles = 240 at P1 and n = 30 at each of the other eight measurement points. A set of n measurements on a measurement point P1 is called a cluster of P
i
. For any cluster, the barycentre is defined as a virtual point whose coordinates


The distance between the ηth cycle measurement at P i and the barycentre of the cluster of P i is

Then the repeatability at P i is defined as follows:
where and
The absolute position accuracy of P i is defined by

where
MeRUE will be used to take US images at prescribed intervals. These US images will then be used to reconstruct the 3D model of the blood vessel. For the purposes of medical examination, the accuracy in measuring the position of a given US image is important w.r.t. the neighbouring images. In other words, the relative accuracy is important for our robot.
A relative position accuracy of a point can be defined as the accuracy of the distance between adjacent points (e.g., the distance accuracy between P1 and P2). Since each point P i (i = 2, …, 9) is reached starting from P i in Figure 3(b), the nominal relative displacement of P i (i = 2, …, 9) is calculated as follows:

where

where δi =
The measurement setup is shown in Figure 4. The measurements are taken with a Faro Laser Tracker ION having a distance accuracy of 8 μm + 0.4 μm/m, and angular accuracy of 10 μm + 2.5 μm/m. The emitted laser is reflected by an SMR, which is magnetically attached to a nest. In our experiment, the target measurement is a 1.5 inch SMR mounted on the tool part (Fig. 4). The measured positions are expressed w.r.t. the laser reference frame (
We note that the measurement accuracy might be influenced by many aspects, such as environment, duration of operation, and the distance between the target and the laser tracker. Therefore, we evaluated the laser tracker accuracy for our own setup. A calibrated bar with a known length was measured ten times, and the distance error was found to be 26 μm ± 14 μm with 95.4% confidence interval of uncertainty. However, the measurement uncertainty was reduced by taking several measurements at each position.

Experiment setup of MedRUE positioning performance assessment and calibration
The results for the position repeatability at the nine measurement points are shown in Table 1. The first row shows the composed repeatability defined in Eq. (21), and the other three rows list the repeatability according to the x, y and z axes. Naturally, the position repeatability at P1 is worse, which is mainly because the arrivals at P1 are from eight different directions. Furthermore, the position repeatability along x at P1 is poorer than along y and z. This is caused by the fact that the motion along the x axis is dominated by the linear guide, which has a backlash of 76 μm according to its manufacturer.
Position repeatability (in μm)

Absolute position accuracy (APA) and relative position accuracy (RPA) before calibration (in mm)

The results for the repeatability at P1 in the two measurement planes (i.e., planes C1C2C7 C8 and C3C4C5C6) are illustrated in Figure 5. On each plane, there are four groups (G1 G2, G3, G4) of data in different colors indicating four different directions to reach P1 The measured data are illustrated with an asterisk marker, while the barycentre of each group is a solid circle. The cluster groups are clearly separated from each other. The divergence of measurement on P1 shows the imperfection of the multidirectional movement caused mainly by the backlash of the mechanical parts of our robot.
The position absolute accuracy and relative accuracy before calibration is given in Table 2. As an early prototype, the robot's poor accuracy is mainly due to its manufacture and assembling errors. The worst case of the absolute accuracy before calibration is about 6 mm, while the worst relative accuracy before calibration is about 3 mm.
In this section the proposed calibration approach is explained. The actual values of the robot parameters are identified to improve robot accuracy.
Kinematic parameters

Kinematic parameters
The parameters expected to be identified are summarized in four groups, as shown in Table 3. Parameters in Group 1 define
The world reference frame

The transformation matrix of

where vector

For convenience, all the further measured positions, in this paper, are implicitly expressed w.r.t.
Frame

The origin O0 of

where

where x
W
, y
W
, z
W
, ³
W
, β
W
and α
W
are the

Measurements at P1 for arrivals from multiple directions: (a) on measurement plane C3C4C5C6, view in xy plane; (b) on measurement plane C3C4C5C6, view in xz plane (c) on measurement plane C1C2C7C8; view in xy plane (d) on measurement plane C1C2C7C8, view in xz plane
The objective of this subsection is to evaluate the difference between the nominal and the real joint offsets. Active joints q2, q3, q4 and q5 are considered. As mentioned earlier, the five-bar mechanisms are symmetrically assembled, and therefore are calibrated with the same method. For simplicity, only the calibration of the second five-bar mechanism is demonstrated.
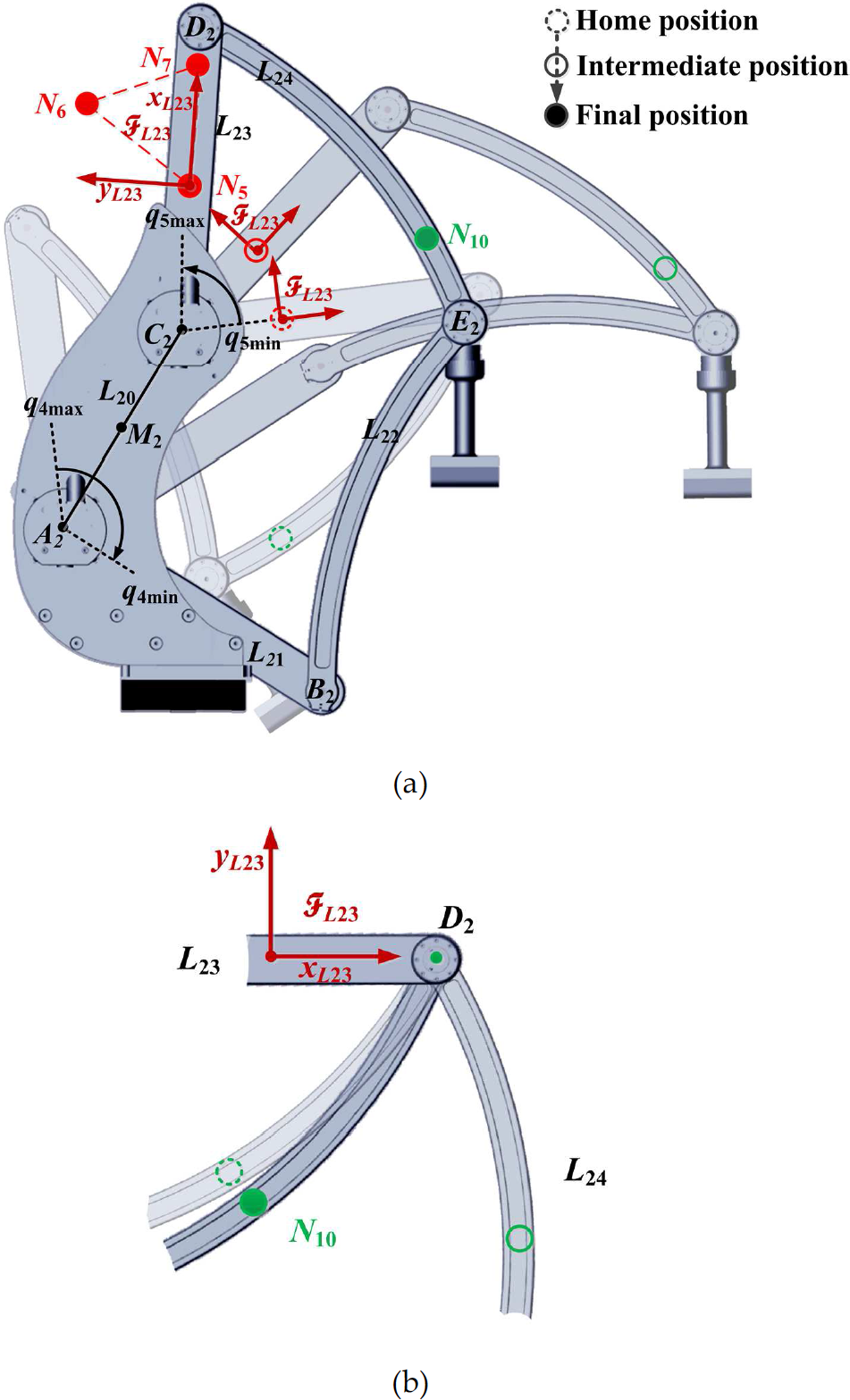
As shown in Figure 6, ten nests (N i , i = 1, …, 10) are attached on the five-bar mechanism for measurement purpose. Four nests (Ni, i = 3, 4, 7, 10) are used in this experiment, and the remaining nests are used to identify other parameters.

Experiment setup for active joint offset value estimation (nests in orange) and link length estimation (nests in orange and blue) on the second five-bar mechanism
Active joint q4 directly drives the rotation motion of L21. Thus, the joint offset error of q4 is assessed via the evaluation of the orientation error of link L21 (Figure 2(a)). The orientation of L21 is determined by the coordinates of A2 and B2. Similarly, the joint offset error of q5 is assessed via the orientation of link L23, which is determined by the coordinates of C2 and D2. Two experiments are designed to obtain the coordinates of A2, B2, C2 and D2 at the robot home position. The joint offset errors are then evaluated.

Path planning in the experiment of active joint offset error (i=1, 2): (a) determine coordinates of A i and D i , (b) determine coordinates of B i and C i
The first experiment is designed to determine the coordinates of A2 and D2 (Figure 7(a)) as follows:
Two nests denoted N3 and N10 are attached to links L21 and L24 respectively, as shown in Figure 6 and Figure 7(a).
The robot starts from its home position, which is illustrated with the highest transparent image in Figure 7(a). The angle of joint q4 is increased gradually with a step of 2°, within a range of 130°. Meanwhile, link L23 is kept in its home position throughout the experiment process. At each motion step the robot motion is halted, and measurements of N3 and N10 are taken.
The measured positions of N 3 and N10 — which follow circular curves centred at A 2 and D2 respectively — are fitted to two circles [31] in order to determine the coordinate of A 2 and D2.
For illustration purposes, an intermediate position of MedRUE is illustrated with intermediate transparency, and the opaque image shows the final position of MedRUE. The nests N 3 and N10 are demonstrated with a dashed circle, solid circle and filled circle in these positions, respectively.
To determine the coordinates of B 2 and C2 we used the same approach as for A 2 and D2. The used nests are denoted N4 and N7, and are attached to links L22 and L23 respectively, as shown in Figure 6. The experiment is illustrated in Figure 7(b).
As shown in Figure 2(a), the coordinates of A2 and B2 evaluate the orientation of links L21 in the y0z0 plane. The orientation of the link L21 is driven directly by active joint ˜4. Thus, the joint offset ˜4 is represented by the difference between the nominal value q4 and the evaluated orientation of L21 at the home position:

where yA2 and zA2 are the y and z coordinates of A2 w.r.t.

The active joint offsets of q2 and q3, related to the first five-bar mechanism, are assessed similarly to q4 and q5, by using the coordinates of A1 B1, C1 and D1.
The assembling parameters are yO1, zO1, yO2, zO2, θ1, θ2 and these describe the assembly of the two five-bar mechanisms on the robot base. The ith (i = 1, 2) five-bar mechanism is assembled on the robot base at joints A i and C i . As shown in Figure 2(a), O i is the middle point of link Li0 defined by A i and C i . Angle θ i illustrates the orientation of link Li0 in y0z0 plane. Knowing that the coordinates of A i and C i are obtained in the previous subsection, the assembling parameters are calculated as follows:


Experiment to assess the link length l23 (a) link reference frame and nests displacement during robot motion (b) trajectory of nest N10 w.r.t. to link reference frame
The assessment of the link length parameters is demonstrated using the second five-bar mechanism (i.e., l20, l21 l22, l23 and l24), while those for the first mechanism (i.e., l10, l11, l12, l13, l14) are obtained similarly.
The link length of L20 is determined by using the coordinates of A2 and C2 w.r.t.

The identification of l21, l22, l23 and l24 is carried out by moving simultaneously joints q5 and q4 inside their limit ranges, as shown in Figure 8(a).
Note that link L20 has both endpoints A2 and C2 fixed w.r.t.
The coordinates of B2 and E2 w.r.t.

To validate the proposed calibration method, we perform the same experiment with nominal and calibrated parameters. Both the nominal and identified values of calibrated parameters are listed in Table 4.
Nominal and identified parameter values

Nominal and identified parameter values
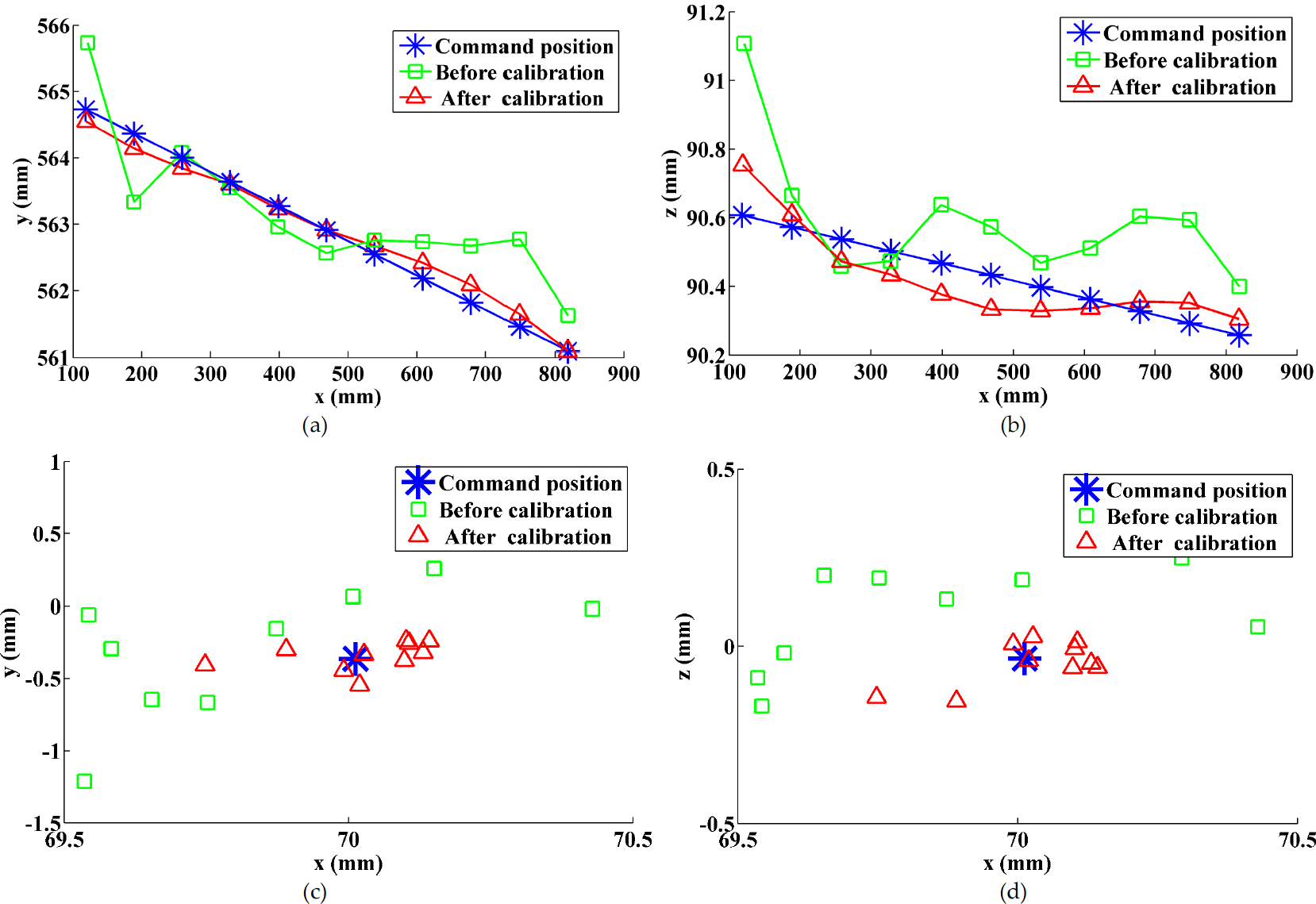
Accuracy improvement in tracking a reference (command) line: Absolute accuracy improvement by observing the trajectory in xy plane (a) and xz plane (b); Relative accuracy improvement in xy plane(c) and xz plane (d)
MedRUE is an early prototype of a medical US robot, and there are many imperfections in its manufacture and assembling. As we can see in Table 4, there are noticeable differences between the nominal parameter values and the calibrated parameter values. The majority of errors come from the assembling of the two five-bar mechanisms on the robot base. Furthermore, the manual nest setup (as in Figure 4) for
The robot's position accuracy assessment after calibration obtained using the ISO 9283 evaluation approach is shown in Table 5. The maximum absolute position error (i.e., absolute accuracy) has been improved from 5.770 mm before calibration to 0.764 mm after calibration. The relative accuracy is also important in medical application, and its accuracy is satisfactory after calibration. The maximum relative position error was improved from 3.018 mm before calibration to 0.489 mm after calibration, as shown in Table 5.
Figure 9 illustrates the improvement of accuracy when the robot is tracking a reference command line, which is marked in a blue solid line. As shown in Figure 9(a) and Figure 9(b), which represent the trajectory projection on planes xy and xz, respectively, the trajectory before calibration has a significant error (poor absolute accuracy), and it is greatly improved after the calibration.
Figure 9(c) and Figure 9(d) illustrate the relative position offset between adjacent points. Since the reference command line is created by a set of points with constant offsets, the relative position offsets are represented as a fixed point (illustrated by an asterisk). The obtained offsets before calibration are illustrated by green squares: ideally all these squares should coincide with the reference offset (i.e., the blue asterisk mark). However, they scattered around the reference offset because of the robot parameter residuals. The obtained results (offsets) after calibration are illustrated in red triangles and it clearly demonstrates the improvement of the robot relative accuracy: i.e., the obtained relative position offsets converge towards to the reference offset.
Absolute position accuracy (APA) and relative position accuracy (RPA) after calibration (mm)

The calibration method demonstrated in this section can be used for many other kinds of serial or parallel robots as well. As it is based on direct measurements, it provides more accurate parameter identification than conventional standard calibration methods based on optimization (e.g., forward calibration and reverse calibration method). The proposed method also requires no complex computation (e.g., identification Jacobian matrix, observability analysis) or advanced optimization knowledge in calibration. The comparison between proposed calibration method and standard calibration method are summarized in Table 6.
Comparison of proposed calibration method and standard calibration method

An assessment method of the repeatability and the accuracy of a new medical robot were presented. The complete kinematic model of the robot was introduced, and the corresponding parameters were calibrated by a direct measurement method. The proposed method is very easy to implement and requires minimum knowledge of advanced calibration techniques. This approach was validated through experiments which demonstrated a significant improvement of the position accuracy from about 6 mm before calibration to less than 1 mm after calibration. Thus, the presented method has great potential value in robot calibration when advance techniques are not available or not necessary.
Footnotes
6.
The authors thank the Canada Foundation for Innovation and the Fonds de recherche du Québec sur la nature et les technologies, who provided the funding for this project.