
Abstract
Most of the literature on healthcare digitalization is focused on the benefits, the barriers and the determinants of the adoption of ICT-based solutions within hospitals. Little is understood about how hospital digitalization can be accomplished or how this digitalization fosters an increase in hospital performance — both in terms of quality improvement and cost rationalization — by ambidextrously combining the exploration and exploitation of hospital assets. This paper sheds a preliminary light on the topic, identifying a set of action-oriented propositions for smart healthcare digitalization within hospitals.
1. Introduction
In today's information-intensive economy [1] Information and Communication Technology (ICT) plays a pivotal role not only in enabling firms to achieve operational excellence [2] but also in facilitating strategic competitive advantage [3]. The progressive digitalization of all industries — from fast moving consumer goods [4] to the insurance sector [5], from aerospace [6] to traditional manufacturing firms [7], from fashion and apparel [8] to inter-freight transportation [9] —provides consistent opportunities to disrupt the way value is created [10,10], transferred [12,12] and defended against competitors [14,14].
The healthcare industry is not an exception to this trend of ICT utilization [16]–[19]. The digitalization of healthcare assets is widely considered one of the most effective answers to the growing pressures of augmenting the quality of healthcare ecosystems while simultaneously reducing their cost [20]–[22]. In fact, ICT offers opportunities to conciliate the capability to exploit current assets with the capability to shift away from them in order to explore new and better ways of delivering value [23]. According to the ambidexterity literature (e.g., [24]–[26]), the ambidextrous balance of these exploitatory and exploratory activities produces overall improvements in both quality enhancement and cost rationalization — even when under specific boundary conditions [27] or through a continuous set of efforts [28].
Despite the emergence of asset digitalization as one of the most promising ways of unfolding ICT's ambidextrous potential within the domain of healthcare [29], the results of the digitalization efforts accomplished within it often fall well below expectations. Unfortunately, most hospitals:
Continue to give healthcare digitalization barely a second thought as a source of innovation [30]; and
Do not adequately analyse the organizational changes required to make all the benefits associated with the digitalization become a reality [21].
The literature, in fact, does not provide them with clear guidance, since previous contributions on healthcare digitalization have largely focused on the benefits, the barriers and the determinants of the adoption of ICT within hospitals [21]. Very little is known about how asset digitalization is accomplished within hospitals or how this digitalization might contribute to effectively increasing both the exploration and the exploitation of hospitals' assets, thereby in improving their performance.
Given this background, this study offers new insights into how to solve the quest for systematically improving hospitals' performance by enhancing and ambidextrously balancing exploration and exploitation capabilities through asset digitalization. Formally, the research question that forms the basis of the investigation is as follows: How can hospital digitalization unfold an effective balance of the exploration and exploitation of hospital assets? (By «effective balance» we mean an ambidextrous balance which is able to increase hospitals' performance — both in terms of quality improvement and cost rationalization).
2. Research Methods
The research is rooted in the activities of the ICTs in the Healthcare Observatory — a permanent research initiative which, since 2007, has been addressing the topic of how healthcare stakeholders can strategically use ICT in order to cope with the issues characterizing the healthcare industry. The reader might refer to [31] and [32] for a description of the overall participative, evolutionary, longitudinal and multi-methodological framework utilized by the Observatory.
In order to answer the research question, an interpretative, inductive perspective [33], based on multiple and embedded case studies [34] was considered appropriate. The interpretative, inductive perspective is useful because the research question aims to better understand the complex dynamics underlying hospital digitalization — retaining «the holistic and meaningful characteristics of real-life events» [35]. The paper relies on multiple cases because they tend to yield to more generalizable, robust and parsimonious results than single cases [36]. The embedded unit of analysis has been selected to not only better measure the performance of the digitalization strategy, but also to diminish the probabilities of conducting the research at an abstract level [32,32].
After the selection of the main research method, the authors focused on the definitions of the constructs to be used. The definitions of exploratory and exploitatory activities are a specialization within the healthcare context of the definitions provided by [24] in his seminal paper:
Exploratory activities: activities that explore new and better alternatives to deliver healthcare services — regarding both the administrative and clinical domains — in order to change existing routines;
Exploitatory activities: activities that refine and extend existing healthcare competences, simplifying the use of existing routines in both the administrative and clinical domains.
Both of these definitions are based not only on literature analysis but also on the suggestions — provided through social agreement [38] — of a group of more than 60 practitioners that have also defined, together with the authors and other researchers working in the Observatory, not only a taxonomy of the ICT-based solutions that a hospital can adopt, but also a classification of those explicitly focused on the digitalization of healthcare assets. Table 1 reports the different solutions which emerged from this collaborative effort.
ICT-based solutions adopted by a generic hospital

The four overarching areas of ICT-driven innovation have been defined by the authors of the paper through a deep analysis of the literature and a focus group with a multidisciplinary group of more than 60 practitioners among which: C-levels of the principal Italian hospitals, national and international health technology suppliers, professionals from national and international healthcare associations, and healthcare experts
Four hospitals in Lombardy have been considered on the basis of their strategies for increasing their performance — both in terms of quality improvement and cost rationalization — by leveraging on their capabilities to explore and exploit through the digitalization of their assets. Table 2 reports some details of the hospitals, which have been selected through a theoretical sampling [33]–[36] based on a convenience principle and a polarization approach. The underlying idea associated with these choices is to sample the appropriate cases so as to more easily observe any contrasting patterns in the data [34,34].
Details of the hospitals included in the research
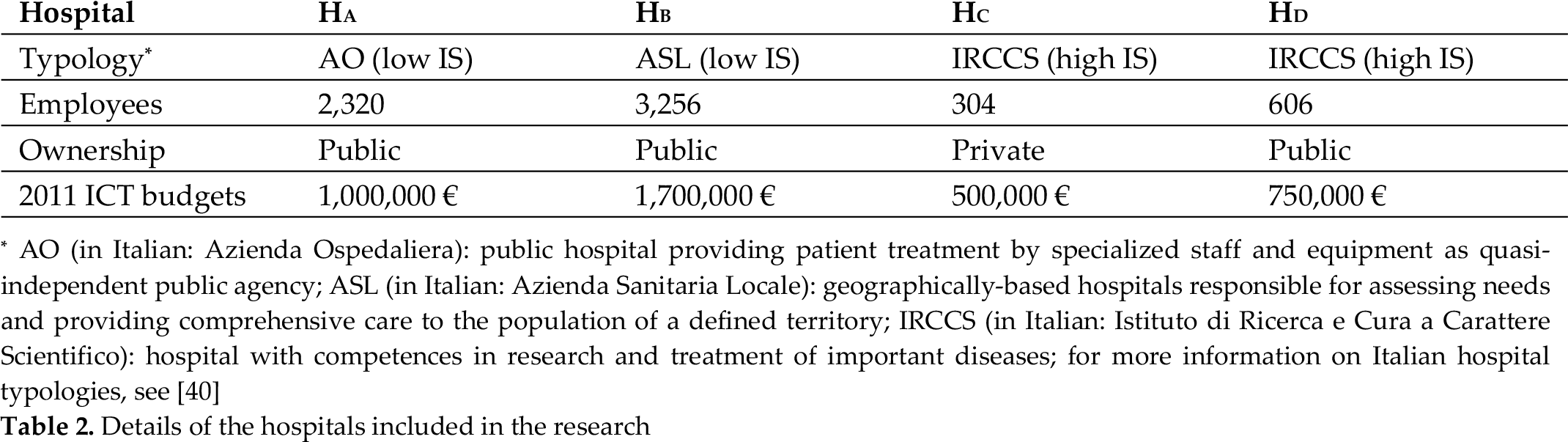
AO (in Italian: Azienda Ospedaliera): public hospital providing patient treatment by specialized staff and equipment as quasi-independent public agency; ASL (in Italian: Azienda Sanitaria Locale): geographically-based hospitals responsible for assessing needs and providing comprehensive care to the population of a defined territory; IRCCS (in Italian: Istituto di Ricerca e Cura a Carattere Scientifico): hospital with competences in research and treatment of important diseases; for more information on Italian hospital typologies, see [40]
The convenience principle is reflected in the selection of the hospitals, which — as can be seen in Table 3 — were all highly focused on the digitalization of their assets during the period of analysis. The polarization approach is associated with the efforts that a hospital has to make in overcoming the exploration-exploitation dichotomy limiting its performance. In fact, the literature (e.g., [39]) suggests that the progressive rendering which is a salient aspect of the underlying tensions between exploratory and exploitatory activities provides opportunities to tackle deeper interrelated tensions, whether latent or not yet present.
ICT-based solutions in the four hospitals analysed
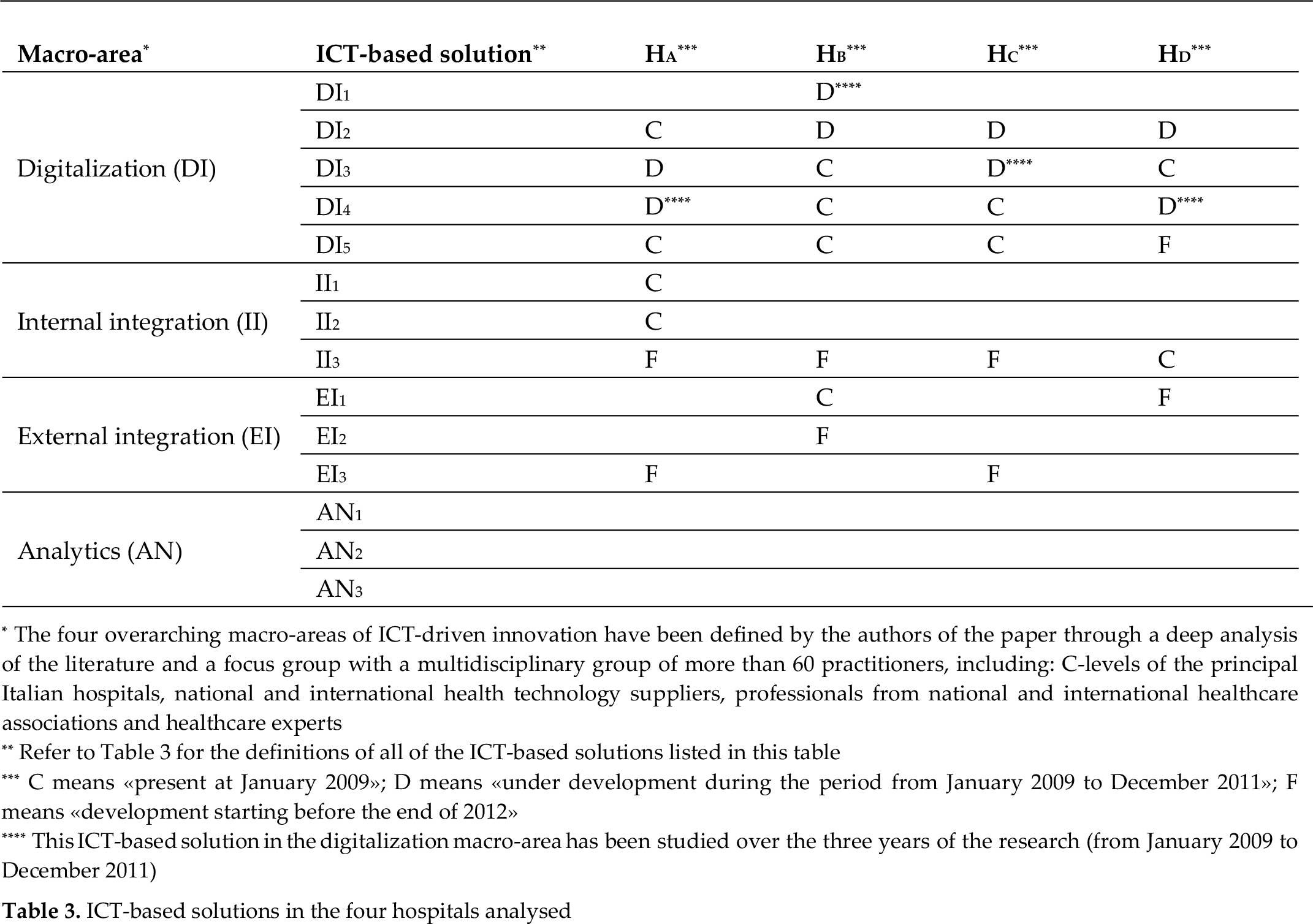
The four overarching macro-areas of ICT-driven innovation have been defined by the authors of the paper through a deep analysis of the literature and a focus group with a multidisciplinary group of more than 60 practitioners, including: C-levels of the principal Italian hospitals, national and international health technology suppliers, professionals from national and international healthcare associations and healthcare experts
Refer to Table 3 for the definitions of all of the ICT-based solutions listed in this table
C means «present at January 2009»; D means «under development during the period from January 2009 to December 2011»; F means «development starting before the end of 2012»
This ICT-based solution in the digitalization macro-area has been studied over the three years of the research (from January 2009 to December 2011)
To generalize this idea, it is possible to introduce the concept of innovation stickiness (IS), which is represented in Figure 1 and can be defined as the incremental efforts made by the hospital in order to render salient and solve the tensions between the exploratory and exploitatory activities conducted over its assets.
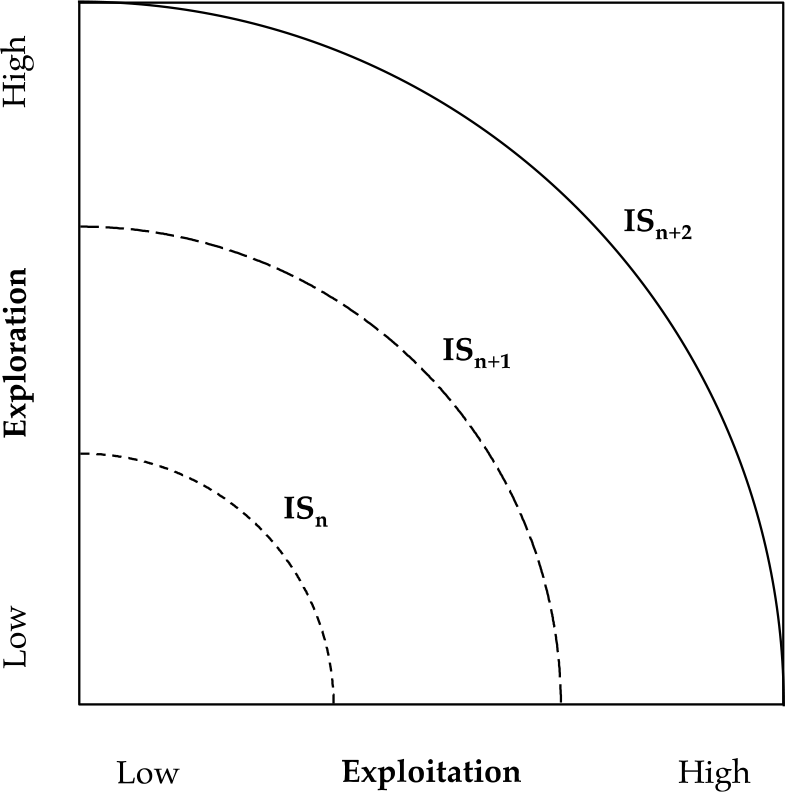
Incrementing levels of innovation stickiness (IS)
When innovation stickiness is low (ISn in Figure 1), the opportunities to overcome the exploration-exploitation dichotomy are greater. When innovation stickiness is high (ISn+i and ISn+2 in Figure 1), further effective combinations of exploration and exploitation are not easily achieved. In the context of this paper, the authors have assigned high IS to the IRCCSs, which not only have certified competences in the research and the treatment of important diseases but also a double control — by the regional healthcare council and the Italian Ministry of Health — over their expenditures [40]. Half of the sample is constituted by IRCCSs, while the other half is constituted by ASLs and AOs — with theoretically less emphasis on exploring and exploiting (refer to Table 2 for the definitions of IRCCS, ASL and AO).
According to [35], a major step in designing and conducting a case-based research is the definition of the unit of analysis (or the case itself). Starting from the research question, as well as from the analysis of the literature, the focus on the digitalization process as a first unit of analysis has been chosen. By ‘digitalization process’ this paper means the set of activities and users involved in the adoption, usage and improvement of the ICT-based solutions used to digitalize the assets of the hospital.
This unit of analysis provides a privileged viewpoint to understand the support delivered to the exploratory and exploitatory activities of these hospitals' assets. In order to improve the likelihood of a rich, accurate theory [28,28], and to better measure the performances achieved through digitalization, the hospital itself has been considered as a second unit of analysis.
As suggested by [37], the research relied on several data sources: face-to-face interviews, phone conversations, follow-up emails and archival data, such as internal documents, press releases, websites and news. The primary data source is composed of 30 semi-structured interviews conducted over three years with the Chief Information Officers (CIOs), at least one of the other C-levels and — through a snowball technique [41] — other knowledgeable informants involved in the digitalization process. Within each hospital, the authors continued recruiting informants until additional interviews failed to dispute existing – or reveal new – categories or relationships; that is, up until theoretical saturation [42] was achieved. Table 4 summarizes the informants involved in the research.
Informants involved in the research

Each interview lasted approximately 1.5 hours; most of the interviews were performed face-to-face
The interviews have been designed on a common protocol that evolved systematically during the research. A key advantage of the study is its three waves of data collection [43]. In the first wave, an emphasis has been placed on the different ICT-based solutions present inside the hospitals. The main information achieved is synthesized in Table 3. In the second and third waves of interviews, an emphasis has been placed on the main digitalization strategies followed in each hospital and — as the data collection and analysis unfolded — the interviews became increasingly focused [44] on the activities and the users involved in the adoption, usage and improvement of specific ICT-based solutions that digitalized the assets of the hospitals, as well as on the relationship between the usage of these solutions and the exploration and/or exploitation of hospital assets.
Following recommendations for multiple case theory building [36], within- and cross-case analyses were performed with no a priori hypotheses. The corresponding author built a first draft of the individual write-ups which triangulated all of the data so as to emphasize themes that were supported by different data collection methods and confirmed by several informants [36]. The other authors integrated the first draft with their comments and highlighted missing details that were successively filled-in with phone calls and emails [43]. Once the write-ups were consolidated, each author read them so as to form an independent viewpoint [35] and develop the preliminary concepts and rough theoretical explanations. Finally, a cross-case analysis was done — using replication logic across the cases — in order to look for alternative theoretical relationships and con-structs that might fit the data better than the initial emergent theory [45]. Tables and other cell designs were used to compare several possible constructs at once [46]. From the emerging constructs and themes, tentative relationships between the constructs have been formed. Next, these initial relationships were refined via replication logic — frequently revising each case so as to compare and verify the occurrence of a specific construct, relationship or logic [43].
Once the cross-case analysis was underway, the authors cycled through the emergent theory, case data and literature in order to further refine the emerging construct definitions, abstraction levels, construct measures and theoretical relationships [45]. The cycles continued until a strong match between the cases and the emergent theory was achieved [43]. To converge on a parsimonious set of constructs, the researchers focused only on the most robust findings [44], asking the informants of the four hospitals to review them in order to solve any discrepancies.
3. Research findings
For each digitalization process, Table 5 and Table 6 offer a summary: (i) the hospital in which it was accomplished, (ii) the related ICT-based solution drove the digitalization process, (iii) the stimuli that led to the decision of investing in this solution, (iv) the problems faced during its adoption, (v) the impacts upon the exploration, exploitation and performance of the hospital, (vi) the approaches utilized to ambidextrously combine the exploratory and the exploitatory activities related to the ICT-based solution, (vii) the challenges and the issues faced during its usage and/or improvement, (viii) the next steps to be accomplished according to those informants interviewed, and (ix) some of their quotes which are felt to be representative of the elements depicted in the tables. To complement the analysis, it is useful to refer to Table 3 for an overview of the other ICT-based solutions that were already present inside the hospitals when they decided to start the digitalization processes presented in Table 5 and Table 6.
Main findings of the interviews performed on the digitalization processes of HA and HB

Each statement in the table has been rated on a 10 point Likert scale in order to measure its importance (0 = not important; 10 = highly important); the number in the squared brackets indicates the average importance provided by the informant in the last round of interviews; the table presents only those statements that have achieved an average importance rate higher than 7.0
According to the CIO, the problems indicated by «Major» risked the compromise of EMR adoption; the problems indicated by «Minor» do not constituted great threats from this viewpoint
For each impact, the CIO has indicated its main nature (ER = exploratory impact; EI = exploitatory impact) and its grade of innovativeness (RI = radical innovation; II = incremental innovation)
Only the main approaches adopted in order to ambidextrously balance exploratory and exploitatory activities are reported in the table; organizational differentiation means that exploration and exploitation occur simultaneously but are situated within distinct units [48]; domain differentiation means that each unit specialises in exploratory or exploitatory activities in a particular domain (e.g., standard patient treatment vs. acute patient treatment) while the hospital balances these activities across domains [25]
According the CIO, the next steps indicated by «Major» had to be accomplished as soon as possible; the next steps indicated by «Minor» were subject to the presence of further ICT budgets
Main findings of the interviews performed on the digitalization processes of HC and HD

Each statement in the table has been rated on a 10 point Likert scale in order to measure its importance (0 = not important; 10 = highly important); the number in the squared brackets indicates the average importance provided by the informant in the last round of interviews; the table presents only those statements that have achieved an average importance rate higher than 7.0
According to the CIO, the problems indicated by «Major» risked compromising EMR adoption; the problems indicated by «Minor» do not constituted great threats from this viewpoint
For each impact, the CIO has indicated its main nature (ER = exploratory impact; EI = exploitatory impact) and its grade of innovativeness (RI = radical innovation; II = incremental innovation)
Only the main approaches adopted in order to ambidextrously balance exploratory and exploitatory activities are reported in the table; temporal differentiation means that the hospital switches between exploration and exploitation over time; organizational differentiation means that exploration and exploitation occur simultaneously but are situated within distinct units; for more information refer to [25]
According to the CIO, the next steps indicated by «Major» had to be accomplished as soon as possible; the next steps indicated by «Minor» were subject to the presence of further ICT budgets
With reference to Table 1, and similarly with latest literature (e.g., [47]), all of the informants agreed on the fact that the first ICT investments in the healthcare domain should be accomplished within the macro area of digitalization. With the exception of the tools supporting service management and delivery (DI1) — not strictly necessary and useful only when a hospital has complex and/or big facilities — all the other ICT-based solutions that were grouped under the digitalization area, in Table 3, were not only almost “mandatory”, but they were also a pre-requisite of any further ICT-driven innovation process. In the words of the informants: «It's really difficult to capture the benefits of ICT-driven innovations such as Electronic Medical Record or Analytics without a preliminary set of investments in infrastructure and digitalization. Without a digital backbone, today a hospital is simply unavailable to generate value» (CEO of HA).
As it is possible to see in Table 5 and Table 6, in all of the cases the initial objectives of the investments in digitalization were related to a willingness to better exploit the resources in the hands of the hospital and achieve efficiency — mainly in terms of cost and time savings or managerial simplification. These tendencies find confirmation in the other cases accomplished outside the Lombard context by the Observatory. For example, a CIO of a medium-sized AO in the North-East of Italy told the authors that: «Most of [the] hospitals start with the dematerialization of radiology and [its] laboratory for the tons of savings it is possible to achieve in terms of resources and time».
A common element emerging from the cases is that it is better to focus on the digitalization of one hospital unit at a time, not only to achieve - in short time lags – the tangible results to be shown to both the strategic board the users, but also to avoid the «over-complications associated with the development of pervasive ICT-based solutions — at least in the initial digitalization stages and/or in the case of [the] low ICT budgets available» (CIO of He). Moreover, the rest of the hospital can continue along its path to solve the dichotomy present between the exploration and exploitation of other hospital assets —making the ambidextrous balance of exploratory and exploitatory activities comprehensively more easily achieved.
This evidence makes an initial contribution to both the literature and the practice of the management of digitalization processes in the domain of healthcare. If the importance of healthcare digitalization is increasingly emphasized (e.g., [21] or [47]), then as far as the authors know there are no indications regarding where to start the digitalization path of hospital assets. From this viewpoint, it is possible to state the following proposition:
P1: The first effective ICT investments within a hospital support exploitatory-based digitalization paths — performed one hospital unit at a time — with the aim of achieving efficiency in the management of hospital assets.
According to the informants, digitalization in the clinical domain is typically preferred to digitalization in the administrative domain. In the opinion of the chief radiologist in HA, the reasons «are mainly related to the higher value associated with clinical digitalization». In fact, most of the assets that can be digitalized within a hospital have a clinical nature. Informants not only confirmed this point, but also underlined that clinical digitalization provides more opportunities to both explore and exploit. In the words of the CMO of HB: «clinical data provides you [with] many more opportunities to both revise the existing paths through which the service of our organization is delivered to our patients, as well as to change and improve these paths. Administrative processes are simply not as pervasive as [the] clinical processes in a hospital. It's a matter of impact». Moreover — as described by the informants of the cases in Table 5 and Table 6 — digitalization in the clinical area produces a stronger positive impact on the performance of the hospital — both that performance directly perceived by physicians (HA) and the patients (HD), as well as that not directly perceived by most of the stakeholders (HC). Thus, the following proposition can be made:
P2: Clinical digitalization is more likely to yield better results in effectively combining exploration and exploitation than is administrative digitalization.
To provoke further consideration, it is possible to recommend radiology and the laboratory as the first hospital departments to digitalize. As indicated by the CIO of HD: «radiology and [the] laboratory are document-intensive departments, mostly detached by the core services offered by their hospital, with technology-friendly physicians and many efficiency needs».
According to the two propositions introduced, a generic hospital aiming to perform a smart digitalization process — digitalization able to effectively combine the exploration and exploitation of hospital assets — can begin following in the clinical domain, the initial part of the path from 0 to ① in Figure 2. If almost all of the hospitals studied by the Observatory [20] began with this path, the analysis of this paper's cases allowed another interesting element to be highlighted.

Efficiency stimulus and ICT
After the appropriation of the main benefits associated with the initial digitalization investments, the ICT-based solutions introduced permitted the exploration of radical, new and better ways of pro viding healthcare services thanks to the integration of (i) the radiological devices in HA, (ii) the queue management systems in HB, (iii) the hardware and software virtualized in He, and (iv) the laboratory devices in HD. For example, HA began the digitalization of its radiology department mainly in order to reduce the usage of radiological films, to save storage space and to rationalize the other resources used in the unit. However, after a specific level of the exploitation of the benefits associated with the digital management of these assets, other opportunities emerged. For instance, the integration of the computed tomography with magnetic resonance imaging allowed radical, new and better ways of providing diagnoses.
Thus, an initial ICT investment supporting pure exploitatory activities and efficiency objectives opened up exploration possibilities that, once seized upon, allowed them to not only ambidextrously balance exploratory and exploitatory activities (the final part of the path from 0 to ① in Figure 2), but also to increase their overall performance — both in terms of cost rationalization and quality improvement (see Table 5 and Table 6). In other words, focusing on producing finding, analysing and sharing information through digital media [50], the ICT-based solutions used to digitalize hospital assets progressively manifest their ambidextrous potential for effectively balancing exploration and exploitation.
Again, the cases seem to suggest that the greater the detachment from the other units of the unit in which asset digitalization is accomplished, the smoother and the more effective the ICT-driven integration produced through this digitalization. Most of the problems encountered during the adoption, use and improvement of (i) the electronic queue management systems in HB and (ii) the virtualization realized in He, can be traced back to the pervasiveness of these ICT-based solutions and the number of processes (assets, activities, users) affected by the relative digitalization.
The discussions with the informants explained these observations mostly in terms of «[the] protection of the unit» (the CIOs of HA, HB and HC). In the initial digitalization stage, the more the unit is protected, the more effective the contribution provided by the process of digitalization. This summary suggests that:
P3: The ICT-based integration among the assets within a hospital unit realized through a digitalization process positively affects the ability of the unit to effectively combine exploration and exploitation — especially if the unit is protected.
A final consideration regards IS polarization. The comparison of the two pairs of cases with high and low IS suggests that the fewer the opportunities to overcome the exploration-exploitation dichotomy, the more urgent and complex the investments in digitalization. In fact, if HA and HB did not encounter major problems during the digitalization of their assets, the strong dependence of the processes of HD on its laboratory imposed various pressures on dematerializing laboratory assets as soon as possible, while the virtualization of HW devices and of the main clinical SW realized in He faced many difficulties, which can mainly be traced back to the introduction of the virtualized solution into the existing organizational processes.
An explanation of these findings is that, having the hospital already rendered as salient and having resolved most of the tensions between the exploration and the exploitation of its assets, further combinations of these forces are achievable only through high incremental efforts, shared among all the actors within the hospital [51]. The ICT-based solutions used in hospital digitalization allow leveraging on these system-oriented, shared efforts [52] and the digitalization of hospital assets is the first step that must be accomplished in order to develop effective ICT-driven innovations within a hospital. This is why digitalization is more urgent in the case of high IS than in the case of low IS.
Moreover, the higher the IS, the more each single unit of the hospital has already explored and exploited in the past and, thus, the more likely it is that the unit has found its balance between its exploratory and exploitatory activities [25]. Basically, the digitalization of the healthcare assets in the unit reconsiders this balance — forcing the unit to alter equilibriums developed in, and maintained through, years of experience. This is why digitalization is more complex in the case of high IS than in the case of low IS. Overall, the following proposition is suggested:
P4: The higher the IS, the more urgent and complex the digitalization of the assets within a hospital.
4. Conclusion
If well-managed, hospital digitalization allows the exploration of current assets and the exploration of new ways of using them, with the end result of tangible improvements in both quality enhancement and cost rationalization. However, the results of the digitalization processes accomplished within the hospital are tremendously variable and hospital managers experience pitfalls and shortcomings in their implementation. This study offers new elements to further the on-going debate about the ability of ICT to enable asset dynamics leading to more efficient and high-quality healthcare services. In particular, Table 7 outlines the main contributions of the achieved findings, which are relevant from a theoretical as well as an empirical viewpoint.
Theoretical and empirical contributions of the findings

From a theoretical perspective, this paper contributes mainly to the ambidexterity literature. First, it focuses on the role that a mostly unconsidered lever (ICT) can play in the exploration-exploitation dichotomy, showing that hospital digitalization can — under specific boundary conditions — foster an effective balance between the exploration and exploitation of hospital assets. Second, it contributes in shifting the traditional attention of ambidexterity researchers from the notion of balance itself to the process of balancing exploration and exploitation. The cases suggest that it is the focus on this balancing process that allows the increasing of hospital performance. Third, it introduces a theoretical construct (IS) that emphasizes the importance of the incremental efforts to be put in place in order to progressively render salient and solve the tensions between exploration and exploitation — suggesting not only the necessity of adopting different ambidextrous behaviours along the path towards hospital digitalization, but also the need to properly lead the transitions along these paths.
From an empirical perspective, the paper provides healthcare practitioners with clear guidelines to leverage on hospital digitalization in order to effectively combine the exploration and the exploitation of hospital assets and, thus, increase healthcare performance. The empirical insights flowing from the cross-case analysis are interesting and useful for (at least) the following actors in a typical hospital:
Those CIOs who need models to increase the exploratory and exploitatory impact of the digitalization processes performed within their hospitals;
Those CEOs who aim to learn more about how to encourage the successful digitalization of their hospitals;
Those CFOs who wish to not only use asset digitalization as a driver of cost reduction, but also as a tool to control the financial situation of their hospitals;
Those CMOs who are committed to exploiting asset digitalization in order to increase the quality of healthcare services offered in their hospitals.
The results at this stage are still preliminary and need to be further refined. However, the work represents a good starting point to frame the potential research that could be interesting to perform in the future. In fact, since the present work represents an exploratory research approach rather than a confirmatory or prescriptive one, the propositions that have been proposed can be further investigated and developed in the future. From this viewpoint, the main problem of this work's findings concerns their generalizability. The focus on a specific lever (asset digitalization), a specific industry (healthcare) and a specific context (Lombardy), combined with the extensive use of an interpretative logic risks producing «very idiosyncratic phenomena» [34] — it is not easily generalizable into other contexts.
There are two further developments already planned in order to fill this gap. First, it would be useful to combine the interpretative-oriented methodology used in this work with a more inductive and quantitative-oriented set of vertical studies that could formally test the effectiveness of the proposed contributions in all their detail. The second is a progressive extension of the research context to other healthcare systems — both Italian as well as European — in order to test the effectiveness of the propositions which emerged during the empirical analysis and see how the considerations achieved change according to the different contingent contexts of analysis tackled.