
Abstract
Psychiatric comorbidities are relatively frequent in people with epilepsy, occurring in one of every three patients, with mood and anxiety disorders predominating. They are the expression of a complex interaction between a previous psychiatric history (and/or genetic predisposition for psychiatric disorder), neurobiologic changes associated with the underlying epilepsy, peri-ictal phenomena, iatrogenic and reactive processes. Furthermore, a bidirectional relation between psychiatric disorders and epilepsy has added another level of complexity, while at the same time opening an opportunity of the recognition of potential pathogenic mechanisms that are responsible for the high comorbid occurrence of these disorders. This article highlights the clinical implications of understanding the course of psychiatric comorbidities relative to the onset of the seizure disorder to minimize their risk of recurrence and their interference in the management of the seizure disorder.
Psychiatric comorbidities (PCs) are relatively frequent in people with epilepsy (PWE); in fact, population-based studies have identified a lifetime history in about 30 to 35 percent of patients, with depressive and anxiety disorders accounting for a majority of these conditions (1). Despite their relatively high prevalence and the negative impact they have on the lives of PWE of all ages, PCs have gone undetected for a long time and, not surprisingly, are not being treated (1). Fortunately, in the last decade, neurologists have started to recognize the need to identify and treat PCs, in particular mood disorders, and have started to rely on the use of several screening instruments to identify symptomatic patients. Furthermore, governmental agencies such as the National Institutes of Health and the Centers for Disease Control and Prevention have designated PCs as benchmarks for research funding, while the screening for comorbid depression has been suggested as a measure of good practice by professional neurologic societies.
For a long time, PCs have been considered to be a “complication” of the underlying epilepsy or a “normal reaction” to the psychosocial obstacles associated with a life with epilepsy. Yet, population-based studies published in the last 2 decades have recognized that not only are PWE at an increased risk of developing PCs but also patients with PCs are at increased risk of developing epilepsy (2–8). In fact, PCs are the expression of a complex interaction between (a) a previous psychiatric history (and/or genetic predisposition for psychiatric disorder), (b) neurochemical, structural, and functional changes associated with the underlying seizure disorder, (c) peri-ictal phenomena, and (d) iatrogenic, and/or (e) reactive processes (see Figure). Notwithstanding the complexity of psychiatric phenomena, a significant percentage of clinicians taking care of PWE and investigators of PC rely on screening instruments to identify PWE with PC. Most screening instruments detect the existence and quantify the severity of individual psychiatric symptoms present during a period ranging between 2 and 4 weeks (depending on the instrument), but by themselves none establish the existence of a specific psychiatric disorder. A few instruments have been developed to screen for specific disorders (e.g., the Neurologic Disorders Depression Inventory in Epilepsy [NDDI-E] for major depressive episodes [MDE] in PWE [9]), but a more in-depth evaluation is always recommended to confirm the diagnosis and establish the duration and the existence of other PCs, which is a common occurrence, particularly in the case of mood and anxiety disorders. In this article, we will highlight the significance of early identification of the lifetime psychiatric history of PWE, preferably at the time of the initial evaluation of the seizure disorder. Such data can help minimize the risk of recurrence of future interictal psychiatric episodes, recognize peri-ictal psychiatric symptomatology, avoid the development of iatrogenic psychiatric adverse events as well as of stress-induced seizures, and finally, help us appreciate the impact of PCs on the response to treatment of the epilepsy. This article will focus in particular on mood disorders, as together with anxiety disorders they are the most frequent and better studied PCs in epilepsy.
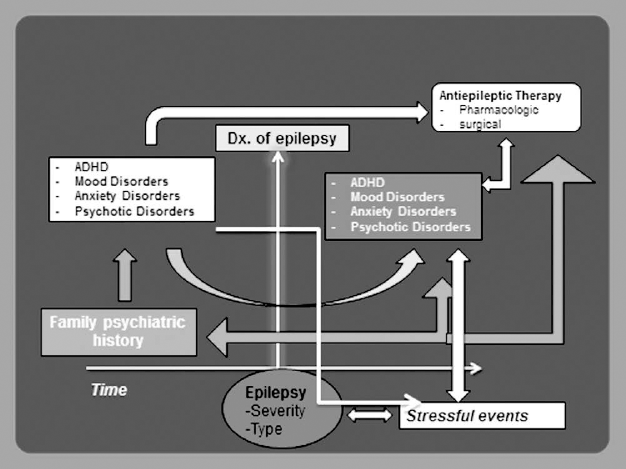
Summary illustration of the course of psychiatric comorbidities over time.
Psychiatric Comorbidities in Epilepsy: Where Does it All Begin?
In a cross-sectional Canadian population-based study, the lifetime prevalence of psychiatric disorders in PWE was estimated to range between 30 and 35 percent (1), with a prevalence of major depressive disorders (MDDs) of 17.4% (95% confidence interval [CI]: 10.0–24.9) compared with 10.7% in controls (95% CI: 10.2–11.2), while the lifetime prevalence of any mood disorder (including MDD, bipolar disorder [BPD], dysthymia, and/or cyclothymia) was found to be 34.2% (95% CI: 25.0–43.3) compared with 19.6% in controls (95% CI: 19.0–20.2). These data have been supported by other population-based studies.
Population-based studies that have investigated the temporal relation between the onset of PC and clinical onset of epilepsy have recognized an increased incidence of psychiatric disorders preceding the first seizure in patients who go on to develop epilepsy compared with controls (2–8). For example, in a population-based study from the United Kingdom, Hesdorffer et al. (5) compared the incidence of mood, anxiety, psychotic disorders, and suicidal behavior in 3,773 subjects who went on to develop epilepsy and 14,025 controls during the 3 years preceding and the 3 years following the onset of epilepsy. Anxiety disorders were identified in 18.5% of subjects who went on to develop epilepsy (vs 13.8% of controls), while depression was found in 17.5% (vs 11.7% of controls). Interestingly enough, the incidence of depressive and anxiety disorders following the onset of epilepsy was 2- to 3-fold higher among PWE than controls. These data confirmed those of three previous population-based studies (2–4). Likewise, in a population-based study conducted in Taiwan, patients with primary schizophreniform disorders had a 6-fold higher risk of developing epilepsy, while PWE were found to have a 7-fold higher risk of developing schizophrenia (6), confirming data from a population-based study done in Sweden (7). Finally, a population-based study in Iceland suggested that children with Attention Deficit Hyperactivity Disorder (ADHD) of the Inattentive type had a 3.5-fold higher risk of developing epilepsy (8). Clearly, these data demonstrate that psychopathology in PWE often precedes the onset of the seizures.
A genetic predisposition is well known in all primary major psychiatric disorders and, in particular, in those that are more prevalent in PWE (mood, anxiety, and ADHD). For example, first-degree relatives of subjects with primary MDD and bipolar disorder have a 2- to 3-fold and an 8- to 9-fold higher lifetime risk of developing these conditions, respectively, with a heritability estimate of 33 to 42 percent for MDD and 65 to 80 percent for bipolar disorder (10). The expression of this heritability has been explained on the basis of multiple genes with variable penetrance. In the case of panic disorders, the lifetime risk in first-degree relatives has been estimated to range between 7.8 and 10.7 percent; while in the case of generalized anxiety disorder (GAD), first-degree relatives had an 8.9 % lifetime risk (11). Likewise, familial aggregation was identified in 19.5% of patients with primary GAD (vs 1.5% of controls). Clearly, identification of psychiatric family history, particularly in first-degree relatives, is of the essence to have a full picture of risk factors.
Impact of a Prior or Current Psychiatric Disorder on the Development of Future PCs
Given the high lifetime prevalence of PCs in PWE (one in three patients), recognition of a lifetime psychiatric history and/or family psychiatric history are of the essence at the time of the initial evaluation of the seizure disorder, as it can help identify those PWE at risk for future PCs including their most serious complications (e.g., completed suicide). In fact, most of the common PCs tend to recur over time. For example, one primary MDE is associated with a 50% risk of a second episode, two MDEs with a 70% risk, and three or more with a >90% risk of recurrence. These observations apply for other types of mood disorders as well as for anxiety disorders. Furthermore, symptoms of primary ADHD persist into adulthood in 50 to 75 percent of patients, although in a modified manner. Thus, when a psychiatric history is endorsed, PWE and their families must be made aware of the increased risk of recurrence of the psychiatric disorder and must be encouraged to report it to their treating physicians. Psychiatric episodes that recur throughout the life of the seizure disorder may be clinically indistinguishable from previous ones, although de novo atypical manifestations of these disorders can develop (12, 13).
In addition, PWE may exhibit common psychiatric phenomena closely related to the seizure disorder including (1) psychiatric symptoms/episodes that occur temporally related to the seizure occurrence, either preceding (pre-ictal) or following (postictal) it, (2) iatrogenic psychiatric symptoms, following the introduction or discontinuation of certain anti-epileptic drugs (AEDs) or following epilepsy surgery. These are reviewed in some detail below.
Postictal Psychiatric Symptoms/Episodes
Postictal psychiatric symptoms/episodes are relatively frequent in patients with treatment-resistant epilepsy but more often than not go unrecognized by clinicians. In one study of 100 consecutive PWE, postictal symptoms of depression were endorsed by 43 patients, postictal symptoms of anxiety by 45, and psychotic symptoms by 7, with a median duration of 24 hours (14). These symptoms were a habitual occurrence as they tended to recur after more than 50% of the seizures that patients experienced in the course of the previous 3 months. Of note, a previous psychiatric history was a risk factor for the development of postictal psychiatric symptoms. In addition, breakthrough symptoms of depression and/or anxiety were reported 1 to 3 days after their seizures in patients whose in-terictal mood and anxiety disorders were in remission on or off psychotropic drugs. Habitual postictal suicidal ideation with a median duration of 24 hours was reported by 13 patients; a prior history of a severe mood disorder and of a psychiatric hospitalization were associated with the occurrence of postictal suicidal ideation. While postictal psychotic symptoms remitted with low doses of antipsychotic drugs, symptoms of depression including suicidal symptoms do not appear to be blocked by antidepressant medication, suggesting different pathogenic mechanisms mediating interictal and postictal symptoms of depression.
Iatrogenic Psychiatric Adverse Events
Several studies have demonstrated the association between a previous and/or family psychiatric history and an increased risk of iatrogenic psychiatric adverse events following the introduction of several AEDs including barbiturates, topiramate, levetiracetam, benzodiazepines, vigabatrin, and zonisamide (15–17). By the same token, discontinuation of AEDs with mood stabilizing (e.g., valproic acid, carbamazepine, oxcarbazepine, lamotrigine), antidepressant (e.g., lamotrigine), and anxiolytic properties (e.g., pregabalin, gabapentin) can result in the development of mood and/or anxiety episodes in PWE with a prior psychiatric disorder that was in remission with any of these AEDs.
Clearly, the occurrence of these iatrogenic adverse events can be anticipated and/or prevented if a lifetime and/or family psychiatric history is elicited at the time of the initial evaluation. Thus, the use of the AEDs with negative psychotropic properties listed above should not be the first choice, and if prescribed, patients and their families must be advised of the increased risk of psychiatric symptoms. Likewise, discontinuation of AEDs with positive psychotropic properties must be conducted with great caution in patients with previous and/or family psychiatric history.
A review of the literature revealed that between 20 and 40 percent of patients who undergo epilepsy surgery are expected to develop a worsening and/or recurrence of a presurgical depressive and/or anxiety disorder during the first 3 to 6 postsurgical months and in 10 to 15 percent, these symptoms may be severe enough to cause suicidal ideation and behavior (18). For example, in a study of 60 PWE undergoing a temporal lobectomy (38 had a resection of mesial structures, and 22 had resection of temporal lateral neocortical structures) (19), a lifetime history of depression was identified in 43% of patients, with no difference between those who had mesial and those who had temporal lateral resections. In the 12 months after surgery, 20 patients (33%) experienced an MDE (occurring in the first 3 postsurgical months in 70% and persisting for at least 6 months in 65% of patients). A preoperative history of depression and poor postoperative family dynamics were predictive of depression after surgery. In a separate study, patients with a preoperative psychiatric history had more than six times the odds of developing a postoperative psychiatric disorder (20). Furthermore, in one multicenter study that included 396 patients, 27 deaths were reported after surgery, 4 of which were attributed to suicide (21). The standardized mortality ratio, compared with suicides in the U.S. population and adjusted for age and sex, was 13.3 (95% CI: 3.6–34.0). Thus, screening for depressive and anxiety disorders at the time of a presurgical evaluation is not sufficient to identify the risk of these patients for postsurgical psychiatric episodes. Identification of a lifetime psychiatric history is of the essence.
Averting Suicidal Attempts
Premature mortality is a well-known phenomenon in PWE. In a recent population study, premature mortality was found to be approximately 11-fold more frequent among PWE than among the general population and unaffected siblings (22), while a lifetime prevalence of psychiatric disorders was 40.7% (compared with 10.3% in controls). Among all deaths, 15.8% were attributed to external causes, which included death by suicide and accidents (in a motor vehicle or through drug poisoning, falls, drowning, assault, and other incidents). Of note, 75% of PWE who died from external causes were found to suffer from PC, mainly depression and drug misuse. Furthermore, in another population-based study of PWE conducted in Denmark, mood disorders were shown to increase the risk of suicide by 32-fold, while anxiety and schizophrenia caused a 12-fold increase (23). In that study, suicides occurred more frequently during the first 6 months after the diagnosis of epilepsy. Thus, an early recognition of a patient's lifetime psychiatric history can help minimize the suicidal risk and premature death from other external causes that are prevalent in PWE.
Impact of a Lifetime Psychiatric History on the Seizure Disorder
A lifetime psychiatric history can have an impact on the course of the seizure disorder at several levels: (1) its response to pharmacologic and surgical treatment, (2) a propensity to seizure worsening with stressors, and (3) its tolerance to AEDs. These points will be reviewed below.
In a retrospective study that included 780 consecutive patients with new-onset epilepsy followed for a median period of 79 months, a psychiatric history preceding the onset of the seizure disorder and, in particular, a history of depression was associated with a greater than 2-fold higher risk of developing treatment-resistant epilepsy (24). In a separate prospective study of 138 consecutive patients with new-onset epilepsy who were started on AEDs, those who endorsed symptoms of depression and anxiety in a screening instrument completed before the start of AEDs were significantly less likely to be seizure free after 12 months of therapy (25). By the same token, a lifetime history of psychiatric disorders has also been associated with a worse postsurgical seizure outcome. For example, in a study of 100 consecutive patients with temporal lobe epilepsy (TLE) who underwent an anterior temporal lobectomy, a lifetime history of depression was identified in 12% of patients who reached complete seizure freedom at 2 years after surgery, in contrast to 79% in patients with persistent disabling seizures (26). These data were confirmed in two studies of 280 and 115 patients with TLE secondary to mesial temporal sclerosis (MTS), respectively (27, 28). These data do not suggest that a lifetime psychiatric history should be considered a reason not to offer a surgical option. However, in PWE and a lifetime psychiatric history, discontinuation of AEDs may be considered with greater caution after a postsurgical seizure-free period; though this question has yet to be investigated in prospective controlled studies.
The Impact of a Lifetime History of PC on the Risk of Stress-Related Worsening of Seizures
In PWE, stress has been found to increase seizure frequency, while animal models of stress have suggested that stressful events facilitate the kindling process (29, 30). For example, in a survey conducted in 89 PWE, 64% had associated the occurrence of stress with an increased frequency of their seizures (31). Yet, while stressful experiences are normal in all humans, pathologic reactions to stressful situations are more likely to occur in patients with a lifetime psychiatric history and/or a family psychiatric history. Haut et al. demonstrated the impact of stress on the occurrence of seizures in a study of 71 PWE in whom one-unit increments of anxiety and stress (on a 10-point scale) were associated with an increased risk of seizure the following day (32). In short, in PWE with a previous history of mood and anxiety disorders, clinicians must investigate the impact of stress on their seizure frequency and recommend stress-reducing strategies to overcome this problem in addition to ensuring that comorbid mood and anxiety disorders are adequately treated..
These data, coupled with the observations that primary psychiatric disorders are associated with an increased risk of developing epilepsy, would suggest that pathogenic mechanisms operant in PCs may enhance the hyperexcitability of the brain. In fact, a review of the neurobiologic pathogenic mechanisms of primary mood and anxiety disorders identified several mechanisms that may in fact yield such hyperexcitability. These include (1) an increase in glutamatergic and a decrease in GABAergic neurotransmission in the brain, (2) a decrease in serotonergic activity, which has been shown to facilitate seizure occurrence in animal models of epilepsy, (3) a hyperactive hypothalamic-pituitary adrenal axis, which has been associated with a decreased serotonergic and increased glutamatergic activity in the brain, structural changes including bilateral hippocampal atrophy as well as atrophy of various frontal lobe structures, and (4) inflammatory disturbances in the brain, which through glutamatergic mechanisms have been identified as pathogenic mechanisms of seizures. This topic is reviewed in great detail elsewhere (33, 34).
Impact of PCs on the Tolerance of AEDs
Psychiatric comorbidities can interfere with the management of seizures as they may have a negative impact on the tolerance of AEDs. Indeed, two studies have demonstrated that patients with MDE endorsed more severe adverse events of AEDs (35, 36). One of these studies also demonstrated that the worse tolerance was also associated with less severe forms of depression such as subsyndromic depressive episodes (36). Furthermore, anxiety disorders were also found to yield a comparably poor tolerance, and this effect was more notable among PWE who experienced comorbid MDE and anxiety disorders (36).
Clearly, the impact of PC on the efficacy and tolerability to AEDs has to be factored in when interpreting data from AED trials in PWE submitted to the FDA for regulatory purposes. Yet, to date, none of these studies controls for the presence of comorbid depressive and anxiety disorders in the assessment of their efficacy and tolerability data.
Concluding Remarks
Psychiatric comorbidities in epilepsy are relatively frequent in PWE and their relation is very complex. While screening for these conditions is a good start to identify PWE who are symptomatic with a PC, it is of the essence that clinicians have a clear picture of the lifetime psychiatric history, as well as major risk factors such as a family psychiatric history. In a busy outpatient practice, neurologists can use data from the screening instruments to investigate the presence of the two most frequent PCs in epilepsy: MDE and GAD. The NDDI-E is used to screen for the former (9), while the Patient's Health Questionnaire, Generalized Anxiety Disorder–7, is used to screen for the latter (37). Total scores >15 and >10 are suggestive of MDE and GAD, respectively. Thus, in symptomatic patients, neurologists should inquire if similar symptoms have occurred in the past, the age of their first occurrence, and estimated frequency of recurrence. To inquire about possible family psychiatric history of these conditions, neurologists can simply ask if any first-degree relative is known to have experienced similar symptoms. Clearly, these questions would add less than 3 minutes to the overall interview. After all, having these clinical data available can mitigate the development of future recurrence of psychiatric disorders, avoid iatrogenic psychiatric episodes, and minimize the risk of poor tolerance to AEDs. Future research will need to determine whether an early remission of psychiatric disorders can reverse the progression of epilepsy, however.