
Abstract

Human Herpesvirus 6 and 7 in Febrile Status Epilepticus: The FEBSTAT Study.
Epstein LG, Shinnar S, Hesdorffer DC, Nordli DR, Hamidullah A, Benn EK, Pellock JM, Frank LM, Lewis DV, Moshe SL, Shinnar RC, Sun S; FEBSTAT study team. Epilepsia 2012;53:1481–1488.
PURPOSE: In a prospective study, Consequences of Prolonged Febrile Seizures in Childhood (FEBSTAT), we determined the frequency of human herpesvirus (HHV)-6 and HHV-7 infection as a cause of febrile status epilepticus (FSE). METHODS: Children ages 1 month to 5 years presenting with FSE were enrolled within 72 h and received a comprehensive assessment including specimens for HHV-6 and HHV-7. The presence of HHV-6A, HHV-6B, or HHV-7 DNA and RNA (amplified across a spliced junction) determined using quantitative polymerase chain reaction (qPCR) at baseline indicated viremia. Antibody titers to HHV-6 and HHV-7 were used in conjunction with the PCR results to distinguish primary infection from reactivated or prior infection. KEY FINDINGS: Of 199 children evaluated, HHV-6 or HHV-7 status could be determined in 169 (84.9%). HHV-6B viremia at baseline was found in 54 children (32.0%), including 38 with primary infection and 16 with reactivated infection. No HHV-6A infections were identified. HHV-7 viremia at baseline was observed in 12 children (7.1%), including eight with primary infection and four with reactivated infection. Two subjects had HHV-6/HHV-7 primary coinfection at baseline. There were no differences in age, characteristics of illness or fever, seizure phenomenology or the proportion of acute EEG or imaging abnormalities in children presenting with FSE with or without HHV infection. SIGNIFICANCE: HHV-6B infection is commonly associated with FSE. HHV-7 infection is less frequently associated with FSE. Together, they account for one third of FSE, a condition associated with an increased risk of both hippocampal injury and subsequent temporal lobe epilepsy.
Acute EEG Findings in Children with Febrile Status Epilepticus: Results of the FEBSTAT Study.
Nordli DR Jr, Moshé SL, Shinnar S, Hesdorffer DC, Sogawa Y, Pellock JM, Lewis DV, Frank LM, Shinnar RC, Sun S; FEBSTAT study team. Neurology 2012;79:2180–2186.
OBJECTIVE: The FEBSTAT (Consequences of Prolonged Febrile Seizures) study is prospectively addressing the relationships among serial EEG, MRI, and clinical follow-up in a cohort of children followed from the time of presentation with febrile status epilepticus (FSE). METHODS: We recruited 199 children with FSE within 72 hours of presentation. Children underwent a detailed history, physical examination, MRI, and EEG within 72 hours. All EEGs were read by 2 teams and then conferenced. Associations with abnormal EEG were determined using logistic regression. Interrater reliability was assessed using the statistic. RESULTS: Of the 199 EEGs, 90 (45.2%) were abnormal with the most common abnormality being focal slowing (n = 47) or attenuation (n = 25); these were maximal over the temporal areas in almost all cases. Epileptiform abnormalities were present in 13 EEGs (6.5%). In adjusted analysis, the odds of focal slowing were significantly increased by focal FSE (odds ratio [OR] = 5.08) and hippocampal T2 signal abnormality (OR = 3.50) and significantly decreased with high peak temperature (OR = 0.18). Focal EEG attenuation was also associated with hippocampal T2 signal abnormality (OR = 3.3). CONCLUSIONS: Focal EEG slowing or attenuation are present in EEGs obtained within 72 hours of FSE in a substantial proportion of children and are highly associated with MRI evidence of acute hippocampal injury. These findings may be a sensitive and readily obtainable marker of acute injury associated with FSE.
Commentary
“The FEBSTAT [Consequences of Prolonged Febrile Seizures in Childhood] study was designed to prospectively examine the association between prolonged febrile seizures and development of HS [hippocampal sclerosis] and associated temporal lobe epilepsy [TLE], one of the most controversial issues in epilepsy” (1). To resolve this issue, children aged 1 month to 6 years presenting with a febrile seizure lasting 30 min or longer, termed febrile status epilepticus (FSE), were enrolled. At baseline, subjects underwent brain magnetic resonance imaging (MRI) study and electroencephalography (EEG) performed within 72 hours, a detailed history, and a neurologic examination. Baseline development and behavior assessment occurred at 1 month, and 1 and 5 years. The subjects are closely monitored for the subsequent occurrence of nonfebrile seizures. Two other groups of children also comprise research cohorts for this study: 1) a “control” group consisting of children with a first febrile seizure (FS) enrolled through a different study protocol at Columbia University who underwent similar baseline and 1-year follow-up examinations and 2) a pilot cohort of FSE from Duke University. In the Columbia control group, 15 of 159 (9.4%) had FSE as their presentation. In the FEBSTAT group, 20% had febrile seizures, and 7% had FSE prior to the FSE episode that resulted in enrollment. The purpose of the Duke Pilot cohort, which consisted of 39 subjects—who appeared to be enrolled about 5 to 10 years prior to the FEBSTAT cohort—is to be hypothesis-generating for the larger FEBSTAT cohort, as findings emerge in this smaller, closely observed group (1).
The relationship between the occurrence of FS and the subsequent development of HS and temporal lobe epilepsy seems so plausible and somehow would be so intellectually satisfying, yet it has not been proven. Perhaps studying these special subjects will prove the connection, some of whose hippocampi harbor a secret mechanism for epileptogenesis, eventually to be revealed.
In the meantime, the reported risks for and incidence of unprovoked seizures and epilepsy after febrile seizures has been stable across decades. As reported by Annegers et al. in 1987 from a Rochester, MN, cohort of 687 children who had a febrile convulsion, the rate of unprovoked seizures was after febrile convulsions was 7% by age 25, and febrile seizures imparted a 5-fold risk of unprovoked seizures later in life (2). In a large population-based study of the relationship of febrile seizures to subsequent epilepsy from Denmark, published in 2007 (3), the overall cumulative incidence of epilepsy after febrile seizures was 6.9% (95% confidence interval: 6.5, 7.3) at 23 years of follow-up. The rate ratio for epilepsy after febrile seizures was 5.43 (95% confidence interval: 5.19, 5.69) and was much higher in the three years following the first febrile seizure. In a more recent 2012 study by Neligan et al. using a large community-based prospective database of FS patients followed for a mean of 22 years (SD 6 years), 6% developed epilepsy (4). The standardized incidence ratio (SIR) of developing epilepsy in the cohort over the entire follow-up period was almost 10 times that of the general population (SIR 9.7, 95% CI 5.7–16.4) but decreased over time. For example, in the 15- to 19-year age group, the SIR did not reach significance.
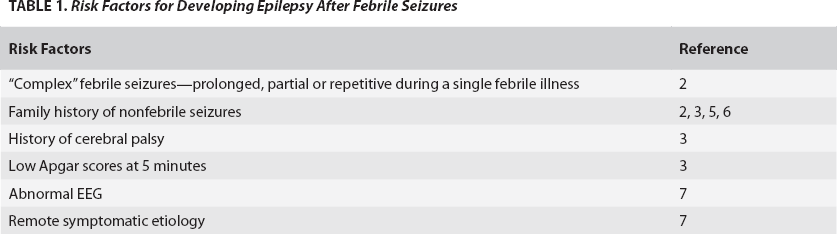
Annegers et al. (2) reported that the development of partial versus generalized epilepsy after febrile seizures is associated with clinical and historical features which actually make intuitive sense (see Table 1). “Complex” febrile seizures—that is, focal, prolonged, or repetitive seizures—within the same febrile illness were associated with the subsequent development of partial epilepsy, while a family history of epilepsy and the number of febrile convulsions were associated with the subsequent development of generalized epilepsy. This clinical picture is consistent with potential localized, mesial temporal brain injury leading to focal epilepsy, and an underlying, perhaps genetically imparted tendency to febrile seizures associating with the later emergence of generalized epilepsy. However, this ultimate chicken-and-egg conundrum associated with febrile seizures as they relate to epilepsy is sufficient to question one's intuition. Indeed, subsequent investigators have not found that the clinical features of febrile seizures are associated with specific forms of epilepsy (5, 6), while a family history of epilepsy remains a strong risk factor across most studies, assuming that families with the autosomal dominant GEFS+ mutations are excluded. See Table 1 for brief list of risk factors.
Risk Factors for Developing Epilepsy After Febrile Seizures
Thus far, in the three FEBSTAT research cohorts, 22 of 199 (11%) of the FEBSTAT subjects have developed epilepsy, 7 of 23 (30%) of the Duke cohort have developed epilepsy, and after 42 months of follow-up in the Columbia cohort of FS, 9 of 157 (5.7%) have developed epilepsy (1). These findings are consistent with the preliminary observation that FSE is more commonly associated with subsequent epilepsy than FS and predict that many more FEBSTAT subjects will develop epilepsy over time.
This brings us to the most interesting finding among the five papers (1, 8–11) reported from the FEBSTAT data: the high rate of new HHV-6B infection in the FEBSTAT cohort of 24% (40/169) (8). This finding, supported by the same virus being overrepresented in TLE mesial temporal surgical specimens (12), may indicate an infectious cause of epilepsy and, therefore, lead to avenues of treatment and even prevention. By way of providing a historical control, the authors cite a HHV-6 infections rate in children with an acute febrile illness of 9.7%, much lower than the proportion found in FEBSTAT subjects (13). The evidence for HHV-6B as a causative agent for later epilepsy will be shown if the FEBSTAT subjects who later developed epilepsy also had positive findings for a new infection, compared to those subjects who did not develop epilepsy. However, children with febrile seizures may also have seropositivity for other viral infections, including adenovirus, influenza, rotavirus, RSV and parainfluenza infections (14). The presence of these viruses were not evaluated in the FEBSTAT study or in the pathologic study from which FEBSTAT is based upon.
The FEBSTAT group is an enriched group for the risk of developing epilepsy. Any factor associated with this transition may be generalizable to other scenarios in which the reason for epilepsy is unknown. But the chicken-and-egg problem remains: Perhaps the new HHV-6B infection requires a brain substrate that is already seizure-prone in order to cause epilepsy later in life, such as when there is a genetic predisposition evidenced by a family history. However, if the infection is overrepresented in groups less vulnerable to developing epilepsy—such as FS only who later develop epilepsy—this would lend more weight to HHV-6B as a causative agent. This is loosely analogous to finding a disease-associated gene in families and then proving that it is disease-causing when there is no family history. Furthermore, the specificity of HHV-6B versus other viral illnesses as a cause of febrile seizures and subsequent epilepsy requires further study.
The presence of HHV-6B in the Columbia FS control group is not available for comparison in this study; serology was not performed for this group. Further, the investigators may have to limit their analysis for this portion of their research to those who had FSE as the initial presentation of a seizure in order to capture the primary infection rate; this is the great majority of their subjects, in any case. The EEG findings (10), while interesting, are not nearly as provocative as the infectious findings; they do not readily lead to any clear ideas for intervention or prevention. We look forward to learning much more about epileptogenesis as this remarkable group is followed.