
Abstract
Stenosis and thrombosis are common causes of prosthetic vascular access (pVA) failure. The role of arteriovenous fistula (AVF) surveillance is widely debated. The aim of this paper is to present a new real-time application designed for AVF surveillance called SPIDER. Surgical staff and hemodialysis nurses are responsible for data entry. SPIDER automatically analyses data and generates alerts in case of abnormal trends. Surgical evaluation and duplex Doppler ultrasonography are then immediately performed to confirm presence of stenosis or other possible pVA defects. Surgery can be performed if required. A preliminary analysis of results will be completed at 12 months after the program begins and subsequently after 24 months. Primary assisted patency will be compared with historical using multivariate analysis. Expected results are an improvement in primary assisted pVA patency and reduction of hospitalizations. Simultaneous management of a high number of patients can become difficult due to the large amount of data required for surveillance. We want to demonstrate whether a real-time automated system could help to prevent thrombosis and graft loss.
Introduction
Arteriovenous fistula (AVF) maintenance still remains the most important challenge for nephrologists and surgeons. Outflow stenoses continue to be the most common cause of prosthetic vascular access (pVA) thrombosis and abandonment. Nevertheless, the role of AVF surveillance is still widely debated. In particular, the literature does not clarified whether surveillance associated with preemptive surgery can prolong AVF survival (1). However, the Society for Vascular Surgery (SVS) clinical practice guidelines suggest a careful instrumental monitoring to prevent thrombosis (2). The aim of this paper is to present our project for real-time computerized surveillance and to compare it with ordinary clinical monitoring.
Definitions
AVF results and complications have been considered and reported according to SVS recommended standards (3). In agreement with SVS standards, an AVF is defined as being affected by thrombosis if it is “not patent and not functional.”
Study objectives
Objective of the present study is to assess the efficacy of a computerized program for pVA surveillance and to evaluate if an early management of pVA defects can prevent thrombosis or graft loss.
Primary end point
The end point of the present study will be an evaluation of whether collection of data on pVA performance and real-time analysis can identify early graft damage and prevent failure. Effectiveness of the program will be estimated in terms of primary assisted graft patency and increased graft survival.
Secondary end point
The secondary end point will be an assessment of more sensitive parameters, or a summation of these, predictive of pVA malfunctioning, to reduce the amount of data collected and analyzed.
Control group
Control group will be represented by the cohort of patients who underwent implantation of pVA before the SPIDER program started (4).
Expected data
The expected result will be the reduction of pVA thrombosis by an estimated 58.7%, with a consequent increase in primary patency to 92% at 12 months.
Patient recruitment
All patients who have already undergone a pVA implantation between October 2011 and December 2014 will be included in the database. In addition, all patients who will undergo a pVA implantation after the SPIDER project begins will be added to the present study. Indications for pVA have already been reported in a previous paper (4). All patients will be informed about the aims of the project, and will have the option of being excluded at any time. Study withdrawals will not affect the quality of care received. All patients will be required to sign an authorization for data processing.
Study plan
Discussion
For the past 4 decades, neointimal graft hyperplasia has been a well-known entity (5), and it is generally considered the leading cause of pVA stenosis (6), mainly observed at the prosthetic–venous anastomosis (in 58% of cases) (7). Finally, it is well documented that pVAs are more prone to thrombosis than autogenous vascular access (8).
Although, many studies have been proposed to demonstrate effectiveness of AVF surveillance, results are still controversial. In fact, data quality is often affected by methodological limitations and inconsistencies. Even the use of percutaneous transluminal angioplasty (PTA) for the treatment of critical stenosis continues to be controversial. Furthermore, some authors suggest that endothelial damage produced by PTA can accelerate processes of restenosis and thrombosis (9) without taking into account the introduction of new devices, such as a drug eluting balloon, that promise significant reduction in terms of restenosis (10). Nevertheless, a large meta-analysis concluded that access surveillance might reduce thrombosis and prolong access survival more than simple clinical monitoring (11). In addition, a recent review emphasized that failure of surveillance programs generally depends on employment of partial instrumental data and on a lack of compliance to international guidelines. In addition, PTA success is generally estimated from a morphological point of view omitting hemodynamic assessment (12). Finally, some authors underline how many clinical trials are affected by incorrect patient recruitment, underestimation of hemodynamic values and overtreatment of asymptomatic patients (13). The National Kidney Foundation (NKF) Kidney Disease Outcome Quality Initiative (KDOQI) Clinical Practice Guidelines (12) declare that surveillance strongly depends on narrow clinical monitoring performed by skilled personnel, with 70% positive predictive value and 90% specificity (8, 14). However, evidence based on everyday experience suggests that careful instrumental monitoring is required to prevent thrombosis most of the time. NKF-KDOQI defines 5 main tools available for arteriovenous (AV) access surveillance: (i) physical examination, (ii) access blood flow measurements, (iii) static venous dialysis pressure, (iv) prepump arterial dialysis pressure and (v) duplex ultrasound (DU) imaging. NKF-KDOQI and SVS guidelines additionally note that decreases in delivered dose of dialysis (Kt/V) have a 69% positive predictive value for significant stenosis (2, 14).
Database architecture
First of all, SPIDER (Fig. 1A) is a database for collection and automated real-time analysis of clinical and instrumental data. Patients involved in the analysis are affected by chronic kidney disease (CKD) stage 5d that perform regularly haemodialysis through a pVA. In our purpose SPIDER would be a real-time automated resource for pVA surveillance. Surgical staff and hemodialysis nurses are responsible for data entry in a structured query language (SQL) database throughout online forms. The application was developed with extensible HyperText Markup Language (XHTML, W3C/IETF standard) and Java™ by Mavilab Web Agency (Mavilab, Milan, Italy). Database and program run on a UNIX® server. Access to SPIDER from haemodialysis centres and data entry will be possible through tablet computers equipped with third generation mobile telecommunication technology. (Fig. 2).

A) The SPIDER logo representing a stylized arteriovenous graft loop that becomes an imaginary lemniscate, symbol of prolonged prosthetic vascular access life. B) Example of nurse hemodialysis data entry form. It supplies useful information about graft type, configuration and management.

Nurse with tablet: a dialysis nurse evaluating a complex vascular access before cannulation using a tablet computer connected to the SPIDER system via the Web.
Data entry
The access to SPIDER is allowed through 2 distinct user profiles: physician and nurse. Physicians can evaluate patient's medical history, intervention descriptions, clinical and radiological follow-up. Nurses can visualize the main surgical informations with detailed notes and summaries of guidelines for the management, maintenance and cannulation of pVAs. Every 2 weeks, nurses will be asked to enter instrumental data: blood flow rate, systolic venous dialysis pressure, systemic systolic blood pressure, pre-pump arterial dialysis pressure and delivered dose of dialysis (Kt/V) (Fig. 3).
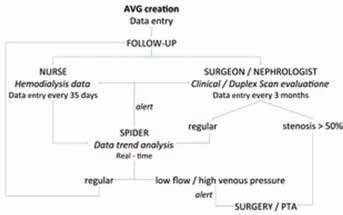
Flow chart of management of complex vascular access through SPIDER. AVG = arteriovenous graft; PTA = percutaneous transluminal angioplasty.
Data analysis and alert messages
Failure in entering required data automatically generates an alert sent to the tablet in the dialysis center as a reminder, and to the physician in charge of the project. Abnormalities in dialysis session, difficulties in cannulation and hemostasis reported by nurses will generate an alert sent to the project manager. Data trends will be analyzed by SPIDER in real time. The program will automatically generate an alert when oddities are detected. The alert will be followed by an immediate clinical and ultrasound analysis performed by a surgeon.
Patient evaluation and stenosis management
Within 48 hours of an alert, the patient will be evaluated with duplex Doppler ultrasonography. In case of stenosis, indication for surgery or endovascular management will be: stenosis that reduce more than 50% the luminal diameter, doubling in peak systolic velocity (PSV) between the two sides of the stenosis, decrease of flow volume ≥25% or <600 ml/min (13).
Period of study
The first training course on SPIDER addressed to nursing staff in our dialysis center will take place on 9 December 2014. On 7 January 2015, SPIDER will formally start to operate. A 3-month break-in test period in a single dialysis center will ensure the resolution of software problems, improvement of data-entry forms, best settings for the virtual server and staff training. Subsequently, on April 2015, the service will be extended to another 6 dialysis centers. The first 6 months will be used to better adjust the cutoffs for sending alerts. Preliminary analysis of results will be performed at 12 months after program start and then at 24 months.
Conclusion
Surveillance on a pVA requires analysis of multiple clinical and instrumental parameters. For that reason, the simultaneous management of a high number of patients can be challenging. The introduction of a real-time automated system can help physicians and nurse to better survey patients, detecting early pVA stenosis and malfunction before thromboses occur. It is our aim to achieve early complication management that will enable us to ensure increased graft survival.
Author contributions
Footnotes
Financial support: The study was funded by Fo.co.VA grant 2014, Fondazione Comunitaria del Varesotto ONLUS, 6, Via Felice Orrigoni - 21100 Varese.
None.