
Abstract
Background
Post-operative upper extremity exercise is recommended to patients with arteriovenous fistulas. It is postulated that increased blood flow to vessels improves maturation and patency rates. Recent studies favour pre-operative exercise therapy to improve the outcomes of arteriovenous fistula creation.
Objectives
To investigate if pre-operative exercise therapy increases vessel diameter and maturation in patients undergoing distal arteriovenous fistula creation.
Methods
34 patients planned for radiocephalic arteriovenous fistula creation were recruited at a tertiary university hospital Vascular Surgery Unit. Patients underwent a 6-week period of self-directed daily upper extremity exercises before surgery. Patients were reviewed up to 6 months post-surgery. The primary outcome investigated was change in venous and arterial diameters following exercise intervention. The secondary outcome investigated was the primary failure rate of the newly created arteriovenous fistulas.
Results
After exercise therapy, mean hand grip strength increased from 20.3 ± 6.62 kg to 21.9 ± 7.16 kg (p=.01). There was a statistically significant increase in basilic vein diameter amongst those who demonstrated strict compliance to at least 42 days of pre-operative exercise therapy by 0.51 mm from 3.23 ± 1.09 mm to 3.74 ± 1.31 mm (p=.03). Primary failure rate of newly created radiocephalic arteriovenous fistulas was 25% (7 of 28), comparable to our previous series of 436 distal arteriovenous fistulas created which had a failure rate of 26%.
Conclusions
There was a trend of increase in vein diameters after pre-operative exercise therapy. Although not statistically significant, patients with successful arteriovenous fistula creation had longer mean completion of exercise days.
Introduction
Autogenous arteriovenous fistulae (AVF) are preferred as the mode of dialysis access in patients with end-stage renal failure due to reduced infections and greater reliability. For patients reliant on haemodialysis, the National Kidney Foundation Kidney Dialysis Outcomes Quality Initiative Clinical Practice Guidelines (NKF KDOQI) recommends a distal to proximal approach to AVF creation, preferentially using superficial veins of the forearm first to preserve proximal vessels for future access. 1 As such, distal forearm access like radiocephalic AVF are often created first.
Primary failure of AVF occurs in 30% to 70% of patients. Small diameter blood vessels and low blood flow are known reasons for non-maturation, besides other non-modifiable factors like age and gender. 2 Smaller vein diameters have also been shown to correlate with ethnic differences resulting in lower rates of AVF maturation. 3
Regular post-operative hand-arm exercises are postulated to increase blood flow to the involved extremity, improving the prospects of successful AVF creation. KDOQI states that arm exercises after AVF creation should be positively considered despite inadequate evidence as it is low cost, non-invasive and causes little to no harm. 1
There is however limited data on pre-operative hand arm exercises and their effect on vessel diameters and AVF maturation in chronic kidney disease patients. We look forward to a randomised control trial (PINCH) which is currently in progress.4–6
Our study investigates the effect of pre-operative exercises on patients undergoing AVF creation, measuring its effect on blood vessel diameters and AVF maturation. It will also explore if pre-operative exercises can improve AVF maturation rates for patients with inadequate blood vessel diameter size who would have previously been ineligible for distal AVF creation.
Methods
Hospital and Patients
This was a single centre prospective pilot study from May 2020 to July 2021 at a Vascular Surgery Unit in a 1500 bed tertiary university hospital. All outpatients who were eligible to undergo radiocephalicAVF creation were screened.
Inclusion and exclusion criteria
Patients planned for radio-cephalic AVF creation with wrist cephalic vein and radial artery diameters of at least 1.5 mm were considered eligible. Our usual criteria includes vessel diameter of at least 2 mm but an expanded criteria with a smaller diameter was used for this study. This is because patients with small vessel diameters had the most to gain from pre-operative exercise therapy should vessel size increase. Patients who were unable to comply with prescribed exercises or had another AVF on the ipsilateral upper limb were excluded. Elderly patients more than 80 years of age were also excluded due to the higher risk of primary failure. 7
34 patients were recruited and underwent a 6-week period of self-directed daily forearm and hand exercises until the date of surgery. Five patients dropped out from the study. A total of 29 patients completed the prescribed duration of pre-operative exercises and underwent radiocephalic AVF creation as planned.
Intervention
Subjects were taught forearm and handgrip exercises by a study coordinator and given an exercise pamphlet for reference (Figure 1). All exercises were performed seated, with the forearm and handgrip exercises performed with the elbows flexed at 90°. Subjects underwent at least 6 weeks of self-directed daily forearm and hand exercises using a red TheraBand® with a resistance level of 3.7–5.5 lbs. (Hygienic Corporation, Akron, Ohio, United States) and hand grip strengthener (Domyos, Shanghai, China). The exercises had been modified from a previous publication by Fontsere et al who showed that 1 month of post-operative exercises appeared to increase 1-month clinical maturation for distal accesses.
8
Exercises were performed until surgery and its effect was quantified using pre- and post-intervention hand grip strengths by use of a digital hand grip strength dynamometer. Three measurements of hand grip strength were taken for each participant with an adequate rest period between to minimize fatigue. The mean value for the measurements was calculated. Adherence was assessed with exercise logs and weekly phone calls by the study coordinator. While a 6-week exercise regimen was recommended, subjects had varying extents of adherence, and some performed exercise beyond the recommended duration of 6-weeks. Forearm and hand exercises.
All surgeries were performed by a consultant grade vascular surgeon or a vascular surgery trainee with a consultant in attendance with the anastomosis performed in end to side fashion. The choice of local anesthesia or regional anesthesia was based on surgeon preference.
Pre- and post-intervention cephalic vein diameter, radial artery diameter and brachial artery diameter were measured via duplex ultrasound by vascular sonographers according to Society of Vascular Ultrasound guidelines, using Philips iU22 ultrasound machines (California, USA). Measurements were performed with an upper limb tourniquet close to the axilla with the patient supine. The location of vessel measurement was standardized on both occasions and across all participants at predetermined anatomic locations. Pre-and post-intervention hand grip strength were measured using a digital hand dynamometer (Camry, United States
9
) on the hand for which radioephalic AVF operation was planned. (Figure 2) Digital hand dynamometer grip strength meter.
Patients were reviewed at 6 weeks, 3 months and 6 months following surgery.
The primary outcome was the change in cephalic vein, basilic vein, radial artery and brachial artery diameters following exercise intervention. The secondary outcome investigated was the primary failure rate at 6-months. The patency of the newly created AVF in the period of follow up was verified with electronic clinical documentation.
In our study, we defined primary failure when an AVF was not successfully used as access for hemodialysis, despite all intervention. 10
Statistical analysis
The sample size was calculated to be 20, using a power of .8 and α of .05, given the known mean cephalic vein diameter of 2.3 mm for radiocephalic AVF creation with an expected increase in .5 mm from previously studies.11,12
Based on our institution’s retrospective series of 436 radiocephalic AVF, we planned for a 25% recruitment rate over 12 months. There were 87 distal AVF creations over 12 months in our institution. 12 To account for unanticipated dropouts of up to 30% from unexpected cancellation of surgeries, a sample size of 30 was planned for recruitment, up to a maximum of 40 patients.
All continuous variables are expressed as mean ± standard deviation. Paired two sample for means t-test was performed to evaluate the change in vessel diameters pre-and post-exercise therapy. A p-value of <.05 was considered statistically significant. Effect size was calculated with Cohen’s d. GraphPad Prism version 8 (San Diego, CA, USA) software was used for statistical analysis.
Results
Study population characteristics.

ESRF: end stage renal failure; arteriovenous fistula: arteriovenous fistula; LA: local anaesthesia; RA: regional anaesthesia; SD: standard deviation.
Of the 29 patients who underwent AVF creation, 21 (72%) were male. The mean age of the patients was 61.2 ± 9.52 years. 25 (86%) had hypertension, 19 (66%) had diabetes mellitus. The most common etiology of end-stage renal failure in these patients was diabetes mellitus (62%), followed by hypertension (24%) and glomerulonephritis (14%). Four (14%) were active smokers, 8 (28%) were ex-smokers while 17 (58%) had never smoked before. Of the 29 newly created radiocephalic AVF, 4 (14%) were created on the right forearm while 25 (86%) were created on the left, 2 (7%) on the dominant forearm and 27 (93%) on the non-dominant forearm.
14 (48%) of the 29 patients who underwent the 6-week period of home-based pre-operative demonstrated adherence to self-directed pre-operative exercises for the intended duration of at least 42 days, while 21 (72%) demonstrated adherence to self-directed pre-operative exercises for at least 28 days. On average, the mean duration of engagement in pre-operative exercise therapy was 45 days while the mean duration of complete adherence to pre-operative exercise therapy regime was 39 days.
Hand grip strength before and after pre-operative exercise therapy.

*p < .05.
Primary outcomes
Cephalic vein, basilic vein diameters before and after exercise therapy.
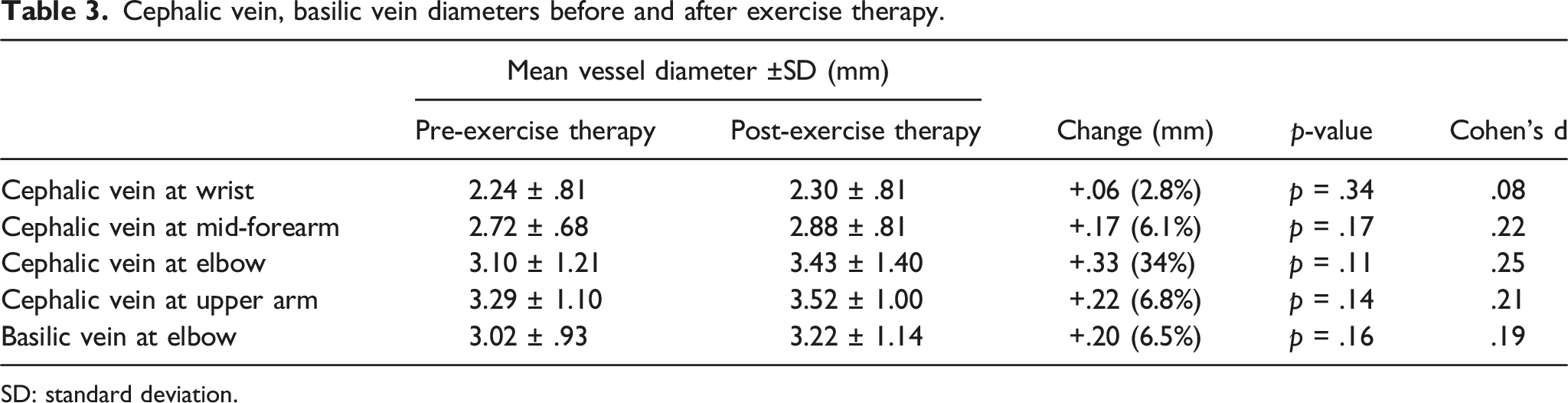
SD: standard deviation.
On subset analysis of the 14 patients who demonstrated adherence to the prescribed exercises for at least 42 days, we found a statistically significant increase in basilic vein diameter by .51 mm (p=.03) (Table 4). There was a non-statistically significant trend of increased cephalic vein and radial artery diameters.
Secondary outcomes
Of the 28 patients who underwent radiocephalic AVF creation and underwent the 6-month period of post-operative study follow up, 7 (25%) experienced primary failure. 21 patients (75%) achieved two needle cannulation and 7 (33%) of these 21 patients required fistuloplasty to aid maturation. The one patient who passed on after AVF creation during the period of study follow-up is not included in the analysis of maturation outcomes.
Even though there was a statistically significant increase in hand grip strength following self-directed exercises, subgroup analysis showed that successful cannulation of AVF did not correlate with increase in grip strength.
The 21 patients who eventually underwent successful 2-needle cannulation of their radiocephalic AVF were noted to have had higher mean duration of compliance to the prescribed pre-operative exercise therapy regimen than the seven patients who experienced primary failure of their radiocephalic arteriovenous fistula (40.9 ± 27.6 days vs 31.6 ± 20.9 days). This, however, was not statistically significant (p=.212).
Discussion
Primary failure of AVF and access dysfunction remain major obstacles to access maturation in end-stage renal failure patients on haemodialysis. Studies have shown that small vessel diameter is a risk factor for early AVF failure. 12 Asian patients have been shown to be more likely to have smaller radial artery diameters than in the Western population, and a recent review of radiocephalic AVF created in Singapore patients showed that larger radial artery diameters were significantly associated with a higher rate of AVF patency.12,13
Exercise upregulates endothelial nitric oxide bioactivity and improves endothelium-dependent vasodilation in both large and small vessels. 14 Over time, these result in enlargement of blood vessels as an adaptive response to mitigate the increases in transmural pressure and wall stress. 15 Cross-sectional studies have shown that young adults who perform regular strenuous endurance exercises have larger arterial diameters than untrained healthy controls. 16
Our study adds to the body of pilot studies in Asia examining the role of pre-operative exercise therapy in patients undergoing distal AVF creation by investigate if the vasodilatory effects of exercise can be utilized as an adjunct to improve vessel size and outcomes post-AVF creation.
Cephalic vein, basilic vein, radial and brachial artery diameters of subjects who demonstrated adherence of ≥42 days of pre-operative exercise therapy.

SD: standard deviation.
Studies investigating changes in vessel characteristics after upper limb exercises.

CKD: chronic kidney disease; AVF: arteriovenous fistula.
Kumar et al investigated the changes in vessel flow velocities in 23 chronic kidney disease patients after engagement in upper arm exercises by squeezing a tennis ball for at least 30 min per day for 28 days at a rate of 20 squeezes per minute over a 4-week period. The effect of the performed exercises on grip strength was also quantified by a hand dynamometer. The study showed marginal but statistically significant increases in brachial artery mean velocity (3 cm/s) and peak systolic velocity (8 cm/s) and increases in forearm vessel diameter. 17
Uy et al. studied the effect of daily handgrip exercises in patients who performed 10 sets of 20 isometric handgrip exercise repetitions per minute. These handgrip exercises resulted in statistically significant increases in cephalic vein diameters after 4 weeks in both dominant and non-dominant arms with mean distal and proximal cephalic vein diameter increments from 1.66 to 2.13 mm and from 2.22 to 2.81 mm respectively. 11
Rus et al. first studied the effects of exercise on forearm arteries and veins of patients on haemodialysis due to end stage renal failure. 5 14 patients undergoing haemodialysis via a native AVF underwent handgrip training on relevant arm for 8 weeks by squeezing a rubber ring 20 times per minute for 30 min each day. The study showed that there was a statistically significant increase in handgrip strength, radial artery diameter and maximal vein diameter. The radial artery diameters remained unchanged for the first 4 weeks but were found to be significantly increased (p=.025) after 8 weeks of training, whilst brachial artery diameter and mean blood flow remained unchanged. In addition, average vein diameters prior to placement of a tourniquet remained unchanged for the first 4 weeks but were significantly increased after 8 weeks of training (p=.015). Average vein diameters following placement of a tourniquet was already significantly higher after 4 weeks (p=.007) and even higher after 9 weeks of training (p ≤ .001). The authors concluded that regular handgrip training increases the diameter of forearm vessels and improves endothelium-dependent vasodilatation and may be beneficial in chronic renal failure patients before AVF creation. 18
A recent randomised trial of 34 patients showed that mean cephalic vein diameter increased significantly from 1.77 to 1.97 mm to 2.15 and 2.43 mm without and with a tourniquet respectively after an 8-week duration of handgrip exercises using a squeeze ball. This study however showed that the increment in the venous diameter was not proportionate to the duration of exercise and that marked changes were noted only at the first 4 weeks of handgrip exercise (mean changes .31 ± .04 mm) and there was only minimal increment observed for the subsequent 4 weeks (.08 ± .03 mm). 19
The PINCH trial is a Dutch multicentre, single blinded, randomised controlled trial which started recruitment in 2017. 6 Patients similarly underwent at least 6 weeks of preoperative forearm exercises using hand grip trainers for 30 min per day in three sessions of 10 min and 20 squeezes per minute. Patients underwent once-weekly group session with a physiotherapist to monitor training. The results have not been published and are awaited.
Our study found that there was a statistically significant increase in basilic vein diameter only in subjects who were fully compliant to the prescribed 6-week pre-operative exercise therapy regimen. There was also a trend of increment in cephalic and basilic vein diameters regardless of adherence, albeit a non-statistically significant one. An analysis of Cohen’s d also showed that there was a near-medium effect size for the increments in cephalic vein diameter at the mid-forearm, elbow, upper arm and basilic vein diameter at the elbow (Cohen’s d = .39 to .46) amongst these subjects (see Table 4). These findings are in agreement with existing studies which found that vasodilatation and vessel diameters were significantly increased in patients with end-stage renal failure after four to 8 weeks of handgrip strength training.5,19 The statistical significance of basilic vein diameter increase in adherent subjects implies that adherence is an important factor in a pre-operative exercise regime.
The lack of strict adherence to the prescribed exercise therapy regime could be attributed to difficulty in enforcing daily exercises remotely and is a possible confounder towards the results of our study. Despite this, there was still a trend of increased cephalic and basilic vein diameters despite suboptimal compliance to the exercise regime. 72% had demonstrated adherence to self-directed pre-operative exercises for at least 28 days, which may be the point where marked changes are noted in venous diameters. 19 There is room for future studies to evaluate if better compliance to our prescribed pre-operative exercise therapy regime can effect further increment in vessel diameter sizes.
One of our patients completed 101 continuous days of pre-operative exercises. This patient had a significant increase in diameters of the wrist cephalic vein from 1.6 mm to 2.7 mm, mid forearm cephalic vein from 3.2 mm to 4.5 mm, elbow basilic vein from 4.0 mm to 6.7 mm. Radial and brachial artery diameters had also increased from 2.2 mm to 2.5 mm and 4.5 mm to 4.8 mm respectively. Although this participant constitutes an outlier data point within our study, it may be worth performing studies with varying upper limb exercise regimes and for longer periods of time to explore other exercise regimes which may increase vessel diameter sizes more effectively. An excessive duration of intervention should not affect the timely creation of AVF however, given the benefits of obtaining functional native vascular access at dialysis initiation instead of relying on temporizing measures like central vein catheter insertions which may complicate subsequent efforts with AVF creation with central venous disease. 20
Our study population had an expanded inclusion criterion, recruiting patients with vessel diameters of at least 1.5 mm to improve eligibility for surgery. Our institution’s previous study of 436 newly created radiocephalic AVF included patients with a vessel sizes of at least 2 mm and showed a primary failure rate of 26%, comparable to that of international norms with minimum vessel sizes of 2.5 or 3.0 mm. 12 The average radial artery diameter was 2.3 mm amongst males and 1.9 mm amongst females (p=.001). With an even further expanded criteria including vessel sizes of at least 1.5 mm, the primary failure rate in our current study was 25% (7 of 28), not inferior to that of our previous series.
Our study also found that patients with radiocephalic AVF cannulation success had longer mean durations of compliance to exercise therapy. Although this finding was not statistically significant, we postulate that a longer duration of compliance to pre-operative exercise therapy would significantly benefit AVF maturation in a study with a larger sample size.
Limitations
Inter-assessment variability and environmental factors can affect cephalic vein diameter measurements. This effect was minimized by performing ultrasound investigations in a room with a preset temperature and by measuring the diameters from pre-set anatomical landmarks. All ultrasound images were also uploaded, to be allowed to be reviewed by the study team in case of significance discrepancies. Lastly, surgeons were allowed to choose between local anesthesia and regional anesthesia. This might also have been a confounding factor, although it is generally accepted that both methods of anesthesia are comparable in AVF creation with respect to the resulting primary failure rates. 21
Conclusion
In agreement with pre-existing literature, our pilot study shows that there is a trend towards increased venous diameters after exercise therapy, reaching statistical significance in subjects adherent to the prescribed exercise regime. While not statistically significant, patients with AVF maturation and cannulation success also had a longer mean completion of exercise days. Further studies can explore the inclusion of control groups, and trial more intensive or longer durations of exercise as the prescribed intervention.
Footnotes
Acknowledgements
We thank the vascular sonographers at the Tan Tock Seng Hospital Vascular Diagnostic Laboratory for their assistance in obtaining vascular measurements essential towards the analysis in our study. We also thank the Tan Tock Seng Hospital Pitch for Fund program for their kind funding.
Author contributions
Study conception: EY, LZJ Data collection: SL Data analysis: EY, SL, LZJ, CWO Manuscript preparation: CWO, EY, LZJ Critical review and revision, final approval: All authors Accountability for all aspects of the work: All authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by funding by the Tan Tock Seng Hospital Pitch for Fund Program (PFFP20-06) as an investigator-initiated study.
Ethical approval
The National Healthcare Group, Domain Specific Review Board (DSRB) reviewed and approved this study protocol (DSRB Ref: 2019/00,831).
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.