
Abstract
Background
The mannose receptor is an immune adhesion molecule mainly expressed on the surface of antigen-presenting cells such as nonmature dendritic cells and macrophages. This study aimed to investigate mannose receptor expression and its predictive role in papillary gastric cancer patients.
Methods
The expression of the mannose receptor was measured in 120 samples of gastric cancer tissues and corresponding paracarcinoma tissues, by immunohistochemical and quantitative real-time PCR analysis. The relationships between mannose receptor expression and clinicopathological features of gastric cancer patients were analyzed.
Results
The expression rate of the mannose receptor in gastric cancer cells was 45.8% (54/120), significantly higher than that in the paracarcinoma tissue (20.0%, 36/120) (χ2 = 6.286, p = 0.012). High expression of the mannose receptor was closely related to tumor size, T stage, N stage and Union for International Cancer Control (UICC) stage of gastric cancer (p<0.05). A Kaplan-Meier survival model indicated that the survival of patients in the high-expression mannose receptor group was significantly shorter than in the low-expression mannose receptor group (p<0.05). Cox regression analysis showed that high mannose receptor expression was an independent predictor for the prognosis of patients with gastric cancer.
Conclusions
High mannose receptor expression indicates poor prognosis for gastric cancer patients. The mannose receptor may be an important molecular marker for gastric cancer prognosis.
Introduction
In 2012, there were 951,000 new cases of gastric cancer and 723,000 deaths due to gastric cancer worldwide (1). In the past decade, the global morbidity of gastric cancer has decreased, but the morbidity in Asia remains very high (2, 3). In China, gastric cancer commonly presents as a malignant tumor, with 400,000 new cases and 300,000 deaths per year (4, 5). Because early metastasis is one of the main causes of death in gastric cancer patients, exploring the mechanism of metastasis in gastric cancer is important for seeking potential therapeutic targets.
Gastric cancer invasion and metastasis are complex processes that involved multiple genes, proteins and cytokines, and the detailed molecular mechanism of gastric cancer metastasis remains unclear (6-8). The mannose receptor is an immune adhesion molecule mainly expressed on the surface of professional antigen-presenting cells, such as nonmature dendritic cells and macrophages (9). The mannose receptor regulates homeostasis, mediates innate and acquired immune responses, and combines these immune responses together by endocytosis (10, 11). The mannose receptor shows abnormal expression in pancreatic, breast and colorectal cancer (12-14). However, the expression patterns of the mannose receptor in gastric cancer are unknown. In this study, we detected the expression of the mannose receptor in gastric cancer tissue and explored the relationship with the occurrence, development and malignancy of gastric cancer.
Materials and Methods
Patients and Samples
Samples of the cancer tissue and corresponding paracarcinoma tissue were collected from 120 patients with gastric cancer, who received surgical treatment at the First Hospital of Lanzhou University from March 2006 to December 2011. Paracarcinoma tissue referred to tissue more than 5 cm away from the cancer site, and pathologically confirmed as normal gastric mucosal tissue. The 120 gastric cancer patients (73 men and 47 women) had a definite pathology diagnosis as well as complete clinical data and follow-up information. Patients were between 32 and 75 years old with a mean age of 57.3 ± 14.5. Clinical stages of patients were judged according to the tumor-node-metastasis (TNM) staging system jointly formulated by the American Joint Committee on Cancer (AJCC) and Union for International Cancer Control (UICC). All patients with gastric cancer received no chemotherapy, radiotherapy, molecular targeted therapy or biological immunotherapy before the operation. After surgery, 86 gastric cancer patients received adjuvant chemotherapy. All patients gave informed consent, and the ethics committee of the First Hospital of Lanzhou University approved this study.
Immunohistochemistry analysis
An immunohistochemistry Elivision 2-step method (Maixin Biological, Fuzhou, China) was adopted. Paraffin specimens were cut into 4-μm sections and incubated at 60°C overnight. The specimens were deparaffinization and rehydrated, and endogenous peroxidase activity was inhibited by incubation with 3% hydrogen peroxide for 10 minutes at room temperature. After antigen retrieval using 0.01 mol/L of citrate buffer (pH 6.0), sections were incubated with rabbit-anti-human mannose receptor polyclonal antibodies (Sigma-Aldrich, St. Louis, MO, USA) with a dilution of 1:200 at 4°C overnight. Sections were washed, incubated with secondary antibodies for 10 minutes at 37°C, and then washed and incubated with horseradish peroxidase labeled streptavidin for 10 minutes at 37°C. After washes, 3,3-diaminobenzidine (DAB) development was monitored under a microscope. Staining was stopped with distilled water.
The sections were evaluated blindly by a pathologist. Five fields from a middle-power lens (×200) were randomly selected, and the percentage of staining in 200 tumor cells was counted in each field. The scores used for the staining intensity were 0 = nonstaining; 1 = light yellow staining; 2 = light brown staining and 3 = tan staining. Low expression was defined as a staining intensity score of either 0 or 1, and high expression was defined as a score of either 2 or 3.
Real-time PCR
The Trizol 1-step method was performed to extract total RNA. RNA integrity was tested by agarose gel electrophoresis (AGE), and an ultraviolet spectrophotometer was used to test purity and quantity. cDNA was synthesized from RNA, and polymerase chain reaction (PCR) was performed with the following conditions: 95°C for 3 minutes; 94°C for 45 seconds, 53°C for 45 seconds, 72°C for 1 minute, 35 cycles; 72°C for 5 minutes. The upstream primer for the mannose receptor was 5′-GACCTTGGACTGAGCAAAGGGG-3′; and the downstream primer was 5′-GACATGATGTCCTCAGGAGGACG-3′. GAPDH was used as internal reference. Electrophoretic gels were imaged in a RNA gel imaging scanner, and band absorbency was measured with Gel-Pro Analyzer 3.1 Software. Relative mRNA levels of mannose receptors were quantified using the formula: (band grayscale × area)/(grayscale of reference substance × area).
Statistical analysis
Patients were divided into 2 groups: low mannose receptor expression and high mannose receptor expression. Chi-square (χ 2 ) tests were performed to analyze the relationships between mannose receptor expression and clinicopathological parameters. The Kaplan-Meier method was performed for survival analysis, and the survival rates of the 2 groups were compared by log-rank tests. Overall survival (OS) and disease-free survival (DFS) were defined as primarily outcome. A Cox risk ratio model was applied to conduct combined effect analysis of various concomitant variables. SPSS Statistics 17.0 software was used for analysis. A p value <0.05 was taken to indicate significant differences.
Results
Mannose receptor expression in gastric cancer
Immunohistochemical analysis showed that mannose receptor staining was strong in the nucleus and cytoplasm of gastric cancer cells, weak in paracarcinoma tissue and negative in normal gastric mucosal tissue (Fig. 1). We divided patients into 2 groups: low expression and high expression of the mannose receptor. The high expression rate of mannose receptor protein in gastric cancer cells was 45.8% (54/120), significantly higher than that in the paracarcinoma tissue (20.0%, 36/120) (χ 2 = 6.286, p = 0.012). To further verify the results of immunohistochemistry, mRNA levels of mannose receptors were detected by real-time PCR (RT-PCR). We randomly selected 30 pairs of gastric cancer tissues and corresponding paracarcinoma tissues. In total, 19 of the 30 paired cases demonstrated a >twofold increase in the expression of mannose receptor mRNA in gastric cancer tissue compared with adjacent paracarcinoma tissue mucosa, and the highest increase in mannose receptor mRNA expression was 14.7-fold (Fig. 2).
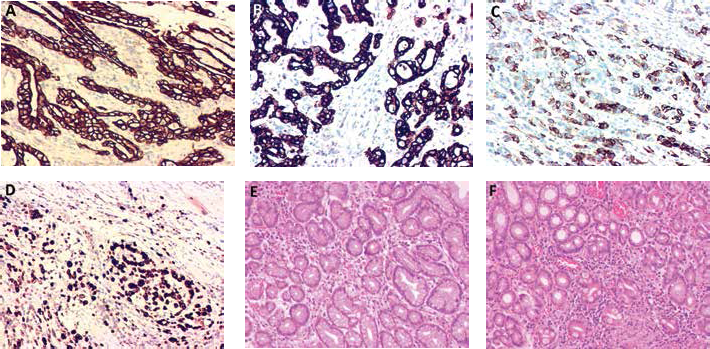
Immunohistochemical analysis of mannose receptor. (A, B) Gastric cancer tissues. (C, D) Adjacent paracarcinoma tissues. (E, F) Normal gastric mucosal tissues. Magnification: ×200.
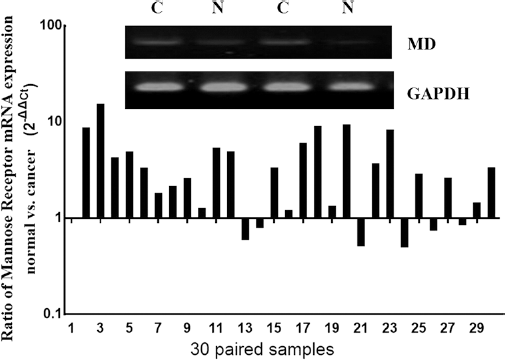
Real-time polymerase chain reaction (RT-PCR) analysis of mannose receptor mRNA levels. C = cancer tissue; MD = mannose receptor; N = paracarcinoma tissue.
Patient characteristics
Next we analyzed the relationship between mannose receptor protein and clinical and pathological characteristics of gastric cancer patients. We found that high expression of the mannose receptor was closely related to tumor size, T stage, N stage and UICC stage of gastric cancer (p<0.05). However, the age, sex, M stage, tumor location, Lauren classification, lymphovascular invasion and postsurgical chemotherapy of gastric cancer patients did not correlate with mannose receptor expression (p>0.05) (Tab. I).
Association between mannose receptor expression and clinicopathological features in patients with gastric cancer (n = 120)
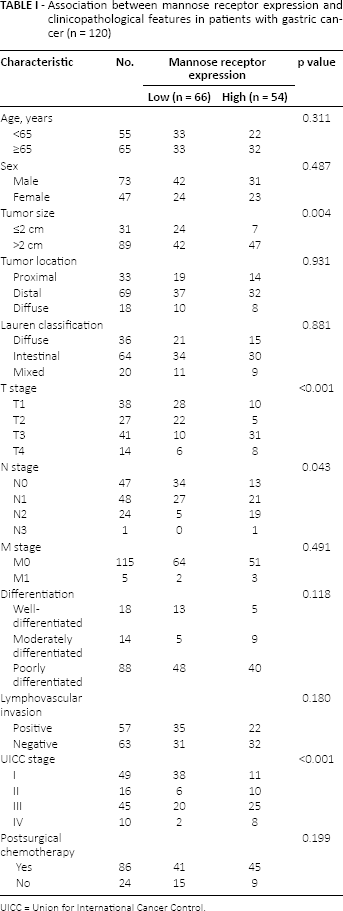
UICC = Union for International Cancer Control.
Expression of the mannose receptor and prognosis of gastric cancer patients
To ascertain the relationship between mannose receptor expression and prognosis of gastric cancer patients, we carried out a long-term follow-up for all patients and generated survival curves. The Kaplan-Meier survival model indicated that both DFS and OS of patients in the high-expression mannose receptor group were significantly shorter than in the low-expression mannose receptor group (Fig. 3). With a Cox risk ratio model, we analyzed each variable influencing DFS and OS of gastric cancer patients. Results of single factor analysis showed that prognosis of gastric cancer patients was closely associated with mannose receptor expression levels. Results of the multifactor analysis showed that high mannose receptor expression was an independent predictor for prognosis of patients with gastric cancer (Tab. II).
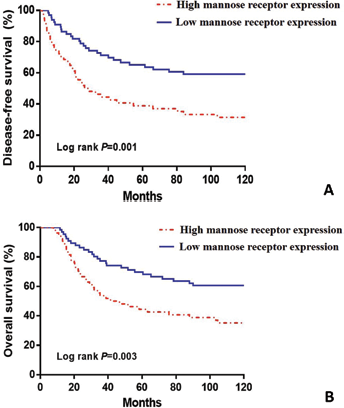
Kaplan-Meier survival curves for gastric cancer patients according to high or low mannose receptor expression status. (A) disease-free survival; (B) overall survival.
Univariate and multivariate analysis of variables affecting disease-free survival and overall survival after surgery
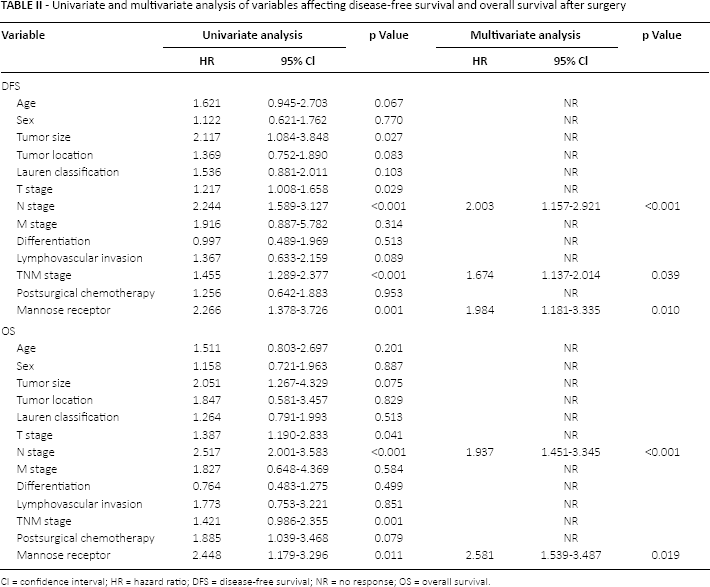
CI = confidence interval; HR = hazard ratio; DFS = disease-free survival; NR = no response; OS = overall survival.
Discussion
The mannose receptor is a 175-kDa Type I transmembrane protein receptor originally called the carbohydrate-recognition receptor (15). The mannose receptor has 5 structural domains: an extracellular structural domain including an N-terminal cysteine rich region (CR), a fibronectin type II domain (FN II), 8 C-typelectin-like domains (CTLD), a transmembrane region and a carboxy-terminal cysteine rich domain (16). The mannose receptor can identify and combine specific glucose molecules through the extracellular domain and has a high affinity for mannose (9, 15). Macrophages can express the mannose receptor, which plays an important role in infection, recognition, phagocytosis and removal of pathogens (17, 18). Tumor-associated macrophages (TAMs) could express the mannose receptor (18). Mutual crosslinking of tumor-like mucoprotein-mediated mannose receptors and infiltrated TAMs may cause an immune suppression state in macrophages leading to the growth of tumors (19, 20). We found no reports exploring the value of mannose receptor expression for the diagnosis or prognosis in gastric cancer patients.
In this study, we first examined the expression pattern of the mannose receptor in gastric cancer tissue using immunohistochemistry. We found that the mannose receptor was expressed in the cytoplasm or cell membranes of gastric cancer cells. By statistical analysis, mannose receptor protein showed high expression in gastric tumor tissues. However, mannose receptor staining was also positive in some paracarcinoma tissues. The reasons were unclear, but may indicate that these paracarcinoma tissues are undergoing the progression to gastric cancer.
Furthermore, we performed PCR to confirm that the level of mannose receptor mRNA in gastric cancer tissue was higher than in paracarcinoma tissue. We found that the expression levels of the mannose receptor were correlated with clinical pathological characteristics such as tumor size, T stage and TNM staging. Thus, the mannose receptor may promote growth, proliferation and invasion of gastric cancer tumor cells. In mannose receptor knockout mice, regional lymph node metastasis of tumors decreased significantly, indicating that blocking mannose receptors might inhibit tumor metastasis via lymph vessels (21, 22). Movahedi et al found that during anoxic conditions, the mannose receptor was highly expressed on the inner surface of tumor blood vessels, and targeted silencing of the mannose receptor could inhibit the growth of tumors (23). Keler et al utilized mannose receptors as targets to develop vaccines for tumor treatment (24, 25).
With long-term follow-up of the 120 gastric cancer patients, we found that patients with high expression of mannose receptor protein had shorter survival times, compared with patients with low expression. By multifactor regression analysis, high expression of the mannose receptor was shown to be one of the important independent indicators for predicting prognosis of gastric cancer patients. Therefore, we speculate that expression of the mannose receptor has a close relationship with the occurrence and development of gastric cancer and that the malignancy of gastric cancer might be positively correlated with mannose receptor expression.
Several limitations of this study should be noted. First, our sample size was relatively small. Second, we performed only retrospective analysis. Third, we did not include other potentially relevant prognostic factor in the multifactorial analysis. Further studies are needed to address these limitations.
In conclusion, high expression of the mannose receptor indicates poor prognosis for gastric cancer patients. Therefore, the mannose receptor is an important molecular marker to predict the prognosis of gastric cancer patients. However, further studies are needed to confirm our conclusion.
Footnotes
Financial support: This work was supported by grants from the Natural Science Foundation of Gansu province (number 145RJZA229).
Conflicts of interest: The authors report no conflicts of interest in this work.